|
|
| (160 intermediate revisions by one other user not shown) |
| Line 1: |
Line 1: |
| The '''prostate gland''' adds juice to the sperm. In old men it creates lotsa problems... [[nodular hyperplasia]] (commonly called BPH or [[benign prostatic hyperplasia]]) and cancer (adenocarcinoma). | | [[Image:Prostatelead.jpg|thumb|right|200px|The prostate gland and its surrounding structures. (WC/NCI)]] |
| | The '''prostate gland''' adds juice to the sperm. In old men it creates a lot of problems... [[nodular hyperplasia]] (commonly called BPH or [[benign prostatic hyperplasia]]) and cancer (usually adenocarcinoma). |
|
| |
|
| =Normal= | | [[Prostate cancer]] is such a big topic it is dealt with in its own article. |
| ==Prostate== | | |
| | The female homologue of the prostate gland is considered to be Skene's gland.<ref name=pmid8522254>{{Cite journal | last1 = Dodson | first1 = MK. | last2 = Cliby | first2 = WA. | last3 = Pettavel | first3 = PP. | last4 = Keeney | first4 = GL. | last5 = Podratz | first5 = KC. | title = Female urethral adenocarcinoma: evidence for more than one tissue of origin? | journal = Gynecol Oncol | volume = 59 | issue = 3 | pages = 352-7 | month = Dec | year = 1995 | doi = 10.1006/gyno.1995.9963 | PMID = 8522254 }}</ref> |
| | |
| | =Normal prostate gland= |
| | ==Anatomy== |
| | Divided into three zones:<ref name=pmid2456702>{{Cite journal | last1 = McNeal | first1 = JE. | title = Normal histology of the prostate. | journal = Am J Surg Pathol | volume = 12 | issue = 8 | pages = 619-33 | month = Aug | year = 1988 | doi = | PMID = 2456702 }} |
| | </ref> |
| | #Peripheral zone - posterior aspect, palpable with digit. |
| | #*Classic location for [[prostate cancer|cancer]]. |
| | #Central zone - considered resistant to disease. |
| | #Transition zone - usual location for [[nodular hyperplasia of the prostate|nodular hyperplasia]]. |
| | |
| | ==Histology== |
| *Glands have two cell layers (similar to glands in breast). | | *Glands have two cell layers (similar to glands in breast). |
| **Second cell layer may be difficult to see (like in breast). | | **Second cell layer may be difficult to see (like in breast). |
| *Epithelium in glands is "folded" or "tufted". | | *Epithelium in glands is "folded" or "tufted". |
| **Very important - helps on differentiate from Gleason pattern 3. | | **Very important - helps to differentiate from Gleason pattern 3. |
| *Luminal epithelium often clear cytoplasm. | | *Luminal epithelium often clear cytoplasm. |
| *Single nucleus. | | *Single nucleus. |
| Line 23: |
Line 36: |
|
| |
|
| Notes: | | Notes: |
| *Tufted epithelium is a strong indicator of benignancy; however two uncommon prostate cancer typically have tufted epithelium: | | *Tufted epithelium is a strong indicator of benignancy; however two uncommon prostate cancer variants typically have tufted epithelium: |
| **Pseudohyperplastic adenocarcinoma. | | **[[Pseudohyperplastic adenocarcinoma]]. |
| **Foamy gland carcinoma. | | **[[Foamy gland carcinoma]]. |
|
| |
|
| Images: | | ====Images==== |
| *[http://commons.wikimedia.org/wiki/File:Corpora_amylacea_low_mag.jpg Benign prostate with corpora amylacea - low mag. (WC)].
| | <gallery> |
| *[http://commons.wikimedia.org/wiki/File:Corpora_amylacea_high_mag.jpg Benign prostate with corpora amylacea - high mag. (WC)].
| | Image:Corpora_amylacea_low_mag.jpg | Benign prostate with corpora amylacea - low mag. (WC/Nephron) |
| | Image:Corpora_amylacea_high_mag.jpg | Benign prostate with corpora amylacea - high mag. (WC/Nephron) |
| | </gallery> |
|
| |
|
| ===IHC of normal prostate===
| | ==IHC of normal prostate== |
| Normal prostate: | | Normal prostate: |
| *AMACR -ve (mark epithelial cells). | | *[[AMACR]] -ve (mark epithelial cells). |
| *CK5/6 +ve,<ref name=pmid19605815>{{Cite journal | last1 = Trpkov | first1 = K. | last2 = Bartczak-McKay | first2 = J. | last3 = Yilmaz | first3 = A. | title = Usefulness of cytokeratin 5/6 and AMACR applied as double sequential immunostains for diagnostic assessment of problematic prostate specimens. | journal = Am J Clin Pathol | volume = 132 | issue = 2 | pages = 211-20; quiz 307 | month = Aug | year = 2009 | doi = 10.1309/AJCPGFJP83IXZEUR | PMID = 19605815 }}</ref> p63 +ve, HMWCK +ve (mark basal cells). | | *[[CK5/6]] +ve,<ref name=pmid19605815>{{Cite journal | last1 = Trpkov | first1 = K. | last2 = Bartczak-McKay | first2 = J. | last3 = Yilmaz | first3 = A. | title = Usefulness of cytokeratin 5/6 and AMACR applied as double sequential immunostains for diagnostic assessment of problematic prostate specimens. | journal = Am J Clin Pathol | volume = 132 | issue = 2 | pages = 211-20; quiz 307 | month = Aug | year = 2009 | doi = 10.1309/AJCPGFJP83IXZEUR | PMID = 19605815 }}</ref> p63 +ve, HMWCK +ve (mark basal cells). |
| *PSA (prostate-specific antigen) +ve, PSAP (prostatic-specific acid phosphatase) +ve. | | *PSA ([[prostate-specific antigen]]) +ve, PSAP ([[prostatic-specific acid phosphatase]]) +ve. |
|
| |
|
| ==Other accessory glands== | | ==Sign out== |
| ===Bulbourethral gland=== | | ===Staining slightly abnormal - morphology not definitely abnormal=== |
| *AKA ''Cowper's gland''.
| | <pre> |
| *Mucinous glands at the apex of the prostate.
| | COMMENT: |
| **Resemble (mucinous) [[salivary gland]]s.<ref>PR. September 2009.</ref>
| | Very focal AMACR staining is seen; this is interpreted as negative, in the |
| | context of no definite cytologic changes. The basal cells appear to be |
| | preserved in all of the tissue sampled. |
| | </pre> |
|
| |
|
| Image: [http://pathology.mc.duke.edu/research/histo_course/mixed_saliv.jpg Mucinous/serous salivary gland (duke.edu)].
| | ===Compatible with previous biopsy=== |
| ===Seminal vesicles=== | | <pre> |
| *Fern-like architecture - epithelial component clustered closely, looks like it connects.
| | COMMENT: |
| **Epithelium surrounded by a thick layer of muscle (>10 cells across ~80 microns).
| | Siderophages are seen in several cores; this is compatible with the history |
| *Lipofuscin (coarse cytoplasmic yellow granules approximately 1-2 micrometers) - '''key feature'''.
| | of a previous biopsy. |
| *Nucleoli - common.
| | </pre> |
| *Nuclear inclusions - common.
| |
|
| |
|
| Notes:
| | =Other accessory glands= |
| *The ''ejaculatory ducts'' have the same epithelium as the seminal vesicles.<ref name=pmid12657938>{{cite journal |author=Leroy X, Ballereau C, Villers A, ''et al.'' |title=MUC6 is a marker of seminal vesicle-ejaculatory duct epithelium and is useful for the differential diagnosis with prostate adenocarcinoma |journal=Am. J. Surg. Pathol. |volume=27 |issue=4 |pages=519–21 |year=2003 |month=April |pmid=12657938 |doi= |url=}}</ref> | | ==Bulbourethral gland== |
| | *[[AKA]] ''Cowper's gland''. |
| | {{Main|Bulbourethral gland}} |
|
| |
|
| Images:
| | ==Seminal vesicles== |
| *[http://commons.wikimedia.org/wiki/File:Seminal_vesicle_low_mag.jpg SV - showing fern-like architecture (WC)].
| | {{Main|Seminal vesicles}} |
| *[http://commons.wikimedia.org/wiki/File:Seminal_vesicle_high_mag.jpg SV - looking vaguely like to prostate adenocarcinoma (WC)].
| |
| *[http://commons.wikimedia.org/wiki/File:Seminal_vesicle_intermed_mag.jpg SV - looks a bit like prostate but lumina too big (WC)].
| |
| *[http://dspace.udel.edu:8080/dspace/bitstream/19716/2016/1/cmrsvlm3.GIF SV (udel.edu)].
