Placenta
The placenta feeds the developing baby, breathes for it and disposes of its waste.
Clinical
Examination of the placenta
- Most placentas are not examined by a pathologist.
Indications for exam by pathology
Some indications for exam by a pathologist:
- Abnormalities in the:
- Fetus:
- Bad fetal outcome.
- Suspected or known congenital abnormalities or chromosomal abnormalities.
- IUGR.
- Mother:
- Infection/suspected infection.
- Pre-term labour.
- Maternal disease (e.g. SLE, coagulopathy).
- Complicated pregnancy (preclampsia, pregnancy induced hypertension, gestational diabetes).
- Placenta:
- Unusual gross characteristics.[1]
- Fetus:
A more detailed list is given by Hargitai et al.[2] and Chang.[3]
Most common
Most common reasons for submitting a placenta to pathology:[4]
- Prematurity.
- PROM / possible chorioamnionitis.
- Multiple gestation.
Bleeding in late pregnancy
DDx of bleeding in late pregnancy:
- Placental abruption (most common).
- Placenta previa.
- Vasa previa (fetus losing blood).
Clinical screening tests
- PAPP-A - low values seen in aneuploidy.[5]
Abbreviations
- C/S = Caesarian section.
- LSCS = lower segment C-section.
- FTP = failure to progress.
- PROM = premature rupture of membranes.
- PPROM = preterm premature ruptures of membranes.
- IUGR = intrauterine growth restriction.
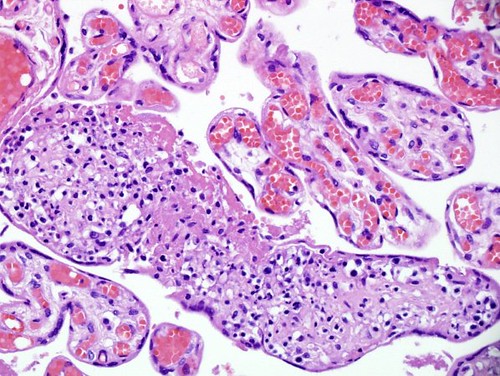
Normal histology
Villi
This is dealt with in a separate article that also covers the types of trophoblast (cytotrophoblast, syncytiotrophoblast, intermediate trophoblast).
Cord
Omphalomesenteric duct remnant
- AKA vitelline duct.
- Benign embryologic remnant.
Features:
- Duct with benign looking cuboidal epithelium.
Allantoic duct remnant
- Benign embryologic remnant.
Features:
- Duct with benign looking flat epithelium.
Vitelline artery remnant
Features:
- Small artery in the cord.
Membranes
Fetus to mother:
- Amnion - thin layer: one cell layer, basement membrane, connective tissue.
- Cleft - artifactual - empty space.
- Chorion - vascular.
- Decidua (maternal tissue) - may contain obsolete chorionic villi; place to look for hypertensive changes.
Amnion
General:
- Next to fetus, surrounds amniotic fluid, avascular.
Characteristics:
- Characterized by a single layer of cells.[6]
- Cuboidal/squamoid shape.
- Eosinophilic cytoplasm.
- Central nucleus.
- Squamous metaplasia may be seen at cord insertion.
- Basement membrane.
- 'Compact layer'.[6]
- 'Fibroblastic layer'.[6]
Chorion
General:
- Surrounds amnion.
Characteristics:
- Layers:[7]
- 'Reticular layer' - cellular (inner aspect).
- 'Pseudo-basemement membrane'.
- 'Outer trophoblastic layer'.
- Has blood vessels.
- Opposed to "trophoblastic X cells" on side opposite of amnion.[6]
- Beneath of the "trophoblastic X cells" is decidua (mnemonic NEW = nucleus central, eosinophilic, well-defined cell border), which is maternal tissue.
Note:
- Fibrin deposition may be found deep to the chorion - known as subchorionic fibrin deposition.
- Gross: subchorionic, white/yellow, laminated, classically has a triangular-shape with the base of triangle parallel to fetal aspect of disc.
- Arises due to localized stasis of the inter-villous maternal blood.
- Focal small deposits are considered to be a normal finding - seen in ~15% of cases.[8][9]
- The pathologic counterpart of this is perivillous fibrin deposition.
- Gross: subchorionic, white/yellow, laminated, classically has a triangular-shape with the base of triangle parallel to fetal aspect of disc.
Common terms
- Chorionic plate - fetal aspect of placenta.
- Basal plate - maternal aspect of placenta.
- Has extravillous trophoblast.
- Place to look for maternal vessels.
Grossing
This is often very quick. The gross is quite important, as some things cannot be diagnosed microscopically.
General
- Dimensions:
- Disc.
- Length of cord, diameter of cord.
- Accessory lobes - dimensions.
- Two lobes of equal size + cord arises in between = bilobate placenta.
- Mass (weight).
- Should be done 'trimmed' (cord cut-off, membrane cut-off).
- Should be done when placenta is "fresh", i.e. not fixed -- as mass tables are based on fresh state.
- Umbilical cord
- Attachment.
- Location: central, eccentric, marginal.
- Marginal attachment assoc. with hypertension[10]
- Membranous or velamentous (veil-like) insertion.
- Vessels separate/branch prior to reaching placental disc.
- Furcate insertion - blood vessels separate before reaching placenta disc/not surrounded by Wharton's jelly - vessels more exposed to trauma (risk for vasa previa).
- Location: central, eccentric, marginal.
- Knots (false vs. true).
- False knots are nothing to worry about -- look like a knot but aren't really one.
- Twisting/coiling - 1-3 coils/10 cm is normal.
- Number of vessels.
- Normal: 2 arteries, 1 vein.
- Attachment.
- Membranes - shiny & translucent - normal (green, opaque/dull - chorioamnionitis).
- Attachment (insertion): marginal (normal), circummarginate (inside edge), circumvallate (folding on self).
- Site of rupture - if obvious; low point of rupture suggests low-lying placenta.
- Placental disc.
- Fetal surface - normal is shinny.
- Dull in chorioamnionitis.
- Maternal surface
- Are the cotyledons intact?
- Adherent clot?
- Parenchyma - after sectioning:
- White vs. red nodules.
- Fetal surface - normal is shinny.
Notes:
- Parenchymal nodules - a brief DDx:
- White: infarct (chronic), thrombi, chorangioma, perivillous fibrin deposition.
- Red: infarct (acute), thrombi.
Sections
- Cord two sections.
- Membranes (rolled), two rolls or more.[11]
- Cord at insertion + disc.
- Placenta - full thickness (maternal and fetal surface).
- Sections should not be taken at the margin of the disc.
Placental membranes
Appearance:[12]
- Normal - shiny.
- Chorioamnionitis - opaque/dull.
- Meconium - green.
- Amnion nodosum - yellow patches.
- Some describe 'em as white.[13]
Placental mass
It is considered routine to obtain a mass for the placenta. This is usually done when the placenta is fresh and with the membranes and cord trimmed, as most tables of placental mass were created with these parameters.
Placental mass by gestational age:[14]
| Gest. Age/Percentile | 25% | 50% | 75% |
| 32 weeks | 275 g | 318 g | 377 g |
| 36 weeks | 369 g | 440 g | 508 g |
| 40 weeks | 440 g | 501 g | 572 g |
Linear regression - placental mass-gestational age
Based on the table in the AFIP book[15] I generated the following regression lines:
| 50% | 10% | 90% | |
| slope (g/week) | 21.58088235 | 19.70588235 | 25.40196078 |
| y-intercept (g) | -357.4558824 | -397.2352941 | -366.7254902 |
| Pearson (r) | 0.988670724 | 0.988268672 | 0.982206408 |
placental mass = slope x gestational age + intercept
What to remember...
Extrapolated from the linear regression (see above):
- 50% at term = 500 grams.
- 50% at 26 weeks = 200 grams.
- The change in mass/week is approximately linear and equal to 300 grams / 14 weeks ~ 20 grams/week.
- The spread in mass between 10% and 90%, crudely estimated, is 200 grams (for GA=26-40).
Notes:
- Is it required?
