Difference between revisions of "Colon"
(tweak) |
(→Microscopic colitis: rm spc) |
||
| Line 433: | Line 433: | ||
| pathoutlines = | | pathoutlines = | ||
}} | }} | ||
:''Microscopic colitis'' may refer to a microscopic manifestation of an unspecified disease process that can be apparent macroscopically. This section deals with a pair of diseases (''lymphocytic colitis'' and ''collagenous colitis'') that are considered to only have microscopic manifestations and characteristic clinical presentation. | :''Microscopic colitis'' may refer to a microscopic manifestation of an unspecified disease process that can be apparent macroscopically. This section deals with a pair of diseases (''lymphocytic colitis'' and ''collagenous colitis'') that are considered to only have microscopic manifestations and characteristic clinical presentation. | ||
===General=== | ===General=== | ||
Revision as of 08:19, 31 July 2013
The colon smells like poo... 'cause that's where poo comes from. This article also covers the rectum and cecum as both have a similar mucosa.
It commonly comes to pathologists because there is a suspicion of colorectal cancer or a known history of inflammatory bowel disease (IBD).
An introduction to gastrointestinal pathology is found in the gastrointestinal pathology article. The anus and ileocecal valve are dealt with in separate articles.
Technically, the rectum and cecum are not part of the colon. Thus, inflammation of the rectum should be proctitis and inflammation of the cecum should be cecitis.
Common clinical problems
Obstruction
Top three (in adults):[1]
- Neoplasia.
- Volvulus (cecal, sigmoid).
- Diverticular disease + stricture formation.
Bleeding
Mnemonic CHAND:[2]
- Colitis (radiation, infectious, ischemic, IBD (UC >CD), iatrogenic (anticoagulants)).
- Hemorrhoids.
- Angiodysplasia.
- Neoplastic.
- Diverticular disease.
Infectious colitis with bleeding - causes:
- Enterohemorrhagic Escherichia coli (EHEC) -- commonly 0157:H7.
- Campylobacter jejuni.
- Clostridium difficile.
- Shigella.
Infectious colitis in the immunosuppressed:
- Cytomegalovirus (CMV).[3]
Images:

CMV colitis - high. mag. (WC/Nephron)

CMV colitis - intermed. mag. (WC/Nephron)


Grossing
Types of specimens
Introduction to colorectal surgery:
- Colonic resection - remove a piece of large bowel.
- Total colectomy - leaves rectum and anus.[5]
- Subtotal colectomy - part of colon removed --or-- some of the rectum remains.
- Right hemicolectomy - right colon + distal ileum.
- Lower anterior resection (LAR) - proximal rectum +/- sigmoid (for proximal rectal malignancies).
- Specimens have should have intact mesorectum - total mesorectal excision (TME) - reduces local recurrence.[6]
- Abdominoperineal resection (APR) - anus + rectum - results in a permanent stoma (for distal rectal malignancies).
- Stoma - these are often done emergently and then get cut-out after the patient's condition has settled.
Images

APR specimen - anterior (WC)

APR specimen - lateral (WC)

APR specimen - inked (WC)



Identifying the specimen
- Transverse colon - has omentum.
- Ascending colon - usu. comes with ileocecal valve and a bit of ileum.
- Descending colon - has a bare area.
- Rectum - has adventitia.
Images
Sigmoid and rectum. APR specimen. (WC)
Lymph nodes
- One should get at least 12 lymph nodes if it is cancer.[9]
Quirke method
Standard method
- Bowel is prep'ed by opening it along the antimesenteric side.
- Dimensions - length, circumference at both margins.
- Radial margin/circumferential margin - should be painted.
- Rectum starts/sigmoid ends @ place where serosa ends on the posterior aspect of the bowel.
- The proximal, anterior aspect of the rectum has serosa, i.e. it is not painted.
- Rectum starts/sigmoid ends @ place where serosa ends on the posterior aspect of the bowel.
Common non-neoplastic disease
Colorectal polyps
Polyps are the bread & butter of GI pathology. They are very common.
Main types:
- Hyperplastic - most common, benign.
- Adenomatous - quite common, pre-malignant.
- Hamartomatous - rare, weird & wonderful.
- Inflammatory, AKA inflammatory pseudopolyps - associated with IBD.
Most common (images):
Hyperplastic polyp image - intermed. mag. (WC/Nephron)
Hyperplastic polyp image - low mag. (WC/Nephron)


Ischemic colitis
General
- May occur together with ischemic enteritis, in which case it is known as ischemic enterocolitis.
Etiology - anything that leads to vascular occlusion:
- Atherosclerosis.
- Vasculitis.
- Embolization, e.g. thrombotic, foreign body.
Possible associated pathology:
- Necrotizing enteritis - necrosis of the small bowel only.
- Necrotizing enterocolitis - necrosis of the small and large bowel.
Closely related:
Note:
- Ischemia = compromised blood supply.
Gross
Features - location:[12]
- Luminal part (mucosa & submucosa) affected - edema.
- Splenic flexture of colon commonly affected (vascular watershed).
Note:
- May have pseudomembranes (classically assoc. with C. difficile colitis), i.e. mimics an infectious process.
- DDx for pseudomembranes:[13]
- C. difficile induced pseudomembranous colitis.
- Ischemic colitis.
- Volvulus.
- Necrotizing infections.
- ... anything that causes severe mucosal injury.
- Radiologic correlate = bowel wall thickening.
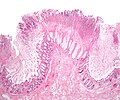
Microscopic
Features:
- Withering crypts - important.
- Colonic epithelium has decreased cytoplasm - NC ratio increased.
- Usually with decreased goblet cells.
- Crypt loss/drop-out.
- Less intestinal crypts present.
- Lamina propria hyalinization.
- Dense pink material replaces loose connective tissue.
- Submucosa hyalinization.
- +/-Pseudomembranes (microscopic):[13]
- Loss of surface epithelium.
- PMNs in lamina propria.
- +/-Capillary fibrin thrombi.
Note:
- Pseudomembranes arise from the crypts - considered acute.
DDx:
- Inflammatory bowel disease.
- Radiation colitis.
- Toxins/drugs.
- Infectious colitis.
Images

Ischemic colitis - low mag. (WC/Nephron)

Ischemic colitis - high mag. (WC/Nephron)