| |
|
| |
|
| =Specimens= | | =Specimens= |
| *Prostate core biopsy - done transrectal. | | *[[Prostate core biopsy]] - done transrectal. |
| *Radical prostatectomy - includes the seminal vesicles. | | *[[Prostate chips]] (from a ''transurethral resection of the prostate'', abbreviated ''TURP'') - usu. done for [[nodular hyperplasia of the prostate gland]]; may be done in the context of obstructing cancer. |
| *Radical cystoprostatectomy - includes the urinary bladder and seminal vesicles.<ref>URL: [http://www.cancer.gov/dictionary?cdrid=446218 http://www.cancer.gov/dictionary?cdrid=446218]. Accessed on: 23 February 2012.</ref> | | *[[Radical prostatectomy]] - includes the [[seminal vesicles]]. |
| | *[[Radical cystoprostatectomy]] - includes the [[urinary bladder]] and [[seminal vesicles]].<ref>URL: [http://www.cancer.gov/dictionary?cdrid=446218 http://www.cancer.gov/dictionary?cdrid=446218]. Accessed on: 23 February 2012.</ref> |
| | |
| | =Approach= |
| | *Know the common diagnoses well. |
| | *Core biopsies - scan the slides with the 10x objective. |
|
| |
|
| =Common diagnoses= | | ==Common diagnoses== |
| *Benign. | | *Benign. |
| **Atrophy - may resemble adenocarcinoma - typically not reported. | | **[[Atrophy of the prostate|Atrophy]] - may resemble adenocarcinoma - typically not reported. |
| **Adenosis - may resemble adenocarcinoma - typically not reported. | | **[[Adenosis of the prostate|Adenosis]] - may resemble adenocarcinoma - typically not reported. |
| *Prostate adenocarcinoma. | | *[[Prostate adenocarcinoma]]. |
| **Most common Grade is 3+3=6. | | *[[HGPIN]] (high-grade prostatic intraepithelial neoplasia) - prostate adenocarcinoma precursor lesion. |
| *HGPIN (high-grade prostatic intraepithelial neoplasia) - prostate adenocarcinoma precursor lesion.
| | *[[ASAP]] (atypical small acinar proliferation) - used if you have a few abnormal appearing glands... but can't decide between prostate adenocarcinoma & benign. |
| *ASAP (atypical small acinar proliferation) - used if you have a few abnormal appearing glands... but can't decide between prostate adenocarcinoma & benign. | |
| *Chronic inflammation. | | *Chronic inflammation. |
| *Acute inflammation - can result in an elevated PSA and may have prompted the biopsy you're looking at. | | *Acute inflammation - can result in an elevated PSA and may have prompted the biopsy you're looking at. |
| *Nodular hyperplasia of the prostate; AKA ''benign prostatic hypertrophy'' (BPH). | | *[[Nodular hyperplasia of the prostate]]; [[AKA]] ''benign prostatic hypertrophy'' (BPH). |
| **Not diagnosed on needle biopsies. | | **Not diagnosed on needle biopsies. |
| **''BPH'' is technically incorrect -- the process is a hyperplasia. | | **''BPH'' is technically incorrect -- the process is a hyperplasia. |
| Line 82: |
Line 102: |
|
| |
|
| =Clinical history= | | =Clinical history= |
| *PSA (serum). | | {{Main|Prostate specific antigen}} |
| | *[[PSA]] (serum). |
| ** >10 ng/mL worrisome for prostate cancer. | | ** >10 ng/mL worrisome for prostate cancer. |
| ** Normal is age dependent - increases with age, usu. cut-off ~ 4 ng/mL. | | ** Normal is age dependent - increases with age, usu. cut-off ~ 4 ng/mL. |
| *HIFU = ''High Intensity Focused Ultrasound'' - an ablation procedure for prostate cancer.<ref>URL: [http://www.internationalhifu.com/what-is-hifu-mainmenu-132.html http://www.internationalhifu.com/what-is-hifu-mainmenu-132.html]. Accessed on: 15 June 2010.</ref> | | *HIFU = ''High Intensity Focused Ultrasound'' - an ablation procedure for prostate cancer.<ref>URL: [http://www.internationalhifu.com/what-is-hifu-mainmenu-132.html http://www.internationalhifu.com/what-is-hifu-mainmenu-132.html]. Accessed on: 15 June 2010.</ref> |
|
| |
|
| =Specific conditions= | | =Benign changes and remnants= |
| ==Prostatic nodular hyperplasia== | | ==Adenosis of the prostate gland== |
| *[[AKA]] ''nodular hyperplasia of the prostate'', AKA ''benign prostatic hyperplasia'' (abbreviated BPH). | | *[[AKA]] ''atypical adenomatous hyperplasia of the prostate gland'' (or ''atypical adenomatous hyperplasia''). |
| | {{Main|Adenosis of the prostate gland}} |
|
| |
|
| ===General=== | | ==Basal cell hyperplasia of the prostate== |
| *Very common.
| | {{Main|Basal cell hyperplasia of the prostate}} |
| *Incidence increases with age.
| |
|
| |
|
| Clinical - mnemonic ''I WISH 2p'':<ref>TN06 U5</ref>
| | ==Atrophy of the prostate== |
| *Intermittency.
| | *[[AKA]] ''atrophy''. |
| *Weak stream. | | *[[AKA]] ''prostatic atrophy''. |
| *Incomplete emptying. | | *[[AKA]] ''atrophy of the prostate gland''. |
| *Straining.
| | {{Main|Atrophy of the prostate gland}} |
| *Hesitancy.
| |
| *Post-void dribbling.
| |
| *Prolonged voiding.
| |
|
| |
|
| ===Microscopic=== | | ==Mesonephric remnant of the prostate gland== |
| Features:
| | {{Main|Mesonephric remnant of the prostate gland}} |
| *Stromal and/or glandular hyperplasia.
| |
|
| |
|
| Image:
| | =Benign conditions= |
| [http://commons.wikimedia.org/wiki/File:Nodular_hyperplasia_of_the_prostate.jpg Prostatic nodular hyperplasia (WC)]. | | ==Prostatic nodular hyperplasia== |
| | *[[AKA]] ''nodular hyperplasia of the prostate''. |
| | *AKA ''benign prostatic hyperplasia'' (abbreviated BPH). |
| | *AKA ''benign prostatic hypertrophy''. |
| | **This is a misnomer. It is ''not'' a hypertrophy. |
| | {{Main|Nodular hyperplasia of the prostate}} |
|
| |
|
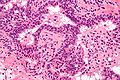
| ==Acute inflammation== | | ==Acute inflammation of the prostate gland== |
| | {{ Infobox external links |
| | | Name = {{PAGENAME}} |
| | | EHVSC = 10176 |
| | | pathprotocols = |
| | | wikipedia = |
| | | pathoutlines = |
| | }} |
| | *[[AKA]] ''prostate gland with acute inflammation''. |
| ===General=== | | ===General=== |
| *A may lead to an increase in the PSA and prompt biopsy. | | *A may lead to an increase in the PSA and prompt biopsy. |
| | |
| | Note: |
| | *"[[Prostatitis]]" is considered a clinical diagnosis. |
| | **Cases are signed out as "acute inflammation". |
| | ***Some pathologists do not comment on the presence (or absence) of inflammation. |
|
| |
|
| ===Microscopic=== | | ===Microscopic=== |
| Features: | | Features: |
| *[[Neutrophil]]s within the glands, between the epithelial cells ''or'' within the stroma - '''key feature'''. | | *[[Neutrophil]]s within the glands, between the epithelial cells ''or'' within the stroma - '''key feature'''. |
| | *+/-Chronic inflammation (lymphocytes) within the surrounding stroma. |
|
| |
|
| Note:
| | DDx: |
| *"Prostatitis" is considered a clinical diagnosis. | | *[[Prostatic infarction]]. |
| **Cases are signed-out as "acute inflammation".
| |
| ***Some pathologists do not comment on the presence (or absence) of inflammation.
| |
|
| |
|
| Image: | | ====Image==== |
| *[http://commons.wikimedia.org/wiki/File:Acute_inflammation_of_prostate.jpg Prostate with acute inflammation (WC)].
| | <gallery> |
| | Image:Acute_inflammation_of_prostate.jpg| Prostate with acute inflammation. (WC/Nephron) |
| | </gallery> |
| | ===Sign out=== |
| | <pre> |
| | G. PROSTATE, LEFT LATERAL SUPERIOR, BIOPSY: |
| | - BENIGN PROSTATE TISSUE; |
| | - FOCAL ACUTE INFLAMMATION. |
| | </pre> |
|
| |
|
| ==Chronic inflammation==
| | <pre> |
| ===Chronic inflammation not otherwise specified===
| | G. PROSTATE, LEFT LATERAL SUPERIOR, BIOPSY: |
| ====Common====
| | - BENIGN PROSTATE TISSUE; |
| *Non-specific.
| | - FOCAL ACUTE AND CHRONIC INFLAMMATION. |
| *Etiology usu. not apparent on histomorphology.
| | </pre> |
|
| |
|
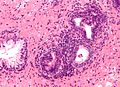
| ====Microscopic==== | | ==Chronic inflammation not otherwise specified== |
| Features:
| | ===General=== |
| *Lymphocytes within the glands, between the epithelial cells ''or'' within the stroma - '''key feature'''.
| |
| | |
| Image:
| |
| *[http://commons.wikimedia.org/wiki/File:Inflammation_of_prostate.jpg Prostate with chronic inflammation (WC)].
| |
| | |
| ===Granulomatous inflammation===
| |
| ====General====
| |
| *Common. | | *Common. |
| *Usu. secondary to BCG treatment of bladder cancer. | | *Non-specific finding. |
| *Several classifications exist<ref name=pmid17092284>{{Cite journal | last1 = Uzoh | first1 = CC. | last2 = Uff | first2 = JS. | last3 = Okeke | first3 = AA. | title = Granulomatous prostatitis. | journal = BJU Int | volume = 99 | issue = 3 | pages = 510-2 | month = Mar | year = 2007 | doi = 10.1111/j.1464-410X.2006.06585.x | PMID = 17092284 | URL = http://onlinelibrary.wiley.com/doi/10.1111/j.1464-410X.2006.06585.x/full }}</ref> - the most commonly used is by ''Epstein & Hutchins''. | | *Etiology usually not apparent on histomorphology. |
|
| |
|
| =====Epstein & Hutchins classification=====
| | ===Microscopic=== |
| The groupings:<ref name=pmid6432674>{{Cite journal | last1 = Epstein | first1 = JI. | last2 = Hutchins | first2 = GM. | title = Granulomatous prostatitis: distinction among allergic, nonspecific, and post-transurethral resection lesions. | journal = Hum Pathol | volume = 15 | issue = 9 | pages = 818-25 | month = Sep | year = 1984 | doi = | PMID = 6432674 }}</ref>
| |
| #Non-specific.