- Sebire and Fox have advocated abandoning the practise of obtaining a placental mass, due to the large number of uncontrolled variables inherent in these measures. Instead, they have advocated using mushy descriptors such as "small", "average" and "large", which require experience in examining the organ.[16]
- In the context of quality, a measure (even if somewhat flawed), is almost certainly more reproducible than arbitrary descriptors which require experience and a continuing case volume to calibrate.
- Sebire and Fox have advocated abandoning the practise of obtaining a placental mass, due to the large number of uncontrolled variables inherent in these measures. Instead, they have advocated using mushy descriptors such as "small", "average" and "large", which require experience in examining the organ.[16]
Placentomegaly
Associations:[17]
- Maternal diabetes - esp. poorly controlled.[18]
- Maternal anemia/low maternal iron stores.[19]
- Fetal malformations.
- Neoplasms of the placenta, e.g. chorangioma.
- Twin-twin transfusion syndrome.
- Chronic intrauterine infections, e.g. syphilis, toxoplasmosis, cytomegalovirus.
Lame causes of a heavy placenta:
- Dates wrong - error in determining the estimated date of confinement.
- Adherent blood clot.
Comment:
- Most of causes seem to have one thing in common:
- There is a decreased oxygen delivery to the fetus.
Sign out
PLACENTA, UMBILICAL CORD AND FETAL MEMBRANES, CESAERIAN SECTION: - LARGE PLACENTA (819 GRAMS -- TRIMMED, POST-FIXATION WEIGHT). - FETAL MEMBRANES WITHIN NORMAL LIMITS. - THREE VESSEL UMBILICAL CORD WITHIN NORMAL LIMITS. - PLACENTAL DISC WITH THIRD TRIMESTER VILLI.
Placental growth restriction
- AKA placenta small for gestational age.
Associations:
- Maternal vascular disease, e.g. hypertension.
- Fetal malformations.
Sign out
PLACENTA, UMBILICAL CORD AND FETAL MEMBRANES, CESAERIAN SECTION: - PLACENTA SMALL FOR GESTATIONAL AGE (160 GRAMS -- TRIMMED, POST-FIXATION WEIGHT). - THREE VESSEL UMBILICAL CORD WITHIN NORMAL LIMITS. - FETAL MEMBRANES WITHIN NORMAL LIMITS. - PLACENTAL DISC WITH THIRD TRIMESTER VILLI WITH: -- OLD CENTRAL TRANSMURAL INFARCT (1.7 CM MAXIMAL DIMENSION). COMMENT: The 10th percentile placental mass (pre-fixation) for 34 weeks and 2 days is approximately 390 grams.
Overview of placental pathology
Approach
The pathology of the placenta is diverse and is not easy to group.
It terms of remembering things. It is probably easiest to take a combined anatomical, etiologic and morphologic approach.
Anatomical basis:
- Cord.
- Membranes.
- Disc.
Etiologic:
- Congential.
- Infectious.
- Neoplastic.
- Endocrine.
- Trauma.
- Vascular.
- Degenerative.
- Autoimmune.
- Toxic.
- Idiopathic.
Compartmental:
- Vasculature.
- Membranes.
- Parenchyma:
- Maternal part (decidua).
- Fetal part (villi, cord).
Common entities/diagnoses
- Normal.
- Chorioamnionitis.
- Placental abruption.
- Meconium.
- Hypertensive changes.
Sign out
What should be commented on...
- Placenta:
- Maturity of villi (2nd or 3rd trimester).
- Infarction?
- Subchorionic less important than maternal aspect.
- Peripheral aspect of placental disc less important than central region of disc.
- Blood vessels.
- Maternal.
- Fetal.
- Membranes.
- Cord:
- 3 vessel?
- Vasculitis/inflammation?
Mnemonic: chorio, cord, vessels, villi (maturity, infarction).
Normal placenta
PLACENTA, UMBILICAL CORD AND FETAL MEMBRANES, BIRTH: - THREE VESSEL UMBILICAL CORD WITHIN NORMAL LIMITS. - FETAL MEMBRANES WITHIN NORMAL LIMITS. - PLACENTAL DISC WITH THIRD TRIMESTER VILLI WITHIN NORMAL LIMITS.
C-section
PLACENTA, UMBILICAL CORD AND FETAL MEMBRANES, CAESARIAN SECTION: - THREE VESSEL UMBILICAL CORD WITHIN NORMAL LIMITS. - FETAL MEMBRANES WITHIN NORMAL LIMITS. - PLACENTAL DISC WITH THIRD TRIMESTER VILLI WITHIN NORMAL LIMITS.
Cord pathology
- Two vessel cord.
- Hypercoiling/Hypocoiling.
- Abnormal insertion.
- Cord knots (true vs. false).
- Strictures.
- Hematoma.
- Hemangioma.
- Benign cyst.
Two vessel umbilical cord
Associations
- Associated with congenital abnormalities, esp. cardiac - key point.[20]
- Thought to be an acquired defect (as prevalence is lower early in gestation).
- May be seen in association of other cord abnormalities (e.g. marginal insertion, velamentous insertion).
- In apparently well (liveborn) infants it is associated with (occult) renal abnormalities, specifically vesico-ureteric reflux; there is no evidence for other abnormalities.[21]
- Associated with maternal diabetes.[22]
Image:
{kind=link}
Sign out
PLACENTA, UMBILICAL CORD AND FETAL MEMBRANES, CAESARIAN SECTION: - TWO VESSEL UMBILICAL CORD, NEGATIVE FOR INFLAMMATION. - FETAL MEMBRANES WITH FOCAL PIGMENTED CELLS CONSISTENT WITH MECONIUM, NEGATIVE FOR APPARENT CHORIOAMNIONITIS. - PLACENTAL DISC WITH THIRD TRIMESTER VILLI WITHOUT APPARENT PATHOLOGY.
Insertion
Marginal insertion
Definition:
- The umbilical cord is attached to the placental disc at its margin.
Prevalence:
- Approximately 12% of placentas.[20]
Relevance:
- None according to WMSP.[20]
- In theory, the cord, dependent on its relation to the internal os, is at greater risk of injury (leading to vasa previa) and compression (fetal hypoxia). A retrospective study found cord position in relation to the internal os is predictive for vasa previa.[24]
Velamentous insertion
Definition:
- The umbilical cord inserts into the fetal membranes.[20]
- The vessels are not protected by Wharton's jelly.
- Wharton's jelly = the connective tissue surrounding the vessels in the cord.
- The vessels are not protected by Wharton's jelly.
Details:[20]
- 3/4 of the time the vessel also branch; in the remaining 1/4 the vessels stay together.
Relevance:
- Increased risk of vasa previa.[24]
Sign out
PLACENTA, UMBILICAL CORDS AND FETAL MEMBRANES, BIRTH: - THREE VESSEL UMBILICAL CORD WITH A VELAMENTOUS INSERTION, OTHERWISE WITHIN NORMAL LIMITS. - FETAL MEMBRANES WITHIN NORMAL LIMITS. - PLACENTAL DISC WITH THIRD TRIMESTER VILLI WITHIN NORMAL LIMITS.
Umbilical knot
General
- Prevalence ~1.25%.[25][26]
- Increase risk of stillbirth; odds ratio 3.93.[25]
Gross
Work-up:[26]
- Diameter measures and colour on both sides of the knot.
- Knot should be untied to assess for deformation of Wharton's jelly.
- Sections from both sides of the knot - to look for thrombi.
Note:
- False knots (large diameter - focally) are common - they cannot be untied.
Microscopic
Features:
- +/-Thrombi.
- Fibrin deposition.
- +/-Lines of Zahn.
Images:
Coiling
- Hypo- and hypercoiling are both considered problematic.[20]
- Normal: 1-3 coils/10 cm.[27]
- Associated with cord stricture, which is usu. at the fetal end of the cord.[28]
Notes:
- There is little uniformity in how coiling is assessed in the medical literature - though 10% and 90% are considered the cut-points for normal.[29]
- What are the 10% and 90% cut-points? They are not given in WMSP. UT access to a journal article[30] that might have it is screwed-up.
Cord hematoma
Features:[28]
- Rare ~ 1/5500.
- Mortality ~50% is severe.