Ischemic colitis - very high mag. (WC/Nephron)
Colonic pseudomembranes - low mag. (WC/Nephron)
Colonic pseudomembranes - intermed. mag. (WC/Nephron)





www:
Sign out
Biopsy
TRANSVERSE COLON, BIOPSY: - SEVERE ACTIVE COLITIS WITH ATTENUATED EPITHELIAL CYTOPLASM AND ULCERATION. - CELLULAR DEBRIS. - NEGATIVE FOR DYSPLASIA AND NEGATIVE FOR MALIGNANCY. COMMENT: The attenuated cytoplasm is compatible with ischemia; however, it is not accompanied with other suggestive findings (crypt drop out, lamina propria fibrosis, pseudomembranes). The crypt architecture is test tube-like. The differential diagnosis includes: ischemia, drug reaction, infectious etiologies and, less likely, inflammatory bowel disease. Clinical correlation is required.
COLON, SPLENIC FLEXURE, BIOPSY: - PATCHY MODERATE ACTIVE COLITIS WITH ATTENUATED EPITHELIAL CYTOPLASM, FOCALLY DECREASED GOBLET CELLS AND ULCERATION. - NEGATIVE FOR DYSPLASIA AND NEGATIVE FOR MALIGNANCY. COMMENT: The findings are consistent with ischemia; however, they are not diagnostic. The differential diagnosis includes: ischemia, drug reaction, infectious etiologies and, less likely, inflammatory bowel disease. Clinical correlation is required.
Short version
LEFT COLON AND SIGMOID COLON, RESECTION: - PSEUDOMEMBRANOUS COLITIS, SEE COMMENT. - ONE LYMPH NODE NEGATIVE FOR MALIGNANCY ( 0 POSITIVE / 1 ). - NEGATIVE FOR DYSPLASIA AND NEGATIVE FOR MALIGNANCY. COMMENT: Pseudomembrane formation is a non-specific finding. It is consistent with ischemia; however, it may be seen in other contexts, including infection. Clinical correlation is required.
Long version
RECTOSIGMOID, RESECTION: - BOWEL WALL ISCHEMIA WITH PERFORATION, SEROSITIS, MICROABSCESS FORMATION AND FOCAL POORLY FORMED PSEUDOMEMBRANES. - NEGATIVE FOR MALIGNANCY. - PLEASE SEE COMMENT. COMMENT: There is no evidence of inflammatory bowel disease: The unaffected mucosa does not have obvious architectural distortion. No granulomas are identified. The inflammation is largely associated with necrosis/ischemic changes and favoured to be reactive. The poorly formed pseudomembranes are associated with mural ischemic changes; they do not specifically suggest an infection in this context. The blood vessels do not show a vasculitis, or significant atherosclerosis. Thrombi are seen on several sections and found predominantly in the (smaller) veins. Considerations are thrombosis, thromboembolism, mechanical vascular compromise, and infectious etiologies. A vascular compromise is favoured as the underlying cause. Clinical and radiologic correlation is suggested.
Another long version
SIGMOID COLON, RESECTION: - BOWEL WALL ISCHEMIA WITH PERFORATION, SEROSITIS, AND FOCAL POORLY FORMED PSEUDOMEMBRANES. - MILD ATHEROSCLEROSIS. - DIVERTICULAR DISEASE. - TWO LYMPH NODES NEGATIVE FOR MALIGNANCY ( 0 POSITIVE / 2 ). - PLEASE SEE COMMENT. COMMENT: The sections show the changes of acute and chronic ischemic colitis (submucosal fibrosis, lamina propria hyalinization, focal crypt drop-out, decreased goblet cells, pigmented macrophages in the lamina propria, intraepithelial neutrophils). No granulomas are identified. The inflammation is largely associated with the necrosis/ischemic changes and favoured to be reactive. The poorly formed pseudomembranes are associated with mural ischemic changes; they do not specifically suggest an infectious etiology in this context. The blood vessels do not show a vasculitis. However, focal neutrophilic perivascular inflammation is seen; this is probably a reactive process. No vascular thrombi are identified. The findings are compatible with perforation secondary to a foreign body in the setting of chronic ischemia.
Micro
Negative for ischemic colitis
The sections show colorectal mucosa with preservation of the crypt density and epithelium with a normal nuclear-to-cytoplasm ratio. There is no apparent lamina propria hyalinization. The muscularis mucosa is prominent. Focally, lymphoid aggregates are present.
No cryptitis is present. Neutrophils are not apparent in the lamina propria. No erosions are identified.
The epithelium matures appropriately from the crypt base to the surface.
Diverticular disease
- Diverticulitis redirect here.
- AKA diverticulosis.
General
- Very common.
Complications:
- Diverticulitis.
- Diverticular-associated colitis[17] - rare.
- Rectal biopsy to differentiate from ulcerative colitis.
Gross
- Corrugated - like cardboard.
- Wall thickening (reactive).[18]
Endoscopic image

Diverticular disease. (WC/Samir)

Grossing notes
Microscopic
Features:
- Mucosa/submucosa invagination into the musuclaris propria (MP).
- At the site the blood vessels supplying the mucosa and submucosa penetrate the MP.[19]
Image:
Sign out
RECTO-SIGMOID, LARGE BOWEL RESECTION: - PERFORATED DIVERTICULITIS WITH SEROSITIS AND ABSCESS FORMATION. - SUBMUCOSAL FIBROSIS. - ONE LYMPH NODE NEGATIVE FOR MALIGNANCY ( 0 POSITIVE / 1 ). - NEGATIVE FOR MALIGNANCY.
SIGMOID COLON, SIGMOIDECTOMY: - DIVERTICULAR DISEASE WITHOUT DIVERTICULITIS. - NEGATIVE FOR MALIGNANCY.
Pseudomembranous colitis
General
- Pseudomembranous colitis is a histomorphologic description which has a DDx. In other words, it can be caused by a number of things.
DDx of pseudomembranous colitis:[13]
- C. difficile.
- Known as C. difficile colitis.
- Ischemic colitis.
- Volvulus.
- Other infections.
Etiology:
- Anything that causes a severe mucosal injury.
Gross
Features:[21]
- Pseudomembranes:
- Pale yellow (or white) irregular, raised mucosal lesions.
- Early lesions: typical <10 mm.
- Interlesional mucosa often near normal grossly.
Images:

Pseudomembranous colitis (WC/Nephron)