| |
| #*No cause identified, usu. incidentally discovered.
| |
| #*Most common.
| |
| #After TURP.
| |
| #Specific.
| |
| #*Identifiable infectious agent, usu. BCG (in the context of treating bladder cancer), rarely [[tuberculosis]] and even more rarely various [[fungi]] and [[syphilis]].
| |
| #Allergic granulomatous prostatitis.
| |
| #*Usually associated with eosinophils.
| |
| #*Examples:
| |
| #*#[[Wegener granulomatosis]].
| |
| #*#[[Churg-Strauss syndrome]].
| |
| | |
| ====Microscopic====
| |
| Features: | | Features: |
| *[[Granulomas]] in the stroma of the prostate. | | *Lymphocytes within the glands, between the epithelial cells ''or'' within the stroma - '''key feature'''. |
|
| |
|
| Images:
| | Notes: |
| *[http://commons.wikimedia.org/wiki/File:Granulomatous_inflammation_of_bladder_neck.jpg Granulomatous inflammation of the prostate/bladder neck - low mag. (WC)]. | | *Rare scattered lymphocytes are common, especially in the central portion of the gland. |
| *[http://commons.wikimedia.org/wiki/File:Granulomatous_inflammation_of_bladder_neck_high_mag.jpg Granulomatous inflammation of the prostate/bladder neck - high mag. (WC)]. | | *"Focal" one field with a 2.2 mm diameter involved. |
|
| |
|
| ==Atrophy== | | ====Image==== |
| ===General=== | | <gallery> |
| *Small glands (may mimic Gleason score 3 pattern).
| | Image:Inflammation_of_prostate.jpg | Prostate with chronic inflammation. (WC/Nephron) |
| | </gallery> |
| | ===Sign out=== |
| | <pre> |
| | G. PROSTATE, LEFT LATERAL SUPERIOR, BIOPSY: |
| | - BENIGN PROSTATE TISSUE; |
| | - FOCAL CHRONIC INFLAMMATION. |
| | </pre> |
|
| |
|
| ===Microscopic===
| | <pre> |
| Features:
| | F. PROSTATE, RIGHT MEDIAL MIDZONE, BIOPSY: |
| *Glands often have a jagged edges/prows (in cancer the glands tend to have round edges) - '''key feature'''.
| | - BENIGN PROSTATE TISSUE; |
| **Prow = forward most part of a ship's bow that cuts through the water.<ref>[http://en.wikipedia.org/wiki/Prow http://en.wikipedia.org/wiki/Prow]</ref>
| | - CHRONIC INFLAMMATION. |
| ***You may have come across ''prow'' in the context of [[breast cancer]], i.e. ''tubular carcinoma''.
| | </pre> |
| *Gland density is usually lower than in prostate carcinoma, i.e. glands are not back-to-back - '''key feature'''.
| |
| *Atrophic glands are often hyperchromatic.<ref>SN. June 3, 2009.</ref>
| |
| *Scant cytoplasm - usually.
| |
|
| |
|
| Negatives:
| | Note: |
| *Nuclei like normal, i.e. nucleoli uncommon. | | *Opinion is divided on whether this finding should be reported. |
| *Should have two cell layers, i.e. epithelial and myoepithelial (may be difficult to see). | | **Advocates for reporting inflammation say "[i]t is just reporting what you see and may explain the bump in PSA." |
| | **Naysayers opine that "[i]t may provide false assurance that no cancer is present." |
|
| |
|
| ===Atrophy vs. cancer=== | | ==Granulomatous prostatitis== |
| {| class="wikitable" | | {{Main|Granulomatous prostatitis}} |
| | |
| |
| |'''Atrophy'''
| |
| |'''Cancer'''
| |
| |-
| |
| |Glandular architecture/<br>arrangement
| |
| |angulated glands, may <br>look like they originate <br>from one large duct
| |
| |round glands, <br>often back-to-back
| |
| |-
| |
| |Nuclear <br>hyperchromasia
| |
| |marked
| |
| |moderate
| |
| |-
| |
| |Cytoplasm
| |
| |scant/minimal
| |
| |moderate, may <br>be amphophilic
| |
| |-
| |
| |Basal cells
| |
| |may be visible
| |
| |absent
| |
| |-
| |
| |Nucleoli
| |
| |absent
| |
| |present
| |
| |-
| |
| |Secretions in <br>glands
| |
| |no
| |
| |yes - eosinophilic <br>or blue
| |
| |}
| |
|
| |
|
| ==Prostatic infarct== | | ==Prostatic infarct== |
| *[[AKA]] ''prostatic infarction''. | | *[[AKA]] ''prostatic [[infarction]]''. |
| ===General=== | | ===General=== |
| *Rare < 0.1% of core biopsies.<ref name=pmid11023099>{{Cite journal | last1 = Milord | first1 = RA. | last2 = Kahane | first2 = H. | last3 = Epstein | first3 = JI. | title = Infarct of the prostate gland: experience on needle biopsy specimens. | journal = Am J Surg Pathol | volume = 24 | issue = 10 | pages = 1378-84 | month = Oct | year = 2000 | doi = | PMID = 11023099 }}</ref> | | *Rare < 0.1% of core biopsies.<ref name=pmid11023099>{{Cite journal | last1 = Milord | first1 = RA. | last2 = Kahane | first2 = H. | last3 = Epstein | first3 = JI. | title = Infarct of the prostate gland: experience on needle biopsy specimens. | journal = Am J Surg Pathol | volume = 24 | issue = 10 | pages = 1378-84 | month = Oct | year = 2000 | doi = | PMID = 11023099 }}</ref> |
| *Can mimic cancer - [[urothelial carcinoma]].<ref name=pmid11023099/> | | *Can mimic cancer - [[urothelial carcinoma]].<ref name=pmid11023099/> |
| *Prostate usu. large. | | *Prostate usually large. |
|
| |
|
| ===Microscopic=== | | ===Microscopic=== |
| Features: | | Features: |
| *Classic findings of necrosis: | | *Classic findings of [[necrosis]]: |
| **Karyolysis (loss of nuclei), karyorrhexis (frag. of nuclei), pyknosis (small shrunken nuclei). | | **Karyolysis (loss of nuclei), karyorrhexis (frag. of nuclei), pyknosis (small shrunken nuclei). |
| *+/-Squamous metaplasia of prostate gland epithelium. | | *+/-Squamous metaplasia of prostate gland epithelium. |
| Line 232: |
Line 230: |
| *Corpora amylacea - help... call it benign. | | *Corpora amylacea - help... call it benign. |
| *Glands maintain normal spacing. | | *Glands maintain normal spacing. |
| | |
| | DDx: |
| | *[[Urothelial carcinoma]] with squamous differentiation. |
|
| |
|
| Image: | | Image: |
| *[http://www.sciencephoto.com/media/258565/enlarge Prostatic thrombosis (sciencephoto.com)]. | | *[http://www.sciencephoto.com/media/258565/enlarge Prostatic thrombosis (sciencephoto.com)]. |
|
| |
|
| ==Basal cell hyperplasia of the prostate== | | =Preneoplastic changes and atypical changes= |
| *[[AKA]] ''[[basal cell hyperplasia]]''.
| |
| ===General===
| |
| *Atypical appearing glands - typically in transition zone.<ref>URL: [http://pathologyoutlines.com/prostate.html#bch http://pathologyoutlines.com/prostate.html#bch]. Accessed on: 19 June 2010.</ref>
| |
| *May have nucleoli.
| |
| *Benign lesion that can be misdiagnosed as cancer.<ref name=pmid6195916>{{Cite journal | last1 = Cleary | first1 = KR. | last2 = Choi | first2 = HY. | last3 = Ayala | first3 = AG. | title = Basal cell hyperplasia of the prostate. | journal = Am J Clin Pathol | volume = 80 | issue = 6 | pages = 850-4 | month = Dec | year = 1983 | doi = | PMID = 6195916 }}</ref>
| |
| | |
| ===Differentiating between diagnoses===
| |
| Basal cell hyperplasia vs. cancer:<ref>URL: [http://pathologyoutlines.com/prostate.html#bch http://pathologyoutlines.com/prostate.html#bch]. Accessed on: 28 June 2010.</ref>
| |
| *Low power gland architecture near normal.<ref>URL: [http://www.nature.com/modpathol/journal/v16/n6/fig_tab/3880810f1.html http://www.nature.com/modpathol/journal/v16/n6/fig_tab/3880810f1.html]. Accessed on: 28 June 2010.</ref><ref>URL: [http://www.nature.com/modpathol/journal/v16/n6/fig_tab/3880810f2.html http://www.nature.com/modpathol/journal/v16/n6/fig_tab/3880810f2.html]. Accessed on: 28 June 2010.</ref>
| |
| **Glands ''not'' as small as cancer.
| |
| **Folds in gland lumina.
| |
| **No hyperchromasia.
| |
| **Two cell populations (as in normal prostate glands).
| |
| | |
| Image:
| |
| *[http://webpathology.com/image.asp?case=18&n=1 Basal cell hyperplasia of the prostate (webpathology.com)].