Image: Hematoma (flylib.com).[31]
{kind=link}
Membranes
- Squamous metaplasia.
- Chorioamnionitis - see infection section.
Amnion nodosum
General
- Associated with (long-standing) oligohydramnios.[32]
- Should be separated from squamous metaplasia of amnion.
Gross
Features:[33]
- Yellow nodules ~ 1-5 mm.
- Some think they are white.[34]
DDx:
- Squamous metaplasia of the amnion - large irregular patches, usu. white.
Images:
- Amnion nodosum (webpathology.com).
- Amnion nodosum & squamous metaplasia of the amnion (archivesofpathology.org).[33]
Microscopic
Features:[33]
- Stratified squamous epithelium - non-keratinizing or minimal keratin.
- Amorphous acidophilic (pink) debris.
Note:
- Normal amnion = simple epithelium.
Images:
- Amnion nodosum (webpathology.com).
- Amnion nodosum & squamous metaplasia of the amnion (archivesofpathology.org).[33]
Placental meconium
- AKA meconium staining.
General
- Associated with fetal distress.
- Small amount - at term - is considered to be normal.
Other meconium-related pathology:
Gross
- Green/green discolourization.
Microscopic
Features:[35]
- Meconium histiocytes - key feature.
- Macrophages with brown fine granular pigment.
- Pseudostratified epithelium (amnion) - low power.
- Amnion - columnar morphology (normally cuboidal).
- "Drop-out" of individual amnion cells / loss of individual cells.
Time of meconium passage:[36]
- <1 h - no staining of membranes.
- 1-3 h - amnion is stained.
- >3 h - chorion is stained.
DDx:
- Hemosiderin-laden macrophages.
- This is sorted-out with an iron stain -- see below.
Notes:
- The above time course is disputed - in vitro experiments suggest it is considerably longer.[37]
Images:
{kind=link}
{kind=link}
Special stains
- Hemosiderin +ve in hemosiderin-laden macrophages.
- PAS +ve in meconium-laden macrophages.[38]
Useful to differentiate hemosiderin-laden macrophages and meconium laden macrophages:
- Hemosiderin stain -- +ve for old blood.
- Prussian-blue stain = hemosiderin stain.[39]
Notes:
- PAS-D -- +ve in meconium... though may rarely stain hemosiderin.
- Meconium contains bile.[40]
Sign out
PLACENTA, UMBILICAL CORD AND FETAL MEMBRANES, BIRTH: - FETAL MEMBRANES WITH MECONIUM-LADEN MACROPHAGES, NEGATIVE FOR CHORIOAMNIONITIS. - THREE VESSEL UMBILICAL CORD WITHIN NORMAL LIMITS. - PLACENTAL DISC WITH THIRD TRIMESTER VILLI WITHIN NORMAL LIMITS.
COMMENT: A PAS-D stain and Prussian blue stain were used to confirm the presence of meconium.
Not definite
PLACENTA, UMBILICAL CORD AND FETAL MEMBRANES, CESAERIAN SECTION: - EARLY CHORIOAMNIONITIS. - FETAL MEMBRANES WITH FOCAL AMNION CELL DROP-OUT AND RARE PIGMENTED CELLS SUGGESTIVE OF MECONIUM. - THREE VESSEL UMBILICAL CORD WITHIN NORMAL LIMITS. - PLACENTAL DISC WITH THIRD TRIMESTER VILLI.
Squamous metaplasia of the amnion
General
- Benign common finding thought to be of no clinical significance.[41]
- One case report suggesting an association with chorioamnionitis.[42]
- Needs to be separated from amnion nodosum - important.[43]
Gross
Features:[33]
- White (or yellow) plaques - irregular outline.
DDx:
- Amnion nodosum - small (~1-5 mm), round, classically yellow.
Images:
Microscopic
Features:[33]
- Dense, paucicellular (pink) compact keratin - key feature.
Image:
{kind=link}
Circumvallate placenta
- AKA circumvallate insertion of the membranes.
General
- May be associated with placental abruption.[45]
Note:
- Membranes usually attach to the edge of the placenta.
Gross
- Fetal membranes attach to the fetal surface of the placenta away from the margin of the placental disc.
Classification:
- Partial - not circumferential.
- Complete.
DDx:
Images:
{kind=link}
{kind=link}
Twin placentas
These are often submitted... even if they are normal. In these specimens, usually, the chorion is the key.
It covers:
- Monozygotic vs. dizygotic twins.
- Twin-to-twin transfusion syndrome.
Placental disc
Villous edema
General
- Non-specific finding.
Microscopic
Features:
- "Swiss chesse-like" appearance / bubbly appearance.
- Usu. patchy and focal.
DDx:
- Chorioamnionitis.
- Fetal edema.
- Idiopathic (no cause apparent).
Image:
{kind=link}
Placental villous immaturity
- AKA distal villous immaturity, AKA villous immaturity, AKA villous dysmaturity.[47]
- Abbreviated PVI.
General
Associated with:
- Diabetes mellitus.[48]
- Beckwith-Wiedemann syndrome.
- Intrauterine fetal demise near term.[49]
Microscopic
Features:[47]
- Increased numbers of (immature) intermediate villi (in relation to the gestational age) with:
- Increased number of capillaries.
- Edema.
- Macrophages.
- Large diffusion distance (vessel-to-villous surface distance large).
- Less (mature) terminal villi.[50]
DDx:
Images:
{kind=link}
{kind=link}
Diseases of the placental attachment
Placenta creta
- What?
- Trophoblastic tissue deeper than it should be.
- Clinical?
- Postpartum hemorrhage leading to a hysterectomy.[51]
- Pathogenesis?
Note:
- Normal: trophoblastic tissue attaches to the decidua.[53]
Placenta accreta
- Trophoblastic tissue (directly) adherent to the myometrium.[53]
Image:
{kind=link}
Placenta increta
- Trophoblastic tissue extends into the myometrium.
Placenta percreta
- Trophoblastic tissue penetrates through the myometrium.
Placental abruption
General
Classic clinical manifestations:[55]
- Vaginal bleeding (~70%).
- Abdominal pain (~50%).
- Fetal heart rate abnormalities (~70%).
Sign-out:
- Pathologists should sign-out this as "focal adherent retroplacental hematoma".
- The pathologic findings may be due to abruption or manual removal of the placenta.
Gross
Features:[56]
- Large adherent blood clot.
- Disc depression on maternal side.
Notes:
- Loosely attached clot less convincing.
- Central haemorrhage is the most worrisome.
Microscopic
Features:
- Decidual hemorrhage.
- Blood in the decidua.
- Intravillous hemorrhage, AKA villous stromal hemorrhage.
- "Bags of blood" - blood outside of vessels in the villi.
- Should not be confused with congested villi.
- "Bags of blood" - blood outside of vessels in the villi.
Notes:
- There are no definitive microscopic findings for placental abruption.
- Intravillous hemorrhage is non-specific - may arise in the following: early placental infarct, cord compression, abdominal trauma.
Inflammatory pathologies
Overview of infections
General:[57]
- Infection usually ascending, i.e. from vagina up through cervix.
- Associated with intercourse.
- Hematogenous rare - manifest as villitis.
- Think TORCH infections (toxoplasmosis, others (syphilis, TB, listeriosis), rubella, cytomegalovirus, herpes simplex virus).
- Funisitis usually follows chorioamnionitis.
- Inflammatory cells in umbilical cord are fetal (trivia).
Types
By site:[57]
- Fetal membranes: chorioamnionitis, membranitis.[58]
- Umbilical cord: funisitis.
- Placenta: placentitis, villitis.
Membranitis
General
- Controversial. (???)
Microscopic
Features:
- PMNs in the decidua.
- +/-PMNs in subamniotic tissue.
- +/-Necrosis in decidua or chorion/subamniotic tissue.
Note:
- Plasma cells in the decidua = chronic deciduitis.
Grading membranitis
Sternberg:[58]
- PMNs - decidua only.
- PMNs - in subamniotic tissue.
- 1 or 2 + necrosis in decidua or chorion/subamniotic tissue.
Chorioamnionitis
General
- Associated with pre-term labour.[59]
- Classically described as due to an ascending infection.