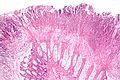
Microscopic
Features:[13]
- Heaped necrotic surface epithelium.
- Described as "volanco lesions" - this is what is seen endoscopically.
- PMNs in lamina propria.
- +/-Capillary fibrin thrombi.
Notes:
- Pseudomembranes arise from the crypts.
- Rarely have (benign) signet ring cell-like cells.[22]
Images
Pseudomembranes - low mag. (WC/Nephron)
Pseudomembranes - intermed. mag. (WC/Nephron)
www:
Volvulus
General
- Uncommonly comes to pathology.
- It is essentially a radiologic diagnosis.
- In the context of autopsy, it is a gross diagnosis.
Gross
- Intestine folded over itself - typically leads to ischemia.
Images:
Microscopic
Features:
- +/-Ischemic changes and/or necrosis.
DDx - essentially anything that causes ischemia:
- Embolus.
- Thrombosis.
- Vasculitis.
Sign out
RECTOSIGMOID, RESECTION: - MURAL ISCHEMIA WITH PERFORATION, SEROSITIS, MICROABSCESS FORMATION AND POORLY FORMED PSEUDOMEMBRANES. - SUBMUCOSAL FIBROSIS. - NEGATIVE FOR MALIGNANCY. COMMENT: The findings are consistent with volvulus and the submucosal fibrosis suggests this may have been recurrent.
Inflammatory diseases
Inflammatory bowel disease
The bread 'n butter of gastroenterology. A detailed discussion of IBD is in the inflammatory bowel disease article. It comes in two main flavours (Crohn's disease, ulcerative colitis).
Microscopic
Features helpful for the diagnosis of IBD - as based on a study:[24]
- Basal, i.e. crypt base, plasmacytosis with severe chronic inflammation,
- Crypt architectural abnormalities, and
- Distal Paneth cell metaplasia.
Microscopic colitis
| Lymphocytic colitis | |
|---|---|
| External resources | |
| EHVSC | 10184 |
- Microscopic colitis may refer to a microscopic manifestation of an unspecified disease process that can be apparent macroscopically. This section deals with a pair of diseases (lymphocytic colitis and collagenous colitis) that are considered to only have microscopic manifestations and characteristic clinical presentation.
General
Presentation:
- Chronic diarrhea, non-bloody.[27]
Notes:
- Clinical DDx includes irritable bowel syndrome - which has no or subtle histopathologic changes.
Classification
- Lymphocytic colitis (LC).
- Collagenous colitis (CC).
Note:
- Some believe that LC and CC are different time points in the same process-- but this is unproven.[27]
Epidemiology
- Age: a disease of adults - usually 50s.
- Sex:
- Drugs are associated with LC and CC.
- NSAIDs - posulated association/weak association,
- SSRIs (used primarily for depression) - moderate association, dependent on specific drug.
- Associated with autoimmune disorders - celiac disease, diabetes mellitus, thyroid disorders and arthritis.[28]
- No increased risk of colorectal carcinoma.[28]
Treatment
- Sometimes just follow-up.
- Steroids - budesonide -- short-term treatment.[28]
Gross
- As the name suggests, they are microscopic, i.e. endoscopic examination is normal.
Microscopic
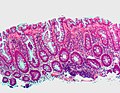
Lymphocytic colitis
Features:
- Lots of intraepithelial lymphocytes (>=20/100 lymphocytes/surface epithelial cells[28]) and
- Lymphocytes in the lamina propria.
Significant negatives:[29]
- No neutrophils.
- No crypt distortion.
DDx:
- Infectious colitis - neutrophils present... not lymphocytes.
- Collagenous colitis - has a band of collagen below the epithelium.
Image:
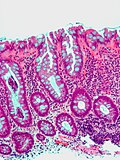
Collagenous colitis
Features:
- Intraepithelial lymphocytes - important.
- Collagenous material in the lamina propria (pink on H&E) -- key feature.
- Can be demonstrated with a trichrome stain -- collagen = green on trichrome.
- Subepithelial collagen needs to be >= 10 micrometres thick for diagnosis.[28]
- Thickening is usually patchy.[31]
- Thickening "follows the crypts from the surface" - useful for differentiating from tangential sections of the basement membrane.[32]
- Collagen may envelope capillaries - useful to discern from basement membrane.[32]
Notes:
- CC is typically more prominent in the proximal colon - may reflect concentration gradient of offending causitive agents.[28]
- Significant negative findings:[29]
- No PMNs.
- No crypt distortion.
- Thickened collagen band uncommon in rectum.[31]
Images

CC - intermed mag. (WC/Nephron)

CC - high mag. (WC/Nephron)


Sign out
TRANSVERSE COLON, BIOPSY: - COLLAGENOUS COLITIS.
ASCENDING COLON, BIOPSY: - LYMPHOCYTIC COLITIS.
Micro
Lymphocytic colitis
The sections show colonic mucosa with abundant intraepithelial lymphocytes (>20 lymphocytes/100 surface epithelial cells). The glandular architecture is within normal limits. No thickened collagen band is apparent below the epithelium.
There are no granulomas. No neutrophilic cryptitis is apparent. The epithelium matures appropriately to the surface.
Collagenous colitis
The sections show colonic mucosa with abundant intraepithelial lymphocytes (>20 lymphocytes/100 surface epithelial cells). A prominent collagen band is apparent below the epithelium (>10 micrometres thick). The glandular architecture is within normal limits.
There are no granulomas. No neutrophilic cryptitis is apparent. The epithelium matures appropriately to the surface.
Diversion colitis
- Diversion proctitis redirect here.
General
- Segment of de-functioned bowel due to surgical diversion, i.e. stoma (ileostomy or colostomy).
- Diagnosis dependent on history - key point.
Gross
Features:[33]
- Ulceration - classic.
- Surgical changes, e.g. fibrotic-appearing thickened wall.
- May not be apparent.
Microscopic
Features:[33]
- Follicular lymphoid hyperplasia - key feature.[34]
- Abundant lymphoid nodules.
- Plasma cells and lymphocytes.
- +/-Changes of an active colitis - uncommon:[35]
- Cryptitis.
- Crypt abscesses.
Notes:
- May show IBD-like changes.[36]
- IBD should not be diagnosed on a diverted segment of bowel.
DDx:[37]
- Inflammatory bowel disease - no stoma.
- Ischemic colitis.
- Infectious colitis.
Images

Diversion proctitis - low mag. (WC/Nephron)

Diversion proctitis - high mag. (WC/Nephron)