| |
| | |
| ==High-grade prostatic intraepithelial neoplasia== | | ==High-grade prostatic intraepithelial neoplasia== |
| *Abbreviated as ''HGPIN''. | | *Abbreviated as ''HGPIN''. |
| *May be referred to as ''prostatic intraepithelial neoplasia'', abbreviated ''PIN''. | | *May be referred to as ''prostatic intraepithelial neoplasia'', abbreviated ''PIN''. |
| ===General===
| | {{Main|High-grade prostatic intraepithelial neoplasia}} |
| *Thought to be a precursor lesion for prostate adenocarcinoma; however, HGPIN does not appear to be associated with increased risk for prostate cancer on re-biopsy at one year (if the initial biopsy had 8 or more cores).<ref name=pmid16406886>{{Cite journal | last1 = Herawi | first1 = M. | last2 = Kahane | first2 = H. | last3 = Cavallo | first3 = C. | last4 = Epstein | first4 = JI. | title = Risk of prostate cancer on first re-biopsy within 1 year following a diagnosis of high grade prostatic intraepithelial neoplasia is related to the number of cores sampled. | journal = J Urol | volume = 175 | issue = 1 | pages = 121-4 | month = Jan | year = 2006 | doi = 10.1016/S0022-5347(05)00064-9 | PMID = 16406886 }}</ref>
| |
| | |
| Low-grade prostatic intraepithelial neoplasia:
| |
| *Not reported and generally believed to be irrelevant biologically/clinically.
| |
| **''PIN'' not otherwise specified refers to ''HGPIN''.
| |
| **Low-grade PIN has the architecture of HGPIN but lacks the nuclear atypia.
| |
| | |
| ===Microscopic===
| |
| Features:
| |
| *Diagnosed on basis of nuclear changes.
| |
| **Hyperchromatic nuclei.
| |
| **Nucleoli present - '''key (high power) feature'''.
| |
| **Often increased N/C ratio.
| |
| **Nuclear enlargement.
| |
| *Different architectures (e.g. micropapillary).
| |
| *Usually epithelial hyperplasia.
| |
| | |
| Note:
| |
| *Nucleoli should be visible with the 20x objective.
| |
| **If one uses the 40x objective... one over calls.
| |
| | |
| ====HGPIN architecture====
| |
| There are several forms:<ref name=Ref_WMSP380>{{Ref WMSP|380}}</ref><ref name=pmid14739906>{{Cite journal | last1 = Bostwick | first1 = DG. | last2 = Qian | first2 = J. | title = High-grade prostatic intraepithelial neoplasia. | journal = Mod Pathol | volume = 17 | issue = 3 | pages = 360-79 | month = Mar | year = 2004 | doi = 10.1038/modpathol.3800053 | PMID = 14739906 | url=http://www.nature.com/modpathol/journal/v17/n3/pdf/3800053a.pdf }}</ref>
| |
| *Flat - uncommon.
| |
| *Tufting - common.
| |
| *Micropapillary - common.
| |
| *Cribriform - rare.
| |
| | |
| Note:
| |
| *The architectural pattern is NOT thought to have any prognostic significance -- may, however, be useful for picking it out from benign prostate.
| |
| | |
| Images:
| |
| *[http://commons.wikimedia.org/wiki/File:High-grade_prostatic_intraepithelial_neoplasia_low_mag.jpg HGPIN - low mag. (WC)].
| |
| *[http://commons.wikimedia.org/wiki/File:High-grade_prostatic_intraepithelial_neoplasia_intermed_mag.jpg HGPIN - intermed. mag. (WC)].
| |
| *[http://commons.wikimedia.org/wiki/File:High-grade_prostatic_intraepithelial_neoplasia_high_mag.jpg HGPIN - high mag. (WC)].
| |
| | |
| ===Differentiating between diagnoses===
| |
| HGPIN vs. adenocarcinoma:
| |
| *Glands with HGPIN have two or more distinct cells layers.
| |
| | |
| HGPIN vs. normal:
| |
| *HPGIN has nuclear changes.
| |
| | |
| May need IHC (especially for cancer vs. HGPIN).
| |
| | |
| IHC patterns:
| |
| *Cancer: AMACR +ve, p63 -ve, HMWCK -ve.
| |
| *HGPIN: AMACR +ve, p63 +ve, HMWCK +ve.
| |
| *Normal: AMACR -ve, p63 +ve, HMWCK ve+.
| |
|
| |
|
| ==Atypical small acinar proliferation== | | ==Atypical small acinar proliferation== |
| *Abbreviated ''ASAP''. | | *Abbreviated ''ASAP''. |
| ===General===
| | *[[AKA]] ''suspicious for carcinoma''.<ref>THvdK. 19 June 2010.</ref> |
| *It is a [[waffle diagnosis]], i.e. it is not considered an entity with a distinct pathobiology.<ref name=pmid17378841>{{cite journal |author=Flury SC, Galgano MT, Mills SE, Smolkin ME, Theodorescu D |title=Atypical small acinar proliferation: biopsy artefact or distinct pathological entity |journal=BJU International |volume=99 |issue=4 |pages=780-5 |year=2007 |month=January |pmid= 17378841 |doi= |url=http://www3.interscience.wiley.com/journal/118508438/abstract}}</ref> | | **''ASAP'' is preferred as it does not contain the word ''carcinoma'' and, thus, cannot be misread as ''carcinoma'', i.e. positive for malignancy. |
| **It is the same as ''suspicious for carcinoma''.<ref>THvdK. 19 June 2010.</ref>
| | {{Main|Atypical small acinar proliferation}} |
| ***''ASAP'' is preferred as it does not contain the word ''carcinoma'' and, thus, cannot be misread as ''carcinoma'', i.e. positive for malignancy.
| |
| **Analogous to ''ASCUS'' on a pap test.
| |
| **ASAP should be used sparingly.
| |
| ***One benchmark is < 3-5% of biopsies.<ref>THvdK. 19 June 2010.</ref>
| |
| *Never diagnosed on excision, i.e. prostatectomy specimen.
| |
| | |
| ===Histologic characteristics===
| |
| *Atypical appearing acini.
| |
| *Limited extent, e.g. 2-3 glands.
| |
| *IHC not contributory.
| |
| *Deeper cuts didn't yield anything.
| |
| | |
| ===Association with adenocarcinoma===
| |
| *On subsequent [[biopsy]] - chance of finding [[adenocarcinoma]] is approximately 40%; this is higher than if there is [[high-grade prostatic intraepithelial neoplasia]] (HGPIN).<ref>{{cite journal |author=Leite KR, Camara-Lopes LH, Cury J, Dall'oglio MF, Sañudo A, Srougi M |title=Prostate cancer detection at rebiopsy after an initial benign diagnosis: results using sextant extended prostate biopsy |journal=Clinics |volume=63 |issue=3 |pages=339–42 |year=2008 |month=June |pmid=18568243 |doi= |url=http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1807-59322008000300009&lng=en&nrm=iso&tlng=en}}</ref>
| |
| | |
| ===Management===
| |
| *ASAP is considered an [[indication]] for re-biopsy;<ref>{{cite journal |author=Bostwick DG, Meiers I |title=Atypical small acinar proliferation in the prostate: clinical significance in 2006 |journal=Arch. Pathol. Lab. Med. |volume=130 |issue=7 |pages=952–7 |year=2006 |month=July |pmid=16831049 |doi= |url=http://journals.allenpress.com/jrnlserv/?request=get-abstract&issn=0003-9985&volume=130&page=952}}</ref> in one survey of [[urologist]]s<ref>{{cite journal |author=Rubin MA, Bismar TA, Curtis S, Montie JE |title=Prostate needle biopsy reporting: how are the surgical members of the Society of Urologic Oncology using pathology reports to guide treatment of prostate cancer patients? |journal=Am. J. Surg. Pathol. |volume=28 |issue=7 |pages=946–52 |year=2004 |month=July |pmid=15223967 |doi= |url=}}</ref> 41/42 (~98%) of respondents considered it a sufficient reason to re-biopsy.
| |
| | |
| ==Intraductal carcinoma==
| |
| ===General===
| |
| *Associated with a poor prognosis.<ref name=pmid19246509>{{Cite journal | last1 = Henry | first1 = PC. | last2 = Evans | first2 = AJ. | title = Intraductal carcinoma of the prostate: a distinct histopathological entity with important prognostic implications. | journal = J Clin Pathol | volume = 62 | issue = 7 | pages = 579-83 | month = Jul | year = 2009 | doi = 10.1136/jcp.2009.065003 | PMID = 19246509 }}</ref>
| |
| | |
| ===Microscopic===
| |
| Features:
| |
| *Malignant cells in glands with basal cells - '''key feature'''.
| |
| **Two cell populations:
| |
| **#Obviously malignant cells with enlarged nuclei, granular chromatin, hyperchromasia and nucleoli.
| |
| **#Cells with pale cytoplasm and smaller nuclei.
| |
| | |
| ==Prostatic adenocarcinoma==
| |
| *[[AKA]] ''adenocarcinoma of the prostate''.
| |
| | |
| ===Criteria as a list===
| |
| Major criteria (the ABCs of prostate pathology):<ref name=pmid17213347>{{cite journal |author=Humphrey PA |title=Diagnosis of adenocarcinoma in prostate needle biopsy tissue |journal=J. Clin. Pathol. |volume=60 |issue=1 |pages=35–42 |year=2007 |month=January |pmid=17213347 |pmc=1860598 |doi=10.1136/jcp.2005.036442 |url=http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1860598/?tool=pubmed}}</ref>
| |
| #Architecture.
| |
| #*Increased gland density.
| |
| #*Small circular glands.
| |
| #**In rare subtypes - large branching glands.
| |
| #*"Infiltrative growth" pattern - malignant glands between benign ones.
| |
| #**Image: [http://www.nature.com/modpathol/journal/v17/n3/fig_tab/3800050f1.html#figure-title Infiltrative growth pattern (nature.com)].
| |
| #Basal cells lacking.
| |
| #Cytological abnormalities:
| |
| #*Nuclear enlargement.