- At term usually non-infectious.[60]
Clinical features:
- Maternal fever.
- Premature rupture of membranes (PROM).
- Non-reassuring fetal heart rate (NRFHR).
Management:
- Antibiotics - usually ampicillin and gentamicin.[61]
Gross
- Fetal membranes dull/opaque.
Microscopic
Features:
- Neutrophils in the amnion.
- Amnion:
- The simple cuboidal epithelium and the paucicellular underlying connective tissue
- Separated from the chorion by an artefactual cleft.
- Amnion:
Note:
- Severe cases may have umbilical cord vasculitis or funisitis.
Images:
- WC:
{kind=link}
{kind=link}
{kind=link}
Grading chorioamnionitis
Chorioamnionitis:[58]
- placental chorionic plate only.
- 1 + subamniotic tissue.
- 1 or 2 + necrosis or abscess.
Sign out
PLACENTA, UMBILICAL CORD AND FETAL MEMBRANES, CESAERIAN SECTION: - CHORIOAMNIONITIS. - FETAL MEMBRANES NEGATIVE MECONIUM. - THREE VESSEL UMBILICAL CORD WITHIN NORMAL LIMITS. - PLACENTAL DISC WITH THIRD TRIMESTER VILLI. - THROMBUS OF THE PLACENTAL DISC (1.3 CM - MAXIMAL DIMENSION).
Umbilical cord vasculitis
General
- Usually seen together with chorioamnionitis.
- May be described as the fetal response to chorioamnionitis.[62]
- Presence considered to be a good prognosticator.[62]
Microscopic
Features:
- Neutrophils in the vessels of the umbilical cord.
- Wharton's jelly without neutrophils.
Note:
- Umbilical vein involvement (umbilical phlebitis) precedes umbilical artery involvement (umbilical arteritis).[63]
DDx:
- Funisitis - neutrophils also in the connective tissue of the umbilical cord (Wharton's jelly).
Grading
Umbilical cord vasculitis:[58]
- +0.5 for each vessel.
- +0.5 for each vessel with severe involvement.
Funisitis
General
- Usu. seen together with chorioamnionitis.
Microscopic
Features:
- Neutrophils in the vessels of the umbilical cord and Wharton's jelly.
Note:
- Wharton's jelly = connective tissue of the umbilical cord.
DDx:
- Umbilical cord vasculitis - neutrophils only in the vessel wall.
Grading funisitis
Funisitis:[58]
- Focal inflammation.
- Diffuse inflammation.
- Necrosis - in umbilical vessels or Wharton jelly.
Sign out
PLACENTA, UMBILICAL CORD AND FETAL MEMBRANES, BIRTH: - CHORIOAMNIONITIS. - THREE VESSEL UMBILICAL CORD WITH FUNISITIS. - PLACENTAL DISC WITH THIRD TRIMESTER VILLI. - TWO THROMBI OF THE PLACENTAL DISC (LARGEST 0.9 CM - MAXIMAL DIMENSION).
Acute villitis
General
- Rare.
- Typically viral - see TORCH infections.
Microscopic
Features:
- Neutrophils in the villous stroma - key feature.
Images:
Villitis of unknown etiology
- Abbreviated VUE.
General
Features:[64]
- Usually term placenta.
- Prevalence: 5% to 15% of all placentas.
- Associated with:
- Intrauterine growth restriction (IUGR).
- Recurrent reproductive loss/adverse outcomes in subsequent pregnancies -- key point.
- Recurrence in up 37% of cases.[65]
Etiology:
- Unknown - as the name of the entity suggests.
- Suspected to be immune-mediated.
Microscopic
Features:[64]
- Lymphocytes in villous stroma - key feature.
- Usually focal/patchy.
- Lymphocytes: maternal derivation, T-lymphocytes -- mostly CD8-positive.
- +/-Intervillositis (lymphocytes between villi).
- +/-Histiocytes.
Notes:
- Lymphocytes are smaller and stain darker than the cells of the villi. (???)
- Neutrophils are usually absent. A significant number of 'em is suggestive of an infectious villitis.
- Infective villitis is usu. B-cell predominant.
- No plasma cells - this suggests an infectious etiology.[66]
- Plasma cells may be seen in the decidua -- these can be ignored.
Images:
- WC:
- www:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Chronic intervillitis
General
- Rare.
- Massive chronic intervillitis - associated IUGR, spontaneous abortion, perinatal fetal death.[70]
- Recurs.
Microscopic
- Intervillous inflammatory cells:
- Lymphocytes.
- Histiocytes.
- Fibrinoid deposition.
Images:
{kind=link}
{kind=link}
Chronic deciduitis
- AKA plasma cell deciduitis.
General
- Associated with preterm labour.[71]
Microscopic
Features:[71]
- Plasma cells within the decidua.
Notes:
- Decidua = maternal tissue.
Images:
{kind=link}
{kind=link}
Placental infarction
True infarcts
General
- May be seen in conjunction with a retroplacental hematoma.
- Infarcts frequently associated with hypertension.[72][73]
Note: "Maternal floor infarct" is not a true infarct.[74]
Gross
Features:[28]
- Early - red.
- Late - white/grey.
Significant infarcts
- > 3cm --or-- central location --or-- in 1st or 2nd trimester.[citation needed]
- Small foci are accepted in term placentae - typically at periphery.
Images:
Microscopic
Features:
- Necrosis of villi; hyaline material (acellular eosinophilic material) replaces the stroma of the villi.
- Loss of intervillous space.[28]
- Villi appear to be crowded.[75]
- Normal spacing is ~1x smallest villus or larger.
- In perivillous fibrin deposition - spacing usu. larger than normal.
- Normal spacing is ~1x smallest villus or larger.
- Villi appear to be crowded.[75]
- Prominent syncytial knots.
- Thickened trophoblastic basement membrane (below cytotrophoblasts).
- +/-Changes seen in decidual vasculopathy:
- Acute atherosis (vaguely like atherosclerosis).
- Fibrinoid necrosis.
- Vessel wall lipid deposition.
- Acute atherosis (vaguely like atherosclerosis).
Images:
- WC:
- www:
{kind=link}
{kind=link}
{kind=link}
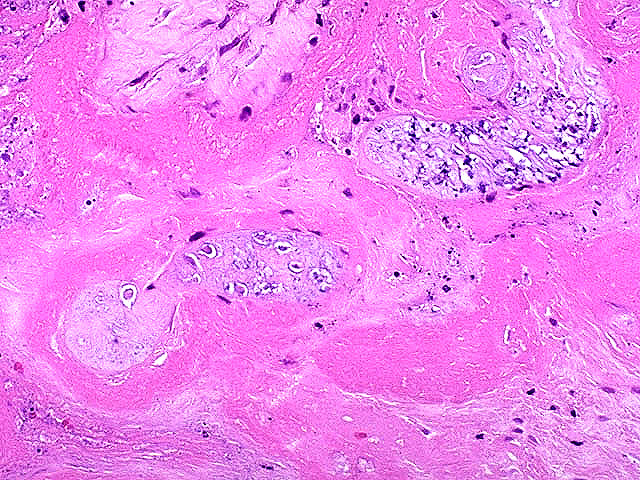
Perivillous fibrin deposition
- Abbreviation PFD.
General
- Thought to be an immunologic problem - resulting in platelet activation and fibrin deposition.[77]
- May be associated with diabetes mellitus.[78]
Gross
- Pale (white).
- Firm.
- White fibrous sepatae.
Microscopic
Features:
- Acellular eosinophilic material around formed villi.
- Obliteration of intervillous space.
- Intervillous distance increased vis-a-vis normal - key feature.
Notes:
- Nuclei of villi are usually preserved.
- Villi may have secondary infarction, i.e. there may be nuclear destruction (karyolysis, karyorrhexis, pyknosis).
DDx:
- Placental infarction - loss of nuclei in the villi (below the edge of the lesion).
- Massive perivillous fibrin deposition (maternal floor infarct).