Sign out
SIGMOID COLON, BIOPSIES: - MILD ACTIVE COLITIS WITH LAMINA PROPRIA FIBROSIS, SEE COMMENT. - NEGATIVE FOR DYSPLASIA. COMMENT: No granulomas are identified. Follicular lymphoid hyperplasia is not identified; however, there is no definite submucosa present. Diverted segments of bowel can have inflammatory bowel disease-like changes. In the context of a diverted segment of bowel, the findings are compatible with a diversion colitis.
Eosinophilic colitis
General
- Rare.
- May be a component of eosinophilic gastroenteritis.[38]
Clinical features:[38]
- Abdominal pain
- Diarrhea +/-blood.
- +/-Weight loss.
Gross
Features - endoscopic:[38]
- Edema.
- Granular appearance.
Microscopic
Features:[38]
- Abundant eosinophils - no agreed upon number.
DDx:[38]
- Inflammatory bowel disease:
- Infection:
- Autoimmune disease:
- Drug reactions.
Image:
Sign out
DESCENDING COLON, BIOPSY: - COLONIC MUCOSA WITH MILD EOSINOPHILIA, SEE COMMENT. - NEGATIVE FOR DYSPLASIA. COMMENT: Focally, there are up to 40 eosinophils / 0.2376 mm*mm (approx. field area at 400X). This is a non-specific finding. No eosinophilic crypt abscesses are seen. No (neutrophilic) cryptitis is present. Clinical correlation is suggested.
DESCENDING COLON, BIOPSY: - COLONIC MUCOSA WITH MILD EOSINOPHILIA, SEE COMMENT. - NEGATIVE FOR ACTIVE COLITIS. - NEGATIVE FOR DYSPLASIA. COMMENT: There are up to 40 eosinophils / 0.2376 mm*mm (field area at 400X). This is a non-specific finding. The differential diagnosis includes inflammatory bowel disease, infection (especially helminths), a drug reaction, and autoimmune disorders (e.g. Churg-Strauss syndrome, celiac disease, scleroderma). Clinical correlation is required.
Infectious
Infectious colitis
- This section covers non-specific colitides that appear to have an infective etiology.
General
- Common.
- Diarrhea - typical symptom.
Gross
- +/-Erythema on endoscopy.
Microscopic
Features:
- Neutrophils predominant - key feature.[40]
- The neutrophils are often superficial - they go to were the bad guys are.
- No architectural distortion - if acute.
DDx:
- Inflammatory bowel disease - lymphoplasmacytic infiltrate predominant,[40] usually has chronic changes.
- Ischemic colitis.
- Medications - focal neutrophils.
- Lymphocytic colitis - lymphocytes with a squiggly nucleus, may be confused with neutrophils.
- Specific causes of infective colitis - with a distinctive morphology.
- CMV colitis - esp. in the immunodeficient.
- Pseudomembranous colitis - usu. due to C. difficle, has characteristic gross & microscopic appearance.
- Intestinal spirochetes.
- Amebiasis.
- Strongyloidiasis.
- Cryptosporidiosis.
IHC
Done if the patient is immunosuppressed, or there is clinical or morphological suspicion:
Sign out
ASCENDING COLON, BIOPSY: - MILD ACTIVE COLITIS, SEE COMMENT. COMMENT: There is are no granulomas. The crypt architecture is normal. A benign lymphoid nodule is present. The differential diagnosis includes infective etiologies, early inflammatory bowel disease and ischemia. The histomorphology is more in keeping with an infective etiology as neutrophils are a predominant feature; however, clinical correlation is required.
Cytomegalovirus colitis
- Abbreviated CMV colitis.
General
- Uncommon.
- Immunosuppressed population at risk, e.g. transplant recipients, individuals with HIV.
Microscopic
Features:
- Enlarged nucleus - classically in endothelial cells.
DDx:
- Infectious colitis without a distinctive morphology.
- CMV colitis superimposed on inflammatory bowel disease.
Images
CMV colitis - intermed. mag. (WC/Nephron)
CMV colitis - high mag. (WC/Nephron)
IHC
- CMV +ve.
Others:
- HSV-1.
- HSV-2.
- VZV.
- EBV.
Intestinal spirochetosis
- AKA intestinal spirochetes; more specifically colonic spirochetes, colonic spirochetosis.
General
- Caused by spirochetes[42][43] - specifically Brachyspira piloicoli[44] (previously Serpulina pilosicoli[45]) and Brachyspira aalborgi.
- Very rare cause of diarrhea, associated with male homosexual behaviour.
Symptoms:[43]
- Watery diarrhea, abdominal pain, +/-blood per rectum.
Treatment:[46]
- Metronidazole.
Microscopic
Features:
- Hyperchromatic fuzz on luminal aspect of epithelial cells; at brush border.
DDx:
- Normal colon.
- Infectious colitis without a distinctive morphology.
Images

Intestinal spirochetes - cropped - very high mag. (WC/Nephron)

Intestinal spirochetes - very high mag. (WC/Nephron)

Intestinal spirochetes - intermed. mag. (WC/Nephron)



www:
Special stains
- Silver stains highlight 'em (e.g. Warthin-Starry stain).
Amebiasis
- May also be spelled amoebiasis.
General
- Infection with Entamoeba histolytica.[47]
- May mimic colon cancer.[48]
May cause:[49]
- Dysentery (diarrhea containing mucus and/or blood in the feces).
- Colitis.
- Liver abscess.
Microscopic
Features:
- Entamoeba histolytica are round/ovoid eosinophilic bodies ~ 40-60 micrometers in maximal dimension.
- Found in bowel lumen.
- Ingest RBCs.
Image

Amebiasis - very high mag. (WC/Nephron)
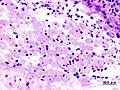
Amebiasis (WC)