| |
| #*Nucleoli.
| |
| | |
| Minor criteria:<ref name=pmid17213347/>
| |
| #Nuclear hyperchromasia.
| |
| #Wispy blue mucin.
| |
| #*Image: [http://www.nature.com/modpathol/journal/v17/n3/fig_tab/3800050f3.html#figure-title Wispy blue mucin (nature.com)] - from Epstein.<ref name=pmid14739905>{{cite journal |author=Epstein JI |title=Diagnosis and reporting of limited adenocarcinoma of the prostate on needle biopsy |journal=Mod. Pathol. |volume=17 |issue=3 |pages=307–15 |year=2004 |month=March |pmid=14739905 |doi=10.1038/modpathol.3800050 |url=http://www.nature.com/modpathol/journal/v17/n3/full/3800050a.html}}</ref>
| |
| #Pink amorphous secretions.
| |
| #*Image: [http://www.nature.com/modpathol/journal/v17/n3/fig_tab/3800050f11.html Pink amorphous secretions (nature.com)] - from Epstein.<ref name=pmid14739905>{{cite journal |author=Epstein JI |title=Diagnosis and reporting of limited adenocarcinoma of the prostate on needle biopsy |journal=Mod. Pathol. |volume=17 |issue=3 |pages=307–15 |year=2004 |month=March |pmid=14739905 |doi=10.1038/modpathol.3800050 |url=http://www.nature.com/modpathol/journal/v17/n3/full/3800050a.html}}</ref>
| |
| #Intraluminal crystalloid.
| |
| #*Image: [http://www.nature.com/modpathol/journal/v17/n3/fig_tab/3800050f4.html#figure-title Intraluminal crystalloid (nature.com)] - from Epstein.<ref name=pmid14739905/>
| |
| #Amphophilic cytoplasm.
| |
| #*Amphopilic is said to be ''bluish-red''<ref>URL: [http://pancreaticcancer2000.com/page1.htm http://pancreaticcancer2000.com/page1.htm]. Accessed on: 3 June 2010.</ref> -- though might also be described as ''blue-grey''.
| |
| #**Image: [http://www.webpathology.com/image.asp?n=4&Case=20 Amphophilic cytoplasm is prostate carcinoma].
| |
| #Adjacent HGPIN.
| |
| #Mitoses - quite rare.
| |
| | |
| Extent/quantity criteria:
| |
| *There is no agreed upon minimum number of glands; however, one paper suggests that agreement among experts is low with 5 or less glands.<ref name=pmid20061936>{{Cite journal | last1 = Van der Kwast | first1 = TH. | last2 = Evans | first2 = A. | last3 = Lockwood | first3 = G. | last4 = Tkachuk | first4 = D. | last5 = Bostwick | first5 = DG. | last6 = Epstein | first6 = JI. | last7 = Humphrey | first7 = PA. | last8 = Montironi | first8 = R. | last9 = Van Leenders | first9 = GJ. | title = Variability in diagnostic opinion among pathologists for single small atypical foci in prostate biopsies. | journal = Am J Surg Pathol | volume = 34 | issue = 2 | pages = 169-77 | month = Feb | year = 2010 | doi = 10.1097/PAS.0b013e3181c7997b | PMID = 20061936 }}</ref>
| |
| **Thus, it has been suggested that six or more glands should be present to diagnose cancer.<ref name=pmid20061936/>
| |
| | |
| ===Low power features===
| |
| *Architecture is the '''key''' to diagnosing low grade cancer.
| |
| **Back-to-back glands or crowding of glands -- think low grade cancer (Gleason pattern 3).
| |
| **Sharp transition between gland border and lumen.
| |
| ***Loss of epithelial folding at the epithelium-gland lumen interface - "punched-out" appearance.
| |
| **Eosinophilic debris within the gland lumen (pink amorphous secretions, intraluminal crystalloid).
| |
| **Blue-tinged acellular material within the gland lumen (mucin) -- uncommon.
| |
| **"Infiltrative": small round/oval (malignant) glands (approx. 5 cells across) interspersed with larger (benign) glands that are 2-3 times larger.
| |
| | |
| ===High power features===
| |
| *Nuclei.
| |
| **Hyperchromatic nuclei (like in HGPIN).
| |
| **Nuclear enlargement.
| |
| ***Difficult to appreciate (if cancer isn't side-by-side with normal prostate).
| |
| ***Difficult to see if not on high power.
| |
| *Nucleoli visible on high power (200x or 100X)
| |
| **May be difficult to see - especially if light intensity is low.
| |
| ***One should not use 400x to look for nucleoli (it is a waste of time + you risk overcalling something benign).
| |
| **If I see three good nucleoli in a gland I'm usually confident it is cancer.
| |
| *Loss of basal cells - diagnostic feature.
| |
| **Like in breast pathology (where one looks for loss of myoepithelial cells) - this may be difficult to see.
| |
| | |
| Notes:
| |
| *Mitoses are not a common feature - don't waste time looking for them.
| |
| | |
| ===IHC===
| |
| *AMACR +ve.
| |
| *AR +ve -- in prostate confined cancer.
| |
| **Usu. -ve in LN +ve disease.<ref name=pmid20878946>{{Cite journal | last1 = Fleischmann | first1 = A. | last2 = Rocha | first2 = C. | last3 = Schobinger | first3 = S. | last4 = Seiler | first4 = R. | last5 = Wiese | first5 = B. | last6 = Thalmann | first6 = GN. | title = Androgen receptors are differentially expressed in Gleason patterns of prostate cancer and down-regulated in matched lymph node metastases. | journal = Prostate | volume = 71 | issue = 5 | pages = 453-60 | month = Apr | year = 2011 | doi = 10.1002/pros.21259 | PMID = 20878946 }}</ref> *PSA +ve.
| |
| *PSAP +ve.
| |
| **May be positive in hindgut [[neuroendocrine tumour]]s.<ref name=pmid>{{Cite journal | last1 = Azumi | first1 = N. | last2 = Traweek | first2 = ST. | last3 = Battifora | first3 = H. | title = Prostatic acid phosphatase in carcinoid tumors. Immunohistochemical and immunoblot studies. | journal = Am J Surg Pathol | volume = 15 | issue = 8 | pages = 785-90 | month = Aug | year = 1991 | doi = | PMID = 1712549 }}</ref>
| |
| *p63 -ve.
| |
| *HMWCK (34betaE12) -ve.
| |
| | |
| Combination immunostains:
| |
| *''PIN-4'' -- consists of: CK5 + CK14 + p63 + P504S (AMACR).<ref>URL: [http://biocare.net/wp-content/uploads/225DS.pdf http://biocare.net/wp-content/uploads/225DS.pdf]. Accessed on: 18 October 2011.</ref><ref>URL: [http://www.antibodies-online.com/antibody/308235/anti-PIN-4+p63+Cytokeratin+HMW+p504S++AMACR/ http://www.antibodies-online.com/antibody/308235/anti-PIN-4+p63+Cytokeratin+HMW+p504S++AMACR/]. Accessed on: 18 October 2011.</ref><ref>URL: [http://www.webpathology.com/image.asp?case=96&n=5 http://www.webpathology.com/image.asp?case=96&n=5]. Accessed on: 18 October 2011.</ref>
| |
| **[[AKA]] ''PIN''.
| |
| **[[AKA]] ''CAP''.
| |
| ***Why '''CAP'''?
| |
| ****A. '''CA'''ncer of the '''P'''rostate.
| |
| | |
| ===Mimics===
| |
| Mimics of prostate adenocarcinoma:<ref>{{Ref TPoSP|100-3}}</ref>
| |
| {| class="wikitable"
| |
| | '''Entity'''
| |
| | '''Key feature'''
| |
| | '''Detailed microscopic'''
| |
| | '''Other'''
| |
| | '''Image'''
| |
| |-
| |
| | Adenosis ([[AKA]] ''atypical adenomatous hyperplasia'')
| |
| | gradual transition between normal & small gland (NOT two populations)
| |
| | many small glands, lack nuclear size variation, basal layer present
| |
| | nucleoli may be present; may need to do p63 or 34betaE12 to find basal layer
| |
| | '''Image'''
| |
| |-
| |
| | Sclerosing adenosis
| |
| | gradual transition between normal & small gland (NOT two populations), fibrosis
| |
| | many small glands, lack nuclear size variation, basal layer present
| |
| | analogous to sclerosing adenosis of breast (???)
| |
| | '''Image'''
| |
| |-
| |
| | Atrophy
| |
| | sharp angulation of gland
| |
| | nuclear hyperchromasia, scant cytoplasm
| |
| | may appear right beside non-atrophic tissue
| |
| | '''Image'''
| |
| |-
| |
| | Basal cell hyperplasia
| |
| | two distinct cell populations (in epithelial component)
| |
| | abundant epithelial cells; nucleoli in pale ('blue') nuclei of basal cells, glandular cell nuclei darker ('purple')
| |
| | vaguely similar to epithelial hyperplasia of usual type (EHUT) in breast
| |
| | '''Image'''
| |
| |-
| |
| | Bulbourethral gland
| |
| | no nuclear atypia
| |
| | clear cytoplasm
| |
| | apex of prostate
| |
| | '''Image'''
| |
| |-
| |
| | Seminal vesicles
| |
| | lipofuscin (yellow granular material in cytoplasm), smudge cells (smeared appearance + hyperchromatic)
| |
| | fern-like arrangement of epithelium (low power), nucleoli, surrounded by muscle, +/- nuclear inclusions
| |
| | involvement by cancer changes staging, lipofuscin may be present in prostate, often has marked nuc. size var.