Images:
Sign out
Thrombi
PLACENTA, UMBILICAL CORD AND FETAL MEMBRANES, BIRTH: - THREE VESSEL UMBILICAL CORD WITHIN NORMAL LIMITS. - FETAL MEMBRANES WITHIN NORMAL LIMITS. - PLACENTAL DISC WITH THIRD TRIMESTER VILLI AND THREE LARGE INTERVILLOUS THROMBI (BLOCKS A7-A9).
Maternal floor infarction
- Abbreviated MFI.
- Formally placental maternal floor infarction.
- AKA massive perivillous fibrin deposition.[79]
General
- Not a true infact.
- It is really fibrin deposition.[74]
Associations:
- Intrauterine growth restriction (IUGR).[80][81]
- Anti-phospholipid antibody (APLA) syndrome.[77]
- APLA is associated with recurrent miscarriage - can be treated with heparin + ASA.[77]
- Pregnancy-induced hypertension.[82]
Gross
Features:[83]
- +/-Thickened placenta.
- Maternal aspect of placental disc irregular or lobulated appearance.
- +/-Yellowish discolourization.
Microscopic
Features:
- Extensive fibrin deposition around villi on maternal aspect - see: Perivillous fibrin deposition.
DDx:
- Perivillous fibrin deposition - less perivillous fibrin.
- Placental infarction.
Images:
- Maternal floor infarct (flickr.com).
- Maternal floor infarct (flickr.com).
- Maternal floor infarct - several images (upmc.edu).
Sign out
PLACENTA, UMBILICAL CORD AND FETAL MEMBRANES, BIRTH: - THREE VESSEL UMBILICAL CORD WITHIN NORMAL LIMITS. - FETAL MEMBRANES WITHIN NORMAL LIMITS. - SMALL PLACENTAL DISC WITH MASSIVE PERIVILLOUS FIBRIN DEPOSITION, SEE COMMENT. COMMENT: Massive perivillous fibrin deposition (MPVFD) is associated with intrauterine growth restriction (IUGR). MPVFD is described in association with in anti-phospholipid antibody (APLA) syndrome, pregnancy-induced hypertension and congenital infections. Perivillous fibrin deposition may be seen in diabetes. There is no apparent infection. Changes suggestive of decidual vasculopathy are not apparent. Changes suggestive of fetal thrombotic vasculopathy are not identified.
Fetal disease
Fetal thrombotic vasculopathy
- Abbreviated FTV.
- A large number of terms are used for this including:[85]
- Fibrinous vasculosis.
- Fibromuscular sclerosis.
- Fetal artery stem thrombosis.
- The multitude of terms reflects the confusion about this finding and that it has numerous etiologies.[85]
General
Microscopic
Features:[86]
- Thrombus in the fetal vasculature +/- recanalization.
- Eosinophilic (light pink on H&E), moderately granular intravascular material (fibrin) with layering.
- Clustered fibrotic villi without blood vessels - key feature.
- This is a chronic change.
Images:
- www:
- WC:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Hemorrhagic endovasculitis
- Abbreviated HEV.
General
- Associated with stillbirth.[90]
Microscopic
Features:[91]
- Walls of the (fetal) placental blood vessels (in the villi) are disrupted.
- +/-Intraluminal necrotic debris.
- RBC fragmentation.
Maternal disease
Hypertensive changes
General
Associated pathologic changes:[92]
- Placental infarcts.
- Increased syncytial knots.
- Hypovascularity of the villi.
- Cytotrophoblastic proliferation.
- Thickening of the trophoblastic basement membrane.
Microscopic
Features:[92]
- Enlarged endothelial cells - fetal capillaries.
- Atherosis of the spiral arteries - placental bed (maternal).
Notes:
- One should look for the changes in the membrane roll, not the maternal surface.[93]
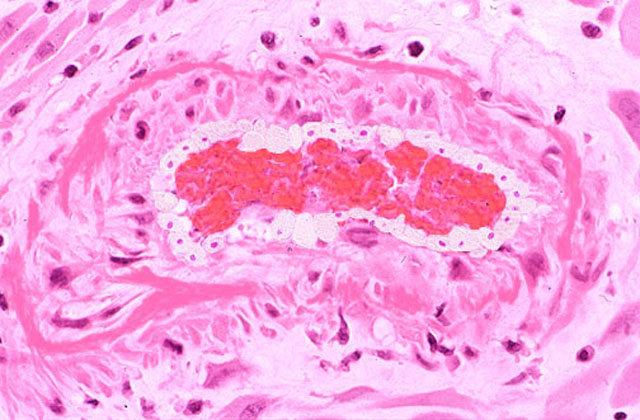
Hypertrophic decidual vasculopathy
General
- A change seen in hypertension.
- Seen in intrauterine growth restriction (IUGR).
Microscopic
Features:[80]
- Mild or moderate:
- Perivascular inflammatory cells.
- +/-Vascular thrombosis.
- Smooth muscle hypertrophy.
- Endothelial hyperplasia.
- Above two lead to narrowing of the decidual spiral arteries[94] -- key feature.
- Severe:[80]
- Atherosis of maternal blood vessels.
- Foamy macrophages within vascular wall.
- Fibrinoid necrosis of vessel wall (amorphous eosinophilic material vessel wall).
- Atherosis of maternal blood vessels.
Note:
- Smooth muscle hypertrophy can also be understood as lack of physiological conversion of spiral arteries of the uterus.[95]
Images:
{kind=link}
{kind=link}
{kind=link}
HELLP syndrome
General
- Diagnosed clinically.
- Pathologically not the same as severe preclampsia.[97]
Definition:
- H = hemolysis.
- EL = elevated liver enzymes.
- LP = low platelets.
Microscopic
Features:[98]
- Thrombotic microangiopathic vasculopathy.
- In essence: severe hypertrophic decidual vasculopathy. (???)
Malaria
General
- Uncommon in Canada.
- May lead to fetal demise.
Microscopic
Feature:
- RBCs with basophilic dots ~1-2 micrometres.
Image:
{kind=link}
Tumours
Chorangioma
General
- Hamartoma-like growth in the placenta consisting of blood vessels.[99]
Epidemiology:
- Often benign/insignificant; large lesions (>4 cm[99] or >5 cm[100]) or multiple lesions are significant.
- May be association with:
- Fetal maternal haemorrhage.
- Fetal hydrops.
- IUGR.
- Incidence: ~1 in 100 placentas.[99]
Gross
- White lesions.
- Occasionally red lesions.
Microscopic
Features:[99]
- Mass of capillaries - key feature.
- +/-High cellularity.
- +/-Degenerative changes.
Images:
{kind=link}
{kind=link}
Notes:
- Must be differentiated from chorangiomatosis (associated with preeclampsia & IUGR) and chorangiosis (assoc. with maternal diabetes mellitus).[99]
Chorangiomatosis
General
Associated with:
- Preeclampsia.
- IUGR.
Gross
- Multiple tan nodules.
Microscopic
Features:
- Multiple chorangiomas - the difference between chorangioma and chorangiomatosis is not well defined.[101]
Images:
Chorangiosis
General
- Should not be confused with chorangioma.
- Relative common among babies in ICU ~5%.[102]
Associations:
Gross
- Usually not seen on gross pathology.
Microscopic
Features:
- Increased blood vessels in the terminal villi.
- Lesion not well circumscribed.
- Villi tend to be larger and have centrally placed blood vessels.[106]
Notes:
- Normal villi have up to five vascular channels.[104]
Images:
{kind=link}
{kind=link}
Sign out
PLACENTA, UMBILICAL CORD AND FETAL MEMBRANES, CESAERIAN SECTION: - THREE VESSEL UMBILICAL CORD WITHIN NORMAL LIMITS. - FETAL MEMBRANES WITHIN MECONIUM STAINING OF THE AMNION, NEGATIVE FOR CHORIOAMNIONITIS. - PLACENTAL DISC WITH: -- CHORANGIOSIS. -- FOCAL PERIVILLOUS FIBRIN DEPOSITION. COMMENT: Chorangiosis is a non-specific finding that may be associated with diabetes, smoking or high altitude.
Other
Fetus papyraceus
- May be spelled foetus papyraceus.
- AKA fetus compressus.
General
- Remnant of a dead fetus usu. from a twin pregnancy.
- No clinical consequence for mother and remaining fetus.
Clinical:[107]
- Documented multiple gestation by imaging.