.jpg)
Cryptosporidiosis
General
- Usually in immune incompetent individuals, e.g. HIV/AIDS.
Microscopic
Features:
- Uniform spherical nodules 2-4 micrometres in diameter, typical location - GI tract brush border.
- Bluish staining of brush border key feature - low power.
Rectal pathology
Solitary rectal ulcer
- AKA solitary ulcer syndrome of the rectum, abbreviated SUS.
- AKA solitary rectal ulcer syndrome.
- Mucosal prolapse syndrome may be used as a synonym; however, it encompasses other entities.[50]
General
- Clinically may be suspected to a malignancy - biopsied routinely.
- Mucosal ulceration.
- "Three-lies disease":[51]
- May not be solitary.
- May not be rectal -- can be in left colon.
- May not be ulcerating -- non-ulcerated lesions: polypoid and/or erythematous.
Note: Each of the words in solitary rectal ulcer is a lie.
Epidemiology
- Typically younger patients - average age of presentation ~30 years in one study.[52]
- Rare.
Clinical presentation
- Usually presents as BRBPR ~ 85% of cases.[52]
- Abdominal pain present in approx. 1/3.[52]
- May be very painful.
Treatment:
- Usually conservative, i.e. non-surgical.
- Resection - may be done for fear of malignancy.
Gross
- Classically, anterior or anterolateral wall of the rectum.[51]
Microscopic
- Fibrosis of the lamina propria.
- Thickened muscularis mucosa with abnormal extension to the lumen.
- +/-Mucosa ulceration.
- +/-Submucosal fibrosis.
DDx:
- Inflammatory pseudopolyp (inflammatory polyp).
- Associated with inflammatory bowel disease.
- Rectal prolapse.
- Well-differentiated adenocarcinoma.
IHC
- p53 -ve.
- May be used to help exclude adenocarcinoma.
Rectal prolapse
General
Microscopic
Features:[55]
- "Fibromuscular hyperplasia" - key feature:
- Fibrosis (submucosa, lamina propria).
- Muscularis mucosae is "too superficial" (muscle in the lamina propria).
- Surface ulceration + inflammation (neutrophils).
- +/-Serration of epithelium at the surface.
Notes:
- Important negative: no nuclear atypia.
Images

Rectal prolapse - low mag. (WC/Nephon)

Rectal prolapse - intermed. mag. (WC/Nephron)


Neoplastic disease
Colorectal Tumours
These are very common. The are covered in a separate article entitled colorectal tumours.
Neuroendocrine tumour
- AKA carcinoid.
Goblet cell carcinoid
- Described in detail in the appendix article.
- AKA crypt cell carcinoma.
- Biphasic tumour; features of carcinoid tumour and adenocarcinoma.
Other
Pseudomelanosis coli
- AKA melanosis coli.[56]
General
- Not melanin as the name melanosis coli suggests; it is actually lipofuscin (in macrophages).[57]
- Endoscopist may see brown pigmentation of mucosa and suspect the diagnosis.
- Presence may lead to endoscopic misinterpretation of colitis severity.[58]
Epidemiology
- Classically associated with anthracene containing laxative (e.g. Senokot) use and herbal remedies.[57]
- May be seen in individuals not using laxatives.[59]
- Seen in (long-standing) inflammatory bowel disease, especially ulcerative colitis.[59]
Gross
- Brown pigmentation of the mucosa, esp. cecum and proximal colon.
Image

Melanosis coli - endoscopic image (WC)

Microscopic
Features:
- Brown granular pigment - in the lamina propria.
- Typically more prominent in the cecum and proximal colon.[57]
Notes:
- DDx of brown pigment:
- Lipofuscin - comes with age (can be demonstrated with a PAS stain[60] or Kluver-Barrera stain[61]).
- Melanosis coli.
- Old haemorrhage, i.e. hemosiderin-laden macrophages (may be demonstrated with Prussian blue stain[62]).
- Melanin (from melanocytes) - rare in colon (may be demonstrated with a Fontana-Masson stain[63] -- though not so useful in the GI tract).
- Foreign material (e.g. tattoo pigment) - not seen in GI tract.
- Lipofuscin - comes with age (can be demonstrated with a PAS stain[60] or Kluver-Barrera stain[61]).
Images

Melanosis coli - high mag. (WC/Nephron)

Melanosis coli - low mag. (WC/Nephron)


Stains
Sign out
ASCENDING COLON, BIOPSY: - PSEUDOMELANOSIS COLI. - NEGATIVE FOR ACTIVE COLITIS. - NEGATIVE FOR DYSPLASIA.
Angiodysplasia
General
- Causes (lower) GI haemorrhage.
- Generally, not a problem pathologists see.
- May be associated with aortic stenosis; known as Heyde syndrome.[65]
Epidemiology:
- Older people.
Etiology:
- Thought to be caused by the higher wall tension of cecum (due to larger diameter) and result from (intermittent) venous occlusion/focal dilation of vessels.[66]
Gross
- Cecum - classic location.
Note:
- Crohn's disease - may mimic angiodysplasia radiographically.[67]
Microscopic
Features:[67]
- Dilated vessels in mucosa and submucosa.
Drugs
Sodium polystyrene sulfonate
- AKA Kayexalate.
General
- Used to treat hyperkalemia - as may be seen in renal failure.
Microscopic
Features:[68]
- Purple blobs on H&E stain - look somewhat like calcium phosphate.
- Can cause focal necrosis.
Image
Adenocarcinoma and sodium polystyrene crystals (WC/Nephron)