| |
| | [http://commons.wikimedia.org/wiki/File:Seminal_vesicle_high_mag.jpg SV - high mag. (WC)], [http://commons.wikimedia.org/wiki/File:Seminal_vesicle_low_mag.jpg SV - low mag. (WC)]
| |
| |-
| |
| | Radiation effect
| |
| | marked nuclear size variation
| |
| | increased stroma (fibrosis), lack nucleoli ???
| |
| | history of Rx; uniform nuc. size with Hx of Rx should raise susp. of cancer
| |
| | '''Image'''
| |
| |-
| |
| | Prostatitis
| |
| | inflammatory cells (lymphocytes, plasma cells, PMNs)
| |
| | no nuclear atypia, normal gland arch.
| |
| | clinical mimic of cancer (elevated PSA); usu. not a problem for the pathologist
| |
| | [http://commons.wikimedia.org/wiki/File:Inflammation_of_prostate.jpg (WC)]
| |
| |-
| |
| | [[Vasitis nodosa]]
| |
| | sperm within ducts, clinical history (usu. post-vasectomy)
| |
| | small tubules, nucleoli common, mild atypia, may "invade" vessels, track along nerves
| |
| | mimics metastatic prostate carcinoma, IHC stains: PSA-, PSAP-
| |
| | [http://www.webpathology.com/image.asp?n=11&Case=40 VN (webpathology.com)]
| |
| |}
| |
| Memory device: '''AAABBRS''' = atrophy, adenosis, adenosis (sclerosing), basal cell hyperplasia, bulbourethral gland, radiation, seminal vesicles.
| |
| | |
| ===Grading===
| |
| There is only one grading system that any one talks about...
| |
| | |
| ====Gleason grading system====
| |
| *Score range: 2-10.
| |
| *Reported as on biopsy as: (primary pattern) + (secondary pattern ''or'' tertiary pattern with the highest grade) = sum.
| |
| **e.g. ''Gleason grade 3+4=7'' means: pattern 3 is present and dominant, pattern 4 is the remainder of the tumour - but present in a lesser amount than pattern 3.
| |
| *Reported as on prostatectomies as: (primary pattern) + (secondary pattern) = sum, (tertiary pattern)
| |
| | |
| *Tertiary Gleason pattern - definition: a pattern that is seen in than 5% of the tumour (volume), that is higher grade than the two dominant patterns.<ref name=Ref_GUP72>{{Ref GUP|72}}</ref>
| |
| **The presence of a tertiary patterns adversely affect the prognosis; however, the prognosis is not as bad as when the tertiary pattern is the secondary pattern, i.e. 3+4 tertiary 5 has a better prognosis than 3+5 (with some small amount of pattern 4).<ref name=Ref_GUP72>{{Ref GUP|72}}</ref>
| |
| | |
| Examples:
| |
| *A biopsy has 80% pattern 4, 15.1% pattern 3 and 4.9% pattern 5... it would be reported as: 4+5=9.
| |
| *A prostatectomy has 80% pattern 4, 15.1% pattern 3 and 4.9% pattern 5... it would be reported as: 4+3=7 with tertiary pattern 5.
| |
| | |
| Testing yourself:
| |
| *There is a nice test-yourself quiz from Johns Hopkins: [http://162.129.103.34/prostate/ http://162.129.103.34/prostate/].
| |
| **It was studied in a paper by Kronz et al..<ref name=pmid11014569>{{Cite journal | last1 = Kronz | first1 = JD. | last2 = Silberman | first2 = MA. | last3 = Allsbrook | first3 = WC. | last4 = Bastacky | first4 = SI. | last5 = Burks | first5 = RT. | last6 = Cina | first6 = SJ. | last7 = Mills | first7 = SE. | last8 = Ross | first8 = JS. | last9 = Sakr | first9 = WA. | last10 = Tomaszewski | first10 = JE. | last11 = True | first11 = LD. | last12 = Ulbright | first12 = TM. | last13 = Weinstein | first13 = MW. | last14 = Yantiss | first14 = RK. | last15 = Young | first15 = RH. | last16 = Epstein | first16 = JI. | title = Pathology residents' use of a Web-based tutorial to improve Gleason grading of prostate carcinoma on needle biopsies. | journal = Hum Pathol | volume = 31 | issue = 9 | pages = 1044-50 | month = Sep | year = 2000 | doi = 10.1053/hupa.2000.16278 | PMID = 11014569 }}</ref>
| |
| | |
| ====Gleason pattern 1 & 2====
| |
| *Academic thing - you can forget about 'em.
| |
| | |
| ====Gleason pattern 3====
| |
| *Glands smaller than normal prostate glands + loss of epithelial folding.
| |
| *Can draw a line around each gland.
| |
| | |
| Notes:
| |
| *All ''cribriform'' is now classified as Gleason pattern 4.<ref name=pmid20006878>{{cite journal |author=Epstein JI |title=An update of the Gleason grading system |journal=J. Urol. |volume=183 |issue=2 |pages=433–40 |year=2010 |month=February |pmid=20006878 |doi=10.1016/j.juro.2009.10.046 |url=}}</ref>
| |
| | |
| ====Gleason pattern 4====
| |
| *Loss of gland lumina.
| |
| *Gland fusion.
| |
| *Benign looking cords ('hypernephroid pattern').
| |
| *Cribriform.
| |
| *Glomeruloid pattern - resembles a glomerulus.
| |
| | |
| Notes:
| |
| *One gland is not enough to call Gleason 4.
| |
| | |
| Images:
| |
| *[http://commons.wikimedia.org/wiki/File:Prostate_cancer_with_Gleason_pattern_4_low_mag.jpg Gleason pattern 4 - cribriform (WC)].
| |
| *[http://commons.wikimedia.org/wiki/File:Gleason_4_and_5_intermed_mag.jpg Gleason pattern 4 - small glands & Gleason pattern 5 - single cells (WC)].
| |
| *[http://www.nature.com/modpathol/journal/v17/n3/fig_tab/3800050f9.html#figure-title Glomeruloid pattern (nature.com)].
| |
| | |
| ====Gleason pattern 5====
| |
| *Sheets.
| |
| **Must be differentiated from intraductal growth (which like in the breast are well circumscribed nests).
| |
| *Single cells.
| |
| **May be confused with stromal/lymphocytic infiltration.
| |
| ***Look for nucleoli, cells should be round (prostatic stroma cells are spindle cells).
| |
| *Cords.
| |
| *Nests of cells with [[necrosis]] at centre.
| |
| | |
| Image: [http://commons.wikimedia.org/wiki/File:Gleason_4_and_5_intermed_mag.jpg Gleason pattern 4 - small glands & Gleason pattern 5 - single cells (WC)].
| |
| | |
| ====Special types====
| |
| Special types of prostate cancer have set Gleason scores:<ref name=pmid14976541>{{cite journal |author=Grignon DJ |title=Unusual subtypes of prostate cancer |journal=Mod. Pathol. |volume=17 |issue=3 |pages=316–27 |year=2004 |month=March |pmid=14976541 |doi=10.1038/modpathol.3800052 |url=}}</ref>
| |
| {| class="wikitable sortable" style="margin-left:auto;margin-right:auto"
| |
| | Special type
| |
| | Gleason pattern
| |
| | Comment
| |
| |-
| |
| |Ductal carcinoma
| |
| | 4
| |
| | may be graded 3 or 5<ref name=bostwicklabs>URL: [https://www.bostwicklaboratories.com/global/physicians/medical-library/articles/gleason-grading.aspx https://www.bostwicklaboratories.com/global/physicians/medical-library/articles/gleason-grading.aspx]. Accessed on: 26 November 2011.</ref>
| |
| |-
| |
| |Mucinous carcinoma
| |
| | 4
| |
| |
| |
| |-
| |
| |Sarcomatoid carcinoma
| |
| | 5
| |
| | glands graded separately
| |
| |-
| |
| |Signet ring cell carcinoma
| |
| | 5
| |
| |
| |
| |-
| |
| |Small cell carcinoma
| |
| | not graded
| |
| | may be graded 5<ref name=bostwicklabs/>
| |
| |-
| |
| |Adenosquamous and squamous carcinoma
| |
| | not graded
| |
| |
| |
| |-
| |
| |Lymphoepithelioma-like carcinoma
| |
| | not graded
| |
| |
| |
| |-
| |
| |Adenoid cystic carcinoma
| |
| | not graded
| |
| |
| |
| |-
| |
| |Urothelial carcinoma
| |
| | not graded
| |
| |
| |
| |-
| |
| |Undifferentiated carcinoma, NOS
| |
| | not graded
| |
| |
| |
| |}
| |
| | |
| How to remember the ones that aren't graded - think of '''Ur''' '''L'''ung carcinomas ('''Ur'''othelial carcinoma, '''L'''ymphoepithelioma-like carcinoma):
| |
| *Small cell carcinoma.
| |
| *Squamous cell carcinoma.
| |
| *Adenosquamous carcinoma.
| |
| *Adenoid cystic carcinoma.
| |
| | |
| ===Management===
| |
| The management changes between Gleason 6, 7 & 8; typically, the implications are:
| |
| * Gleason 6: watchful waiting or radioactive seeds, surgery if patient wants.
| |
| * Gleason 7: do something.
| |
| * Gleason 8+: bad cancer - do something quickly!
| |
| | |
| Bottom line: You want to be sure when you call something Gleason pattern 4.
| |
| | |
| Note:
| |
| *The usual caveats apply to the above; if the patient is moribund-- nothing is done, if the patient refuses treatment... nothing is done et cetera.
| |
| ===Margins + Extension===
| |
| {{Main|Surgical margins}}
| |
| Definitions:
| |
| *Extraprostatic extension (EPE) is difficult to assess (in prostatectomy specimens) as there is no consensus definition.