- Elevated AFP.
- May be a "fetal reduction" in the context of in vitro fertilization (IVF).
Note:
- "Papyraceus" = paper-like.
Gross
- Pale yellow flattened disk or plaque with a pigmented macule[107] - on membranes or placental disc.
Microscopic
Features:
- Fetal structures - such as:
- Cartilage.
- Bone.
Images:
Placental mesenchymal dysplasia
- Abbreviated PMD.
General
- Very rare ~ 70 reported cases.[109]
- Etiology unknown.
Associations:[109]
- IUGR ~ 50% of cases.
- Fetal demise ~ 40-45% of cases.
- Beckwith-Wiedemann syndrome.
Gross
Features:[110]
- Placentomegaly.
- Grape-like vesicles.
DDx - gross:
Image:
Microscopic
Features:[111]
- Stem villi with edema (hydropic changes) and few blood vessels.
- Paucivascular (few blood vessels) or avascular (terminal) villi.
Note:
- Stem villi = large villi with a fibrotic core and (fetal) arteries and veins.[112]
Image:
See also
References
- ↑ Yetter JF (March 1998). "Examination of the placenta". Am Fam Physician 57 (5): 1045–54. PMID 9518951.
- ↑ Hargitai B, Marton T, Cox PM (August 2004). "Best practice no 178. Examination of the human placenta". J. Clin. Pathol. 57 (8): 785–92. doi:10.1136/jcp.2003.014217. PMC 1770400. PMID 15280396. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1770400/.
- ↑ URL: http://smj.sma.org.sg/5012/5012ra1.pdf. Accessed on: 11 February 2011.
- ↑ CS. 8 February 2011.
- ↑ URL: http://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=5069. Accessed on: 7 July 2010.
- ↑ 6.0 6.1 6.2 6.3 Sternberg, Stephen S. (1997). Histology for Pathologists (2nd ed.). Lippincott Williams & Wilkins. pp. 974. ISBN 978-0397517183.
- ↑ Sternberg, Stephen S. (1997). Histology for Pathologists (2nd ed.). Lippincott Williams & Wilkins. pp. 977. ISBN 978-0397517183.
- ↑ Narasimha, A.; Vasudeva, DS.. "Spectrum of changes in placenta in toxemia of pregnancy.". Indian J Pathol Microbiol 54 (1): 15-20. doi:10.4103/0377-4929.77317. PMID 21393870.
- ↑ URL: http://zulekhahospitals.com/uploads/files/Sub-chorionic.pdf. Accessed on: 17 August 2012.
- ↑ J Anat. Soc. India 49(2) 149-152 (2000). Available at: http://www.indmedica.com/anatomy/aindex1.cfm?anid=41. Accessed on: January 21, 2009.
- ↑ Winters R, Waters BL (December 2008). "What is adequate sampling of extraplacental membranes?: a randomized, prospective analysis". Arch. Pathol. Lab. Med. 132 (12): 1920–3. PMID 19061291.
- ↑ Lester, Susan Carole (2005). Manual of Surgical Pathology (2nd ed.). Saunders. pp. 461. ISBN 978-0443066450.
- ↑ CS. 7 February 2011.
- ↑ AFIP Placental pathol. ISBN: 1-881041-89-1. P.312
- ↑ AFIP Placental pathol. ISBN: 1-881041-89-1. P.312
- ↑ Fox, Harold; Sebire, Neil J. (2007). Pathology of the Placenta (Major Problems in Pathology) (3rd ed.). Saunders. pp. 559-561. ISBN 978-1416025924.
- ↑ URL: http://quizlet.com/5793113/ob-flash-cards/. Accessed on: 13 January 2012.
- ↑ Clarson, C.; Tevaarwerk, GJ.; Harding, PG.; Chance, GW.; Haust, MD.. "Placental weight in diabetic pregnancies.". Placenta 10 (3): 275-81. PMID 2771897.
- ↑ Hindmarsh, PC.; Geary, MP.; Rodeck, CH.; Jackson, MR.; Kingdom, JC. (Aug 2000). "Effect of early maternal iron stores on placental weight and structure.". Lancet 356 (9231): 719-23. PMID 11085691.
- ↑ 20.0 20.1 20.2 20.3 20.4 20.5 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 464. ISBN 978-0781765275.
- ↑ Srinivasan R, Arora RS (January 2005). "Do well infants born with an isolated single umbilical artery need investigation?". Arch. Dis. Child. 90 (1): 100–1. doi:10.1136/adc.2004.062372. PMC 1720078. PMID 15613529. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1720078/.
- ↑ Lilja M (July 1994). "Infants with single umbilical artery studied in a national registry. 3: A case control study of risk factors". Paediatr Perinat Epidemiol 8 (3): 325–33. PMID 7997408.
- ↑ URL: http://www.glowm.com/?p=glowm.cml/section_view&articleid=151. Accessed on: 8 January 2011.
- ↑ 24.0 24.1 Hasegawa J, Farina A, Nakamura M, et al. (December 2010). "Analysis of the ultrasonographic findings predictive of vasa previa". Prenat. Diagn. 30 (12-13): 1121–5. doi:10.1002/pd.2618. PMID 20872421.
- ↑ 25.0 25.1 Airas U, Heinonen S (April 2002). "Clinical significance of true umbilical knots: a population-based analysis". Am J Perinatol 19 (3): 127–32. doi:10.1055/s-2002-25311. PMID 12012287.
- ↑ 26.0 26.1 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 464. ISBN 978-0781765275.
- ↑ CS. 7 February 2011.
- ↑ 28.0 28.1 28.2 28.3 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 465. ISBN 978-0781765275.
- ↑ Khong TY (December 2010). "Evidence-based pathology: umbilical cord coiling". Pathology 42 (7): 618–22. doi:10.3109/00313025.2010.520309. PMID 21080869.
- ↑ PMID 16076615.
- ↑ URL: http://flylib.com/books/en/2.953.1.49/1/. Accessed on: 10 January 2011.
- ↑ URL: http://library.med.utah.edu/WebPath/PLACHTML/PLAC042.html. Accessed on: 12 January 2011.
- ↑ 33.0 33.1 33.2 33.3 33.4 33.5 33.6 Adeniran, AJ.; Stanek, J. (Dec 2007). "Amnion nodosum revisited: clinicopathologic and placental correlations.". Arch Pathol Lab Med 131 (12): 1829-33. doi:10.1043/1543-2165(2007)131[1829:ANRCAP]2.0.CO;2. PMID 18081444.
- ↑ CS. 7 February 2011.
- ↑ ALS. 6 Febraury 2009.
- ↑ Miller PW, Coen RW, Benirschke K (October 1985). "Dating the time interval from meconium passage to birth". Obstet Gynecol 66 (4): 459–62. PMID 2413412.
- ↑ Funai EF, Labowsky AT, Drewes CE, Kliman HJ (January 2009). "Timing of fetal meconium absorption by amnionic macrophages". Am J Perinatol 26 (1): 93–7. doi:10.1055/s-0028-1103028. PMID 19031358.
- ↑ Povýsil C, Bennett R, Povýsilová V (January 2001). "CD 68 positivity of the so-called meconium corpuscles in human foetal intestine". Cesk Patol 37 (1): 7–9. PMID 11268705.
- ↑ Sienko A, Altshuler G (September 1999). "Meconium-induced umbilical vascular necrosis in abortuses and fetuses: a histopathologic study for cytokines". Obstet Gynecol 94 (3): 415?0. PMID 10472870.
- ↑ Sienko A, Altshuler G (September 1999). "Meconium-induced umbilical vascular necrosis in abortuses and fetuses: a histopathologic study for cytokines". Obstet Gynecol 94 (3): 415?0. PMID 10472870.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 463. ISBN 978-0781765275.
- ↑ Chew, RH.; Silberberg, BK. (Apr 1990). "Possible association of acute inflammatory exudate in chorioamnionitis and amniotic squamous metaplasia.". Am J Clin Pathol 93 (4): 582-5. PMID 2321592.
- ↑ CS. 7 February 2011.
- ↑ URL: http://flylib.com/books/en/2.953.1.49/1/. Accessed on: 10 January 2011.