{kind=link}
{kind=link}
{kind=link}
Graft-versus host disease
- Abbreviated as GVHD.
- Seen in the context of bone marrow transplants.
Bowel transplant
The histology of bowel transplant rejection is identical to GVHD - see GVHD.
Chronic constipation
- This section deals with chronic constipation that has no apparent cause.
General
General differential diagnosis for constipation:
- Tumour.
- Adhesions - due to previous surgery.
- Neuropathy.[69]
- Congenital defect (Hirschsprung's disease).
- Myopathy.[69]
- Medications/substance use.
- Idiopathic.
Gross
- No changes.
Microscopic
Features:
- Colon within normal limits.
- Look for the Ganglion cells (submucosal plexus, myenteric plexus).
- Look for interstitial cells of Cajal (with CD117) - typically most common around the myenteric plexus.[70]
Negatives:
- No significant vascular disease.
- No fibrosis.
- No loss of muscle.
Stains & IHC
Work-up if no tumour is identified:[71][72]
- Routine H&E.
- Smooth muscle actin - confirm myocyte loss.
- Gomori trichrome - examine connective tissue.
- CD117 - to look for the interstitial cells of Cajal.
- <50% the expected = abnormal.[72]
- Normal numbers not defined.
- <50% the expected = abnormal.[72]
- HU - neuronal marker.[73]
Sign out
- A long list of things to report is contained the recommendation of a working group.[72]
- Most pathology practises do not report much.
TERMINAL ILEUM, CECUM, COLON (ASCENDING, TRANSVERSE AND SIGMOID), COLECTOMY: - SMALL BOWEL, CECUM, AND COLON WITHIN NORMAL LIMITS. - FOUR LYMPH NODES NEGATIVE FOR MALIGNANCY ( 0 POSITIVE / 4 ). - NEGATIVE FOR DYSPLASIA AND NEGATIVE FOR MALIGNANCY. COMMENT: Several stains were done: CD117: interstitial cells of Cajal present, no apparent decrease. SMA: no significant myocyte loss. Gomori trichrome: no abnormal fibrosis apparent. Tau: no abnormalities apparent.
See also
References
- ↑ URL: http://www.emedicine.com/EMERG/topic65.htm. Accessed on: 28 June 2011.
- ↑ TN 2007 G29.
- ↑ Golden MP, Hammer SM, Wanke CA, Albrecht MA (September 1994). "Cytomegalovirus vasculitis. Case reports and review of the literature". Medicine (Baltimore) 73 (5): 246–55. PMID 7934809.
- ↑ Kandiel A, Lashner B (December 2006). "Cytomegalovirus colitis complicating inflammatory bowel disease". Am. J. Gastroenterol. 101 (12): 2857–65. doi:10.1111/j.1572-0241.2006.00869.x. PMID 17026558.
- ↑ http://www.allaboutbowelsurgery.com/shared/stoma_care/stoma_surgery/procedures/surgery_colon/subtotal.htm
- ↑ Arbman, G.; Nilsson, E.; Hallböök, O.; Sjödahl, R. (Mar 1996). "Local recurrence following total mesorectal excision for rectal cancer.". Br J Surg 83 (3): 375-9. PMID 8665198.
- ↑ Lester, Susan Carole (2010). Manual of Surgical Pathology (3rd ed.). Saunders. pp. 339. ISBN 978-0-323-06516-0.
- ↑ URL: http://www.bartleby.com/107/249.html. Accessed on: 19 October 2012.
- ↑ Bilimoria KY, Bentrem DJ, Stewart AK, et al. (September 2008). "Lymph node evaluation as a colon cancer quality measure: a national hospital report card". J. Natl. Cancer Inst. 100 (18): 1310–7. doi:10.1093/jnci/djn293. PMID 18780863. http://www.medscape.com/viewarticle/581463.
- ↑ West NP, Morris EJ, Rotimi O, Cairns A, Finan PJ, Quirke P (September 2008). "Pathology grading of colon cancer surgical resection and its association with survival: a retrospective observational study". Lancet Oncol. 9 (9): 857–65. doi:10.1016/S1470-2045(08)70181-5. PMID 18667357.
- ↑ West NP, Finan PJ, Anderin C, Lindholm J, Holm T, Quirke P (July 2008). "Evidence of the oncologic superiority of cylindrical abdominoperineal excision for low rectal cancer". J. Clin. Oncol. 26 (21): 3517–22. doi:10.1200/JCO.2007.14.5961. PMID 18541901.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 852. ISBN 0-7216-0187-1.
- ↑ 13.0 13.1 13.2 13.3 Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 837-8. ISBN 0-7216-0187-1.
- ↑ Tan, J.; Pretorius, CF.; Flanagan, PV.; Pais, A. (2012). "Adverse drug reaction: rosuvastatin as a cause for ischaemic colitis in a 64-year-old woman.". BMJ Case Rep 2012. doi:10.1136/bcr.11.2011.5270. PMID 22744258.
- ↑ Fabra, I.; Roig, JV.; Sancho, C.; Mir-Labrador, J.; Sempere, J.; García-Ferrer, L. (Jan 2011). "[Cocaine-induced ischemic colitis in a high-risk patient treated conservatively].". Gastroenterol Hepatol 34 (1): 20-3. doi:10.1016/j.gastrohep.2010.10.005. PMID 21237534.
- ↑ Appu, S.; Thompson, G. (Nov 2001). "Gangrenous ischaemic colitis following non-steroidal anti-inflammatory drug overdose.". ANZ J Surg 71 (11): 694-5. PMID 11736840.
- ↑ Mulhall, AM.; Mahid, SS.; Petras, RE.; Galandiuk, S. (Jun 2009). "Diverticular disease associated with inflammatory bowel disease-like colitis: a systematic review.". Dis Colon Rectum 52 (6): 1072-9. doi:10.1007/DCR.0b013e31819ef79a. PMID 19581849.
- ↑ Nicholson, BD.; Hyland, R.; Rembacken, BJ.; Denyer, M.; Hull, MA.; Tolan, DJ. (Aug 2011). "Colonoscopy for colonic wall thickening at computed tomography: a worthwhile pursuit?". Surg Endosc 25 (8): 2586-91. doi:10.1007/s00464-011-1591-7. PMID 21359889.
- ↑ West, AB.. "The pathology of diverticulitis.". J Clin Gastroenterol 42 (10): 1137-8. doi:10.1097/MCG.0b013e3181862a9f. PMID 18936652.
- ↑ URL: http://histology-group28.wikispaces.com/DigestiveSystemProject. Accessed on: 23 August 2011.
- ↑ URL: http://radiology.uchc.edu/eAtlas/GI/1749.htm. Accessed on: 22 May 2012.
- ↑ Abdulkader, I.; Cameselle-Teijeiro, J.; Forteza, J. (Apr 2003). "Signet-ring cells associated with pseudomembranous colitis.". Virchows Arch 442 (4): 412-4. doi:10.1007/s00428-003-0779-1. PMID 12684766.