| |
| **The prostate does NOT have a well defined capsule.
| |
| ***Intraobserver agreement for EPE is fair-moderate and lower than for the surgical margin.<ref name=pmid18708939>{{Cite journal | last1 = Evans | first1 = AJ. | last2 = Henry | first2 = PC. | last3 = Van der Kwast | first3 = TH. | last4 = Tkachuk | first4 = DC. | last5 = Watson | first5 = K. | last6 = Lockwood | first6 = GA. | last7 = Fleshner | first7 = NE. | last8 = Cheung | first8 = C. | last9 = Belanger | first9 = EC. | last10 = Amin | first10 = MB. | last11 = Boccon-Gibod | first11 = L. | last12 = Bostwick | first12 = DG. | last13 = Egevad | first13 = L. | last14 = Epstein | first14 = JI. | last15 = Grignon | first15 = DJ. | last16 = Jones | first16 = EC. | last17 = Montironi | first17 = R. | last18 = Moussa | first18 = M. | last19 = Sweet | first19 = JM. | last20 = Trpkov | first20 = K. | last21 = Wheeler | first21 = TM. | last22 = Srigley | first22 = JR. | title = Interobserver variability between expert urologic pathologists for extraprostatic extension and surgical margin status in radical prostatectomy specimens. | journal = Am J Surg Pathol | volume = 32 | issue = 10 | pages = 1503-12 | month = Oct | year = 2008 | doi = 10.1097/PAS.0b013e31817fb3a0 | PMID = 18708939 }}</ref>
| |
| *Surgical margin - where the surgeon cut.
| |
| **It is possible to have EPE without a positive margin.
| |
| **It is possible to have a positive margin without EPE.
| |
| | |
| Important:
| |
| *EPE cannot be called on a biopsy unless the tumour is next to adipose tissue.<ref>AE. 4 June 2010.</ref>
| |
| | |
| ====Extraprostatic extension (EPE)====
| |
| *Prostatectomy specimens: EPE is present if there is either:
| |
| *#A "significant bulge" in the contour of the prostate at low power ''and'' no fibromuscular tissue surrounding the malignant cells.
| |
| *#Malignant cells directly adjacent to peri-prostatic adipose tissue.
| |
| *Prostate biopsy: EPE is present if tumour touches adipose tissue.<ref name=pmid17707261>{{Cite journal | last1 = Epstein | first1 = JI. | last2 = Srigley | first2 = J. | last3 = Grignon | first3 = D. | last4 = Humphrey | first4 = P. | title = Recommendations for the reporting of prostate carcinoma. | journal = Hum Pathol | volume = 38 | issue = 9 | pages = 1305-9 | month = Sep | year = 2007 | doi = 10.1016/j.humpath.2007.05.015 | PMID = 17707261 }}
| |
| </ref>
| |
| **The prostate, at the apex, may have some skeletal muscle. Thus, it is difficult to define extention... ergo EPE not called at the apex.
| |
| | |
| ===Reporting prostate cancer===
| |
| ====Elements of a prostate biopsy report with cancer====
| |
| Important elements:<ref name=pmid17213347/>
| |
| #Type of cancer, e.g. "prostatic adenocarcinoma, acinar type".
| |
| #Gleason score including primary and secondary pattern, e.g. "Gleason score 3+4=7".
| |
| #Number of cores and number involved, e.g. "2/3 cores involved by cancer".
| |
| #Percent area involved, i.e. how much of the core is cancer, e.g. "75% of specimen is tumour".
| |
| #Percent area involved that is Gleason pattern 4 or 5, e.g. "25% of the tumour is Gleason pattern 4 or 5".
| |
| #Presence of perineural invasion.
| |
| #Presence of extension into fat (extraprostatic extension).
| |
| | |
| Notes:
| |
| *"Percent area involved" may seem like an odd thing to request 'cause it is sampling dependent, i.e. if the radiologist sticks the biopsy needle deeper into the lesion more of the core is positive, but urologists think it is important -- more important than perineural invasion.<ref>{{cite journal |author=Rubin MA, Bismar TA, Curtis S, Montie JE |title=Prostate needle biopsy reporting: how are the surgical members of the Society of Urologic Oncology using pathology reports to guide treatment of prostate cancer patients? |journal=Am. J. Surg. Pathol. |volume=28 |issue=7 |pages=946–52 |year=2004 |month=July |pmid=15223967 |doi= |url=}}</ref>
| |
| | |
| ====Prostatectomy specimens====
| |
| See: [http://www.cap.org/apps/cap.portal?_nfpb=true&cntvwrPtlt_actionOverride=/portlets/contentViewer/show&_windowLabel=cntvwrPtlt&cntvwrPtlt{actionForm.contentReference}=committees/cancer/cancer_protocols/protocols_index.html&_pageLabel=cntvwr CAP checklist].
| |
| | |
| ===Molecular changes in prostate cancer===
| |
| A fusion gene between ''TMPRSS2'' and ''ERG'' is described.<ref name=pmid20478527>{{cite journal | author = Yu J, Yu J, Mani RS, Cao Q, Brenner CJ, Cao X, Wang X, Wu L, Li J, Hu M, Gong Y, Cheng H, Laxman B, Vellaichamy A, Shankar S, Li Y, Dhanasekaran SM, Morey R, Barrette T, Lonigro RJ, Tomlins SA, Varambally S, Qin ZS, Chinnaiyan AM | title = An Integrated Network of Androgen Receptor, Polycomb, and TMPRSS2-ERG Gene Fusions in Prostate Cancer Progression | journal = Cancer Cell | volume = 17 | issue = 5 | pages = 443–54 | year = 2010 | month = May | pmid = 20478527 | pmc = 2874722 | doi = 10.1016/j.ccr.2010.03.018 | url = }}</ref><ref name=omim602060>{{OMIM|602060}}</ref>
| |
| *Both genes are on chromosome 21.
| |
| *Currently ''not'' used diagnostically.
| |
| *Fusion gene seen in approx. 50% of prostate cancer.<ref name=omim602060>{{OMIM|602060}}</ref>
| |
| *A subset of ''TMPRSS2-ERG'' known as ''2+Edel'' (seen in ~7% of all prostate cancer cases) predicts poor survival.<ref name=pmid17637754>{{Cite journal | last1 = Attard | first1 = G. | last2 = Clark | first2 = J. | last3 = Ambroisine | first3 = L. | last4 = Fisher | first4 = G. | last5 = Kovacs | first5 = G. | last6 = Flohr | first6 = P. | last7 = Berney | first7 = D. | last8 = Foster | first8 = CS. | last9 = Fletcher | first9 = A. | title = Duplication of the fusion of TMPRSS2 to ERG sequences identifies fatal human prostate cancer. | journal = Oncogene | volume = 27 | issue = 3 | pages = 253-63 | month = Jan | year = 2008 | doi = 10.1038/sj.onc.1210640 | PMID = 17637754 }}</ref>
| |
| | |
| =Unusual forms of prostate cancer=
| |
| ==Prostatic ductal adenocarcinoma==
| |
| *[[AKA]] ''ductal adenocarcinoma of the prostate''.
| |
| *[[AKA]] ''prostatic adenocarinoma, large duct type''.
| |
| ===General===
| |
| *Sometimes it is referred to as ''endometrioid'' or ''endometrial'' adenocarcinoma; both terms are discouraged.<ref name=pmid18773743>{{Cite journal | last1 = Samaratunga | first1 = H. | last2 = Delahunt | first2 = B. | title = Ductal adenocarcinoma of the prostate: current opinion and controversies. | journal = Anal Quant Cytol Histol | volume = 30 | issue = 4 | pages = 237-46 | month = Aug | year = 2008 | doi = | PMID = 18773743 }}</ref>
| |
| *Controversial - may represent ''acinar adenocarcinoma'' with periurethral ducts involvement.<ref name=pmid10403300>{{Cite journal | last1 = Bock | first1 = BJ. | last2 = Bostwick | first2 = DG. | title = Does prostatic ductal adenocarcinoma exist? | journal = Am J Surg Pathol | volume = 23 | issue = 7 | pages = 781-5 | month = Jul | year = 1999 | doi = | PMID = 10403300 }}</ref>
| |
| | |
| ===Microscopic===
| |
| Features:<ref name=Ref_GUP88>{{Ref GUP|88}}</ref>
| |
| *Pseudostratified (crowded appearing) columnar (or cigar-shaped) nuclei - '''key feature'''.
| |
| **Vaguely resembles colonic adenocarcinoma.
| |
| *Variable architecture:
| |
| **Papillary.
| |
| **Cribriform.
| |
| **Single gland (large glands).
| |
| **Endometrioid - vaguely looks like endometrial carcinoma (with back-to-back glands).
| |
| | |
| Notes:
| |
| *Usually seen in association with conventional (acinar) prostate adenocarcinoma.
| |
| | |
| Images:
| |
| *[http://path.upmc.edu/cases/case203.html Prostatic ductal adenocarcinoma - several images (upmc.edu)].
| |
| *[http://path.upmc.edu/cases/case711.html Prostatei ductal adenocarcinoma - another case - several images (upmc.edu)].
| |
| | |
| ==PIN-like prostatic ductal adenocarcinoma==
| |
| ===General===
| |
| *Recently described.<ref name=pmid16607376>{{Cite journal | last1 = Hameed | first1 = O. | last2 = Humphrey | first2 = PA. | title = Stratified epithelium in prostatic adenocarcinoma: a mimic of high-grade prostatic intraepithelial neoplasia. | journal = Mod Pathol | volume = 19 | issue = 7 | pages = 899-906 | month = Jul | year = 2006 | doi = 10.1038/modpathol.3800601 | PMID = 16607376 }}</ref><ref name=pmid20438402>{{Cite journal | last1 = Lee | first1 = TK. | last2 = Miller | first2 = JS. | last3 = Epstein | first3 = JI. | title = Rare histological patterns of prostatic ductal adenocarcinoma. | journal = Pathology | volume = 42 | issue = 4 | pages = 319-24 | month = Jun | year = 2010 | doi = 10.3109/00313021003767314 | PMID = 20438402 }}</ref>
| |
| *May be confused with [[prostatic intraepithelial neoplasia]] (PIN).