- ↑ Suzuki, S. (Feb 2008). "Clinical significance of pregnancies with circumvallate placenta.". J Obstet Gynaecol Res 34 (1): 51-4. doi:10.1111/j.1447-0756.2007.00682.x. PMID 18226129.
- ↑ URL: http://www.med.yale.edu/obgyn/kliman/placenta/articles/EOR_Placenta/Trophtoplacenta.html. Accessed on: 28 May 2011.
- ↑ 47.0 47.1 Baergen, Rebecca N. (2011). Manual of Pathology of the Human Placenta (2nd ed.). Springer. pp. 375. ISBN 978-1441974938.
- ↑ Arizawa, M.; Nakayama, M.; Kidoguchi, K. (Jun 1991). "[Correlation of placental villous immaturity and dysmaturity with clinical control of maternal diabetes].". Nihon Sanka Fujinka Gakkai Zasshi 43 (6): 595-602. PMID 1856519.
- ↑ Stallmach, T.; Hebisch, G. (Jul 2004). "Placental pathology: its impact on explaining prenatal and perinatal death.". Virchows Arch 445 (1): 9-16. doi:10.1007/s00428-004-1032-2. PMID 15138817.
- ↑ 50.0 50.1 Daskalakis, G.; Marinopoulos, S.; Krielesi, V.; Papapanagiotou, A.; Papantoniou, N.; Mesogitis, S.; Antsaklis, A. (2008). "Placental pathology in women with gestational diabetes.". Acta Obstet Gynecol Scand 87 (4): 403-7. doi:10.1080/00016340801908783. PMID 18382864.
- ↑ 51.0 51.1 Tantbirojn, P.; Crum, CP.; Parast, MM. (Jul 2008). "Pathophysiology of placenta creta: the role of decidua and extravillous trophoblast.". Placenta 29 (7): 639-45. doi:10.1016/j.placenta.2008.04.008. PMID 18514815.
- ↑ Wortman, AC.; Alexander, JM. (Mar 2013). "Placenta accreta, increta, and percreta.". Obstet Gynecol Clin North Am 40 (1): 137-54. doi:10.1016/j.ogc.2012.12.002. PMID 23466142.
- ↑ 53.0 53.1 Böcker, Werner; Denk, Helmut; Heitz, Philipp U.; Moch, Holger (2008). [Pathologie] (4th ed.). Urban & Fischer Verlag/Elsevier GmbH. pp. 974. ISBN 978-3437423826.
- ↑ URL: http://library.med.utah.edu/WebPath/EXAM/IMGQUIZ/plfrm.html. Accessed on: 3 December 2011.
- ↑ Tikkanen M, Nuutila M, Hiilesmaa V, Paavonen J, Ylikorkala O (2006). "Clinical presentation and risk factors of placental abruption". Acta Obstet Gynecol Scand 85 (6): 700–5. doi:10.1080/00016340500449915. PMID 16752262.
- ↑ CS. 7 February 2011.
- ↑ 57.0 57.1 Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 1106. ISBN 0-7216-0187-1.
- ↑ 58.0 58.1 58.2 58.3 58.4 Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Oberman, Harold A; Reuter, Victor E (2004). Sternberg's Diagnostic Surgical Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 2311. ISBN 978-0781740517.
- ↑ Martinelli, P.; Sarno, L.; Maruotti, GM.; Paludetto, R. (Oct 2012). "Chorioamnionitis and prematurity: a critical review.". J Matern Fetal Neonatal Med 25 Suppl 4: 29-31. doi:10.3109/14767058.2012.714981. PMID 22958008.
- ↑ Roberts, DJ.; Celi, AC.; Riley, LE.; Onderdonk, AB.; Boyd, TK.; Johnson, LC.; Lieberman, E. (2012). "Acute histologic chorioamnionitis at term: nearly always noninfectious.". PLoS One 7 (3): e31819. doi:10.1371/journal.pone.0031819. PMID 22412842.
- ↑ Tita, AT.; Andrews, WW. (Jun 2010). "Diagnosis and management of clinical chorioamnionitis.". Clin Perinatol 37 (2): 339-54. doi:10.1016/j.clp.2010.02.003. PMC 3008318. PMID 20569811. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3008318/.
- ↑ 62.0 62.1 Lahra, MM.; Jeffery, HE. (Jan 2004). "A fetal response to chorioamnionitis is associated with early survival after preterm birth.". Am J Obstet Gynecol 190 (1): 147-51. doi:10.1016/j.ajog.2003.07.012. PMID 14749651.
- ↑ Vedovato, S.; Zanardo, V. (Jun 2010). "[Chorioamnionitis and inflammatory disease in the premature newborn infant].". Minerva Pediatr 62 (3 Suppl 1): 155-6. PMID 21090086.
- ↑ 64.0 64.1 Redline RW (October 2007). "Villitis of unknown etiology: noninfectious chronic villitis in the placenta". Hum. Pathol. 38 (10): 1439–46. doi:10.1016/j.humpath.2007.05.025. PMID 17889674.
- ↑ Feeley L, Mooney EE (2010). "Villitis of unknown aetiology: correlation of recurrence with clinical outcome". J Obstet Gynaecol 30 (5): 476–9. doi:10.3109/01443611003802339. PMID 20604650.
- ↑ Sherman, C. 7 February 2011.
- ↑ URL: http://jcp.bmj.com/content/61/12/1254.abstract. Accessed on: 11 January 2011.
- ↑ 68.0 68.1 URL: http://www.flickr.com/photos/jian-hua_qiao_md/3954021698/. Accessed on: 11 January 2011.
- ↑ 69.0 69.1 Jacques, SM.; Qureshi, F. (Oct 1993). "Chronic intervillositis of the placenta.". Arch Pathol Lab Med 117 (10): 1032-5. PMID 8215826.
- ↑ 70.0 70.1 Rota, C.; Carles, D.; Schaeffer, V.; Guyon, F.; Saura, R.; Horovitz, J. (Nov 2006). "[Perinatal prognosis of pregnancies complicated by placental chronic intervillitis].". J Gynecol Obstet Biol Reprod (Paris) 35 (7): 711-9. PMID 17088773.
- ↑ 71.0 71.1 Edmondson, N.; Bocking, A.; Machin, G.; Rizek, R.; Watson, C.; Keating, S.. "The prevalence of chronic deciduitis in cases of preterm labor without clinical chorioamnionitis.". Pediatr Dev Pathol 12 (1): 16-21. doi:10.2350/07-04-0270.1. PMID 18171100.
- ↑ URL: http://www.medind.nic.in/jae/t04/i1/jaet04i1p27.pdf. Accessed on: 16 April 2012.
- ↑ Becroft, DM.; Thompson, JM.; Mitchell, EA. (Apr 2002). "The epidemiology of placental infarction at term.". Placenta 23 (4): 343-51. doi:10.1053/plac.2001.0777. PMID 11969346.
- ↑ 74.0 74.1 Weedman Molavi, Diana (2008). The Practice of Surgical Pathology: A Beginner's Guide to the Diagnostic Process (1st ed.). Springer. pp. 178. ISBN 978-0387744858.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 1109. ISBN 0-7216-0187-1.
- ↑ URL: http://path.upmc.edu/cases/case75/micro.html. Accessed on: 6 January 2011.
- ↑ 77.0 77.1 77.2 Sebire NJ, Backos M, Goldin RD, Regan L (May 2002). "Placental massive perivillous fibrin deposition associated with antiphospholipid antibody syndrome". BJOG 109 (5): 570–3. PMID 12066949. http://www3.interscience.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=1470-0328&date=2002&volume=109&issue=5&spage=570.
- ↑ Baergen, Rebecca N. (2011). Manual of Pathology of the Human Placenta (2nd ed.). Springer. pp. 327. ISBN 978-1441974938.
- ↑ Baergen, Rebecca N. (2011). Manual of Pathology of the Human Placenta (2nd ed.). Springer. pp. 367. ISBN 978-1441974938.
- ↑ 80.0 80.1 80.2 Roberts, DJ.; Post, MD. (Dec 2008). "The placenta in pre-eclampsia and intrauterine growth restriction.". J Clin Pathol 61 (12): 1254-60. doi:10.1136/jcp.2008.055236. PMID 18641412.