- ↑ URL: http://pathsrvr.rockford.uic.edu/inet/GI/GI%20Station%201.htm. Accessed on: 9 April 2012.
- ↑ Tanaka M, Riddell RH, Saito H, Soma Y, Hidaka H, Kudo H (January 1999). "Morphologic criteria applicable to biopsy specimens for effective distinction of inflammatory bowel disease from other forms of colitis and of Crohn's disease from ulcerative colitis". Scand. J. Gastroenterol. 34 (1): 55–67. PMID 10048734.
- ↑ Tanaka M, Saito H, Kusumi T, et al (December 2001). "Spatial distribution and histogenesis of colorectal Paneth cell metaplasia in idiopathic inflammatory bowel disease". J. Gastroenterol. Hepatol. 16 (12): 1353–9. PMID 11851832. http://www3.interscience.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=0815-9319&date=2001&volume=16&issue=12&spage=1353.
- ↑ Rubio CA, Nesi G (2003). "A simple method to demonstrate normal and metaplastic Paneth cells in tissue sections". In Vivo 17 (1): 67–71. PMID 12655793.
- ↑ 27.0 27.1 27.2 27.3 URL: http://emedicine.medscape.com/article/180664-overview. Accessed on: 31 May 2010.
- ↑ 28.0 28.1 28.2 28.3 28.4 28.5 28.6 28.7 Tysk C, Bohr J, Nyhlin N, Wickbom A, Eriksson S (December 2008). "Diagnosis and management of microscopic colitis". World J. Gastroenterol. 14 (48): 7280-8. PMID 19109861. http://www.wjgnet.com/1007-9327/14/7280.asp. Cite error: Invalid
<ref>tag; name "pmid19109861" defined multiple times with different content - ↑ 29.0 29.1 http://hopkins-gi.nts.jhu.edu/pages/latin/templates/index.cfm?pg=disease1&disease=29&organ=6&lang_id=1
- ↑ Offner, FA.; Jao, RV.; Lewin, KJ.; Havelec, L.; Weinstein, WM. (Apr 1999). "Collagenous colitis: a study of the distribution of morphological abnormalities and their histological detection.". Hum Pathol 30 (4): 451-7. PMID 10208468.
- ↑ 31.0 31.1 Tanaka, M.; Mazzoleni, G.; Riddell, RH. (Jan 1992). "Distribution of collagenous colitis: utility of flexible sigmoidoscopy.". Gut 33 (1): 65-70. PMID 1740280.
- ↑ 32.0 32.1 Bell, D. 4 Mar 2009.
- ↑ 33.0 33.1 Edwards, CM.; George, B.; Warren, B. (Jan 1999). "Diversion colitis--new light through old windows.". Histopathology 34 (1): 1-5. PMID 9934577.
- ↑ Yeong, ML.; Bethwaite, PB.; Prasad, J.; Isbister, WH. (Jul 1991). "Lymphoid follicular hyperplasia--a distinctive feature of diversion colitis.". Histopathology 19 (1): 55-61. PMID 1916687.
- ↑ Ma, CK.; Gottlieb, C.; Haas, PA. (Apr 1990). "Diversion colitis: a clinicopathologic study of 21 cases.". Hum Pathol 21 (4): 429-36. PMID 2318485.
- ↑ Yantiss, RK.; Odze, RD. (Jan 2006). "Diagnostic difficulties in inflammatory bowel disease pathology.". Histopathology 48 (2): 116-32. doi:10.1111/j.1365-2559.2005.02248.x. PMID 16405661.
- ↑ Thorsen, AJ. (Feb 2007). "Noninfectious colitides: collagenous colitis, lymphocytic colitis, diversion colitis, and chemically induced colitis.". Clin Colon Rectal Surg 20 (1): 47-57. doi:10.1055/s-2007-970200. PMC 2780148. PMID 20011361. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2780148/.
- ↑ 38.0 38.1 38.2 38.3 38.4 Alfadda, AA.; Storr, MA.; Shaffer, EA. (2011). "Eosinophilic colitis: an update on pathophysiology and treatment.". Br Med Bull 100: 59-72. doi:10.1093/bmb/ldr045. PMC 3165205. PMID 22012125. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3165205/.
- ↑ 39.0 39.1 39.2 Okpara, N.; Aswad, B.; Baffy, G. (Jun 2009). "Eosinophilic colitis.". World J Gastroenterol 15 (24): 2975-9. PMC 2702104. PMID 19554649. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2702104/. Cite error: Invalid
<ref>tag; name "pmid19554649" defined multiple times with different content - ↑ 40.0 40.1 Iacobuzio-Donahue, Christine A.; Montgomery, Elizabeth A. (2005). Gastrointestinal and Liver Pathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 324. ISBN 978-0443066573.
- ↑ Karlitz, JJ.; Li, ST.; Holman, RP.; Rice, MC. (Jan 2011). "EBV-associated colitis mimicking IBD in an immunocompetent individual.". Nat Rev Gastroenterol Hepatol 8 (1): 50-4. doi:10.1038/nrgastro.2010.192. PMID 21119609.
- ↑ Amat Villegas I, Borobio Aguilar E, Beloqui Perez R, de Llano Varela P, Oquiñena Legaz S, Martínez-Peñuela Virseda JM (January 2004). "[Colonic spirochetes: an infrequent cause of adult diarrhea]" (in Spanish; Castilian). Gastroenterol Hepatol 27 (1): 21–3. PMID 14718105.
- ↑ 43.0 43.1 URL: http://www.jhasim.com/files/articlefiles/pdf/XASIM_Master_6_5_May_Vignette.pdf. Accessed on: 25 April 2011.
- ↑ Margawani, KR.; Robertson, ID.; Hampson, DJ. (Feb 2009). "Isolation of the anaerobic intestinal spirochaete Brachyspira pilosicoli from long-term residents and Indonesian visitors to Perth, Western Australia.". J Med Microbiol 58 (Pt 2): 248-52. doi:10.1099/jmm.0.004770-0. PMID 19141744. http://ukpmc.ac.uk/abstract/MED/19141744/abstract/MED/19141744?ukpmc_extredirect=http://dx.doi.org/10.1099/jmm.0.004770-0.
- ↑ URL: http://www.cdc.gov/ncidod/eid/vol12no05/05-1180.htm. Accessed on: 28 June 2011.
- ↑ Calderaro A, Bommezzadri S, Gorrini C, et al. (November 2007). "Infective colitis associated with human intestinal spirochetosis". J. Gastroenterol. Hepatol. 22 (11): 1772–9. doi:10.1111/j.1440-1746.2006.04606.x. PMID 17914949.
- ↑ URL: http://www.health.state.ny.us/diseases/communicable/amebiasis/fact_sheet.htm. Accessed on: 17 June 2010.
- ↑ Fernandes, H.; D'Souza, CR.; Swethadri, GK.; Naik, CN.. "Ameboma of the colon with amebic liver abscess mimicking metastatic colon cancer.". Indian J Pathol Microbiol 52 (2): 228-30. PMID 19332922. http://www.ijpmonline.org/article.asp?issn=0377-4929;year=2009;volume=52;issue=2;spage=228;epage=230;aulast=Fernandes.