| |
| | |
| ===Microscopic===
| |
| Features:<ref name=pmid16607376>{{Cite journal | last1 = Hameed | first1 = O. | last2 = Humphrey | first2 = PA. | title = Stratified epithelium in prostatic adenocarcinoma: a mimic of high-grade prostatic intraepithelial neoplasia. | journal = Mod Pathol | volume = 19 | issue = 7 | pages = 899-906 | month = Jul | year = 2006 | doi = 10.1038/modpathol.3800601 | PMID = 16607376 }}</ref>
| |
| *Stratified malignant epithelium.
| |
| | |
| Note:
| |
| *Vaguely similar to a tubular adenoma of the colon.
| |
| | |
| Image:
| |
| *[http://www.nature.com/modpathol/journal/v19/n7/fig_tab/3800601f1.html#figure-title PIN-like adenocarcinoma (nature.com)].
| |
| | |
| ==Foamy gland carcinoma==
| |
| | |
| ===Microscopic===
| |
| Features:
| |
| *Tufted glandular border.
| |
| *Abundant eosinophilic (or hyperchromatic) cytoplasm - '''key feature'''.
| |
| *Gland size larger than "typical" prostate cancer.
| |
| | |
| Image: [http://www.nature.com/modpathol/journal/v17/n3/fig_tab/3800050f11.html#figure-title Foamy gland carcinoma (nature.com)].
| |
| | |
| ==Atrophic carcinoma==
| |
| ===Microscopic===
| |
| Features:
| |
| *Scant cytoplasm.
| |
| *Nuclear features of conventional prostate cancer (nucleoli, nuclear enlargement).
| |
| *Increased gland density.
| |
| | |
| Image: [http://www.nature.com/modpathol/journal/v17/n3/fig_tab/3800050f12.html#figure-title Atrophic carcinoma (nature.com)].
| |
| | |
| ==Mucinous prostate carcinoma==
| |
| ===General===
| |
| *Rare.
| |
| | |
| ===Microscopic===
| |
| Features:
| |
| *Cytologically malignant cells floating in mucin.
| |
| *> 25% of tumour mucinous.<ref name=pmid14976541>{{cite journal |author=Grignon DJ |title=Unusual subtypes of prostate cancer |journal=Mod. Pathol. |volume=17 |issue=3 |pages=316–27 |year=2004 |month=March |pmid=14976541 |doi=10.1038/modpathol.3800052 |url=}}</ref>
| |
| **One study suggests '''>=''' 25%.<ref>{{cite journal |author=Osunkoya AO, Nielsen ME, Epstein JI |title=Prognosis of mucinous adenocarcinoma of the prostate treated by radical prostatectomy: a study of 47 cases |journal=Am. J. Surg. Pathol. |volume=32 |issue=3 |pages=468–72 |year=2008 |month=March |pmid=18300802 |doi=10.1097/PAS.0b013e3181589f72 |url=}}</ref>
| |
| | |
| Notes:
| |
| *[[Mucinous carcinoma]] - percentage required to call varies by site.
| |
| | |
| ==Pseudohyperplastic prostatic adenocarcinoma==
| |
| ===Microscopic===
| |
| Features:<ref name=Ref_GUP77>{{Ref GUP|77}}</ref><ref name=pmid14688829>{{cite journal |author=Arista-Nasr J, Martinez-Benitez B, Valdes S, Hernández M, Bornstein-Quevedo L |title=Pseudohyperplastic prostatic adenocarcinoma in transurethral resections of the prostate |journal=Pathol. Oncol. Res. |volume=9 |issue=4 |pages=232–5 |year=2003 |pmid=14688829 |doi=PAOR.2003.9.4.0232 |url=}}</ref>
| |
| *Medium to large glands with an atypical morphology - '''key low power feature''':
| |
| **Papillary or pseudopapillary infoldings, luminal undulations, branching or cystic dilatation.
| |
| *Nuclear features of conventional prostate cancer (nucleoli, nuclear enlargement).
| |
| | |
| Image: [http://www.nature.com/modpathol/journal/v17/n3/fig_tab/3800050f13.html Pseudohyperplastic prostatic adenocarcinoma (nature.com)].
| |
| | |
| Notes:
| |
| *Usually associated with conventional (acinar) prostate adenocarcinoma.
| |
| *Pale abundant cytoplasm - similar to normal prostate.
| |
| | |
| ==Prostatic signet ring cell carcinoma==
| |
| ===General===
| |
| *Very rare - 9 cases in a series of 29,783 prostate cancer cases.<ref name=pmid21123640>{{Cite journal | last1 = Warner | first1 = JN. | last2 = Nakamura | first2 = LY. | last3 = Pacelli | first3 = A. | last4 = Humphreys | first4 = MR. | last5 = Castle | first5 = EP. | title = Primary signet ring cell carcinoma of the prostate. | journal = Mayo Clin Proc | volume = 85 | issue = 12 | pages = 1130-6 | month = Dec | year = 2010 | doi = 10.4065/mcp.2010.0463 | PMID = 21123640 }}</ref>
| |
| *Criteria vary - percentage of SRCs required for Dx varies from 20% to 50%.<ref name=pmid21123640/>
| |
| | |
| ===Microscopic===
| |
| Features:
| |
| *Signet ring cells - see ''[[basics]]'' article.
| |
| | |
| Image:
| |
| *[http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2996149/figure/F1/ Prostatic SRC (nih.gov)].
| |
| | |
| ==Sarcomatoid prostate carcinoma==
| |
| *[[AKA]] ''carcinosarcoma''.
| |
| | |
| ===Microscopic===
| |
| Features:<ref name=Ref_GUP80>{{Ref GUP|77 & 80}}</ref>
| |
| *Biphasic tumour:
| |
| *#Spindle cells (sarcomatous component).
| |
| *#*May include components of: osteosarcoma, chondrosarcoma and/or rhabdomyosarcoma.
| |
| *#Glandular component (like conventional prostate carcinoma).
| |
| *#*Typically stains PSA +ve, keratin +ve.
| |
| | |
| ==Small cell carcinoma of the prostate gland==
| |
| {{Main|Small cell carcinoma}}
| |
| Features:
| |
| *Nuclear moulding.
| |
| *Stippled chromatin.
| |
| *High [[NC ratio]].
| |
| *Small cells.
| |
| | |
| Notes:
| |
| *Similar to [[small cell carcinoma of the lung]].
| |
| *High-grade squamoid component favours metastatic [[urothelial carcinoma]].
| |
| **UCC usu. HWCK +ve.
| |
| | |
| ==Adenoid cystic/basal cell carcinoma of the prostate==
| |
| *Abbreviated ''ACBCC''.
| |
| ===General===
| |
| *Rare.
| |
| *Typically indolent - may be aggressive.<ref name=pmid14657711>{{Cite journal | last1 = Iczkowski | first1 = KA. | last2 = Ferguson | first2 = KL. | last3 = Grier | first3 = DD. | last4 = Hossain | first4 = D. | last5 = Banerjee | first5 = SS. | last6 = McNeal | first6 = JE. | last7 = Bostwick | first7 = DG. | title = Adenoid cystic/basal cell carcinoma of the prostate: clinicopathologic findings in 19 cases. | journal = Am J Surg Pathol | volume = 27 | issue = 12 | pages = 1523-9 | month = Dec | year = 2003 | doi = | PMID = 14657711 }}</ref>
| |
| | |
| ===Microscopic===
| |
| Features:
| |
| *[[Adenoid cystic carcinoma]]-like and [[basal cell adenoma]]-like:
| |
| **Nests of cells that have round spaces filled by whispy blue mucin.
| |
| **Dense collagenous stroma.
| |
| | |
| Images:
| |
| *[http://www.webpathology.com/image.asp?case=23&n=15 Adenoid basal cell tumour (webpathology.com)].
| |
| *[http://www.webpathology.com/image.asp?case=23&n=16 Adenoid basal cell tumour (webpathology.com)].
| |
|
| |
|
| ===IHC=== | | =Prostate cancer= |
| *HER2/neu +ve (strong).<ref name=pmid17142577>{{Cite journal | last1 = Iczkowski | first1 = KA. | last2 = Montironi | first2 = R. | title = Adenoid cystic/basal cell carcinoma of the prostate strongly expresses HER-2/neu. | journal = J Clin Pathol | volume = 59 | issue = 12 | pages = 1327-30 | month = Dec | year = 2006 | doi = 10.1136/jcp.2005.035147 | PMID = 17142577 }}</ref>
| | {{Main|Prostate cancer}} |
| | This is a big topic that is dealt with in its own article. |
|
| |
|
| =See also= | | =See also= |
| Line 794: |
Line 260: |
| {{reflist|2}} | | {{reflist|2}} |
|
| |
|
| =External links=
| |
| *[http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2006/prostate06_ckw.pdf CAP prostate check list] - cap.org.
| |
| *[http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2006/prostate06_ckw.pdf CAP prostate protocol] - cap.org.
| |
| *[http://162.129.103.34/prostate/ Gleason score quiz] - Johns Hopkins Prostate Center.
| |
|
| |
|
| [[Category: Genitourinary pathology]] | | [[Category: Genitourinary pathology]] |