- ↑ 81.0 81.1 Katzman, PJ.; Genest, DR.. "Maternal floor infarction and massive perivillous fibrin deposition: histological definitions, association with intrauterine fetal growth restriction, and risk of recurrence.". Pediatr Dev Pathol 5 (2): 159-64. doi:10.1007/s10024-001-0195-y. PMID 11910510.
- ↑ Kanfer, A.; Bruch, JF.; Nguyen, G.; He, CJ.; Delarue, F.; Flahault, A.; Nessmann, C.; Uzan, S. (Jan 1996). "Increased placental antifibrinolytic potential and fibrin deposits in pregnancy-induced hypertension and preeclampsia.". Lab Invest 74 (1): 253-8. PMID 8569189.
- ↑ 83.0 83.1 Baergen, Rebecca N. (2011). Manual of Pathology of the Human Placenta (2nd ed.). Springer. pp. 368. ISBN 978-1441974938.
- ↑ AFIP - Placental Pathology. P.135. ISBN: 1-881041-89-1. 2004.
- ↑ 85.0 85.1 Marchetti, D.; Belviso, M.; Fulcheri, E. (Mar 2009). "A case of stillbirth: the importance of placental investigation in medico-legal practice.". Am J Forensic Med Pathol 30 (1): 64-8. doi:10.1097/PAF.0b013e318187387e. PMID 19237859.
- ↑ 86.0 86.1 Kraus FT, Acheen VI (July 1999). "Fetal thrombotic vasculopathy in the placenta: cerebral thrombi and infarcts, coagulopathies, and cerebral palsy". Hum. Pathol. 30 (7): 759–69. PMID 10414494. Cite error: Invalid
<ref>tag; name "pmid10414494" defined multiple times with different content - ↑ URL: http://jcp.bmj.com/content/61/12/1254.abstract. Accessed on: 12 January 2011.
- ↑ URL: http://gut.bmj.com/content/41/3/354.full. Accessed on: 12 January 2011.
- ↑ URL: http://www.womenandinfants.org/fertilityandpregnancy/current-topics-in-perinatal-pathology.cfm. Accessed on: 17 December 2012.
- ↑ Stevens NG, Sander CH (October 1984). "Placental hemorrhagic endovasculitis: risk factors and impact on pregnancy outcome". Int J Gynaecol Obstet 22 (5): 393–7. PMID 6151926.
- ↑ Sander CM, Gilliland D, Akers C, McGrath A, Bismar TA, Swart-Hills LA (February 2002). "Livebirths with placental hemorrhagic endovasculitis: interlesional relationships and perinatal outcomes". Arch. Pathol. Lab. Med. 126 (2): 157–64. PMID 11825110.
- ↑ 92.0 92.1 Soma H, Yoshida K, Mukaida T, Tabuchi Y (1982). "Morphologic changes in the hypertensive placenta". Contrib Gynecol Obstet 9: 58–75. PMID 6754249.
- ↑ CS. 7 February 2011.
- ↑ AFIP - Placental Pathology. P.122. ISBN: 1-881041-89-1. 2004.
- ↑ Naicker, T.; Khedun, SM.; Moodley, J.; Pijnenborg, R. (Aug 2003). "Quantitative analysis of trophoblast invasion in preeclampsia.". Acta Obstet Gynecol Scand 82 (8): 722-9. PMID 12848643.
- ↑ URL: http://path.upmc.edu/cases/case75.html. Accessed on: 2 January 2012.
- ↑ Vinnars MT, Wijnaendts LC, Westgren M, Bolte AC, Papadogiannakis N, Nasiell J (May 2008). "Severe preeclampsia with and without HELLP differ with regard to placental pathology". Hypertension 51 (5): 1295–9. doi:10.1161/HYPERTENSIONAHA.107.104844. PMID 18362224.
- ↑ Ornstein MH, Rand JH (July 1994). "An association between refractory HELLP syndrome and antiphospholipid antibodies during pregnancy; a report of 2 cases". J. Rheumatol. 21 (7): 1360–4. PMID 7966086.
- ↑ 99.0 99.1 99.2 99.3 99.4 Amer HZ, Heller DS (2010). "Chorangioma and related vascular lesions of the placenta--a review". Fetal Pediatr Pathol 29 (4): 199–206. doi:10.3109/15513815.2010.487009. PMID 20594143.
- ↑ Lež C, Fures R, Hrgovic Z, Belina S, Fajdic J, Münstedt K (2010). "Chorangioma placentae". Rare Tumors 2 (4): e67. doi:10.4081/rt.2010.e67. PMC 3019602. PMID 21234259. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3019602/.
- ↑ URL: http://path.upmc.edu/cases/case655/dx.html. Accessed on: 28 January 2012.
- ↑ URL: http://www.bhj.org/journal/2009_5102_april/download/pg251-252.pdf. Accessed on: 26 July 2011.
- ↑ Altshuler, G. (Jan 1984). "Chorangiosis. An important placental sign of neonatal morbidity and mortality.". Arch Pathol Lab Med 108 (1): 71-4. PMID 6546343.
- ↑ 104.0 104.1 De La Ossa, MM.; Cabello-Inchausti, B.; Robinson, MJ. (Sep 2001). "Placental chorangiosis.". Arch Pathol Lab Med 125 (9): 1258. doi:10.1043/0003-9985(2001)1251258:PC2.0.CO;2. PMID 11520290. http://www.archivesofpathology.org/doi/full/10.1043/0003-9985%282001%29125%3C1258:PC%3E2.0.CO;2.
- ↑ URL: http://path.upmc.edu/cases/case655/dx.html. Accessed on: 28 January 2012.
- ↑ E. Latta. 26 July 2011.
- ↑ 107.0 107.1 Baergen, Rebecca N. (2011). Manual of Pathology of the Human Placenta (2nd ed.). Springer. pp. 141. ISBN 978-1441974938.
- ↑ URL: http://www.neonet.ch/en/03_Case_of_the_month/archive/11_dermatologic_disorders/2002_10.asp. Accessed on: 3 January 2012.
- ↑ 109.0 109.1 Pham, T.; Steele, J.; Stayboldt, C.; Chan, L.; Benirschke, K. (Jul 2006). "Placental mesenchymal dysplasia is associated with high rates of intrauterine growth restriction and fetal demise: A report of 11 new cases and a review of the literature.". Am J Clin Pathol 126 (1): 67-78. doi:10.1309/RV45-HRD5-3YQ2-YFTP. PMID 16753607.
- ↑ Rohilla, M.; Siwatch, S.; Jain, V.; Nijhawan, R. (2012). "Placentomegaly and placental mesenchymal dysplasia.". BMJ Case Rep 2012. doi:10.1136/bcr-2012-007777. PMID 23266781.
- ↑ 111.0 111.1 111.2 Umazume, T.; Kataoka, S.; Kamamuta, K.; Tanuma, F.; Sumie, A.; Shirogane, T.; Kudou, T.; Ikeda, H. (2011). "Placental mesenchymal dysplasia, a case of intrauterine sudden death of fetus with rupture of cirsoid periumbilical chorionic vessels.". Diagn Pathol 6: 38. doi:10.1186/1746-1596-6-38. PMID 21513565.
- ↑ Demir, R.; Kosanke, G.; Kohnen, G.; Kertschanska, S.; Kaufmann, P.. "Classification of human placental stem villi: review of structural and functional aspects.". Microsc Res Tech 38 (1-2): 29-41. doi:10.1002/(SICI)1097-0029(19970701/15)38:1/229::AID-JEMT53.0.CO;2-P. PMID 9260835.
Recommended reading
- Langston C, Kaplan C, Macpherson T, et al. (May 1997). "Practice guideline for examination of the placenta: developed by the Placental Pathology Practice Guideline Development Task Force of the College of American Pathologists". Arch. Pathol. Lab. Med. 121 (5): 449–76. PMID 9167599.
- Baergen, Rebecca N. (2005). Manual of Benirschke and Kaufmann's Pathology of the Human Placenta (1st ed.). Springer. ISBN 978-0387220895.