- ↑ Mortimer, L.; Chadee, K. (Mar 2010). "The immunopathogenesis of Entamoeba histolytica.". Exp Parasitol. doi:10.1016/j.exppara.2010.03.005. PMID 20303955.
- ↑ Abid, S.; Khawaja, A.; Bhimani, SA.; Ahmad, Z.; Hamid, S.; Jafri, W. (2012). "The clinical, endoscopic and histological spectrum of the solitary rectal ulcer syndrome: a single-center experience of 116 cases.". BMC Gastroenterol 12: 72. doi:10.1186/1471-230X-12-72. PMID 22697798.
- ↑ 51.0 51.1 51.2 Crespo Pérez L, Moreira Vicente V, Redondo Verge C, López San Román A, Milicua Salamero JM (November 2007). "["The three-lies disease": solitary rectal ulcer syndrome"] (in Spanish; Castilian). Rev Esp Enferm Dig 99 (11): 663–6. PMID 18271667. http://www.grupoaran.com/mrmUpdate/lecturaPDFfromXML.asp?IdArt=459864&TO=RVN&Eng=1.
- ↑ 52.0 52.1 52.2 Chong VH, Jalihal A (December 2006). "Solitary rectal ulcer syndrome: characteristics, outcomes and predictive profiles for persistent bleeding per rectum". Singapore Med J 47 (12): 1063–8. PMID 17139403. http://www.sma.org.sg/smj/4712/4712a7.pdf.
- ↑ Malik, AK.; Bhaskar, KV.; Kochhar, R.; Bhasin, DK.; Singh, K.; Mehta, SK.; Datta, BN. (Jul 1990). "Solitary ulcer syndrome of the rectum--a histopathologic characterisation of 33 biopsies.". Indian J Pathol Microbiol 33 (3): 216-20. PMID 2091997.
- ↑ Brosens LA, Montgomery EA, Bhagavan BS, Offerhaus GJ, Giardiello FM (November 2009). "Mucosal prolapse syndrome presenting as rectal polyposis". J. Clin. Pathol. 62 (11): 1034–6. doi:10.1136/jcp.2009.067801. PMC 2853932. PMID 19861563. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2853932/.
- ↑ Schneider A, Fritze C, Bosseckert H, Machnik G (1988). "[Primary clinical, endoscopic and histologic findings in solitary rectal ulcer]" (in German). Dtsch Z Verdau Stoffwechselkr 48 (3-4): 183–9. PMID 3234303.
- ↑ URL: http://www.medicinenet.com/melanosis_coli/article.htm. Accessed on: 4 March 2011.
- ↑ 57.0 57.1 57.2 Freeman HJ (July 2008). ""Melanosis" in the small and large intestine". World J. Gastroenterol. 14 (27): 4296-9. PMID 18666316. http://www.wjgnet.com/1007-9327/14/4296.asp.
- ↑ Zapatier, JA.; Schneider, A.; Parra, JL. (Dec 2010). "Overestimation of ulcerative colitis due to melanosis coli.". Acta Gastroenterol Latinoam 40 (4): 351-3. PMID 21375218.
- ↑ 59.0 59.1 Pardi, DS.; Tremaine, WJ.; Rothenberg, HJ.; Batts, KP. (Apr 1998). "Melanosis coli in inflammatory bowel disease.". J Clin Gastroenterol 26 (3): 167-70. PMID 9600362.
- ↑ Kovi J, Leifer C (July 1970). "Lipofuscin pigment accumulation in spontaneous mammary carcinoma of A/Jax mouse". J Natl Med Assoc 62 (4): 287–90. PMC 2611776. PMID 5463681. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2611776/pdf/jnma00512-0077.pdf.
- ↑ URL: http://education.vetmed.vt.edu/curriculum/VM8054/labs/Lab2/Examples/exkluvbarr.htm. Accessed on: 5 May 2010.
- ↑ URL: http://education.vetmed.vt.edu/curriculum/VM8054/labs/Lab2/Examples/exprussb.htm. Accessed on: 5 May 2010.
- ↑ URL: http://education.vetmed.vt.edu/curriculum/VM8054/labs/Lab2/Examples/exfontana.htm. Accessed on: 5 May 2010.
- ↑ Benavides SH, Morgante PE, Monserrat AJ, Zárate J, Porta EA (August 1997). "The pigment of melanosis coli: a lectin histochemical study". Gastrointest. Endosc. 46 (2): 131–8. PMID 9283862.
- ↑ Hui YT, Lam WM, Fong NM, Yuen PK, Lam JT (August 2009). "Heyde's syndrome: diagnosis and management by the novel single-balloon enteroscopy". Hong Kong Med J 15 (4): 301–3. PMID 19652242. http://www.hkmj.org/abstracts/v15n4/301.htm.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 854. ISBN 0-7216-0187-1.
- ↑ 67.0 67.1 Hemingway, AP. (Apr 1988). "Angiodysplasia: current concepts.". Postgrad Med J 64 (750): 259-63. PMID 3054852.
- ↑ Abraham SC, Bhagavan BS, Lee LA, Rashid A, Wu TT (May 2001). "Upper gastrointestinal tract injury in patients receiving kayexalate (sodium polystyrene sulfonate) in sorbitol: clinical, endoscopic, and histopathologic findings". Am. J. Surg. Pathol. 25 (5): 637-44. PMID 11342776. http://meta.wkhealth.com/pt/pt-core/template-journal/lwwgateway/media/landingpage.htm?issn=0147-5185&volume=25&issue=5&spage=637.
- ↑ 69.0 69.1 69.2 Knowles, CH.; Farrugia, G. (Feb 2011). "Gastrointestinal neuromuscular pathology in chronic constipation.". Best Pract Res Clin Gastroenterol 25 (1): 43-57. doi:10.1016/j.bpg.2010.12.001. PMID 21382578.
- ↑ Streutker, CJ.; Huizinga, JD.; Driman, DK.; Riddell, RH. (Jan 2007). "Interstitial cells of Cajal in health and disease. Part I: normal ICC structure and function with associated motility disorders.". Histopathology 50 (2): 176-89. doi:10.1111/j.1365-2559.2006.02493.x. PMID 17222246. http://onlinelibrary.wiley.com/doi/10.1111/j.1365-2559.2006.02493.x/pdf.
- ↑ IAV. 15 December 2009.
- ↑ 72.0 72.1 72.2 Knowles, CH.; De Giorgio, R.; Kapur, RP.; Bruder, E.; Farrugia, G.; Geboes, K.; Gershon, MD.; Hutson, J. et al. (Aug 2009). "Gastrointestinal neuromuscular pathology: guidelines for histological techniques and reporting on behalf of the Gastro 2009 International Working Group.". Acta Neuropathol 118 (2): 271-301. doi:10.1007/s00401-009-0527-y. PMID 19360428.
- ↑ Barami K, Iversen K, Furneaux H, Goldman SA (September 1995). "Hu protein as an early marker of neuronal phenotypic differentiation by subependymal zone cells of the adult songbird forebrain". J. Neurobiol. 28 (1): 82–101. doi:10.1002/neu.480280108. PMID 8586967.