Thyroid gland
The thyroid gland is an important little endocrine organ in the anterior neck. It is not infrequently afflicted by cancer... but the common cancer has such a good prognosis there is debate about how aggressively it should be treated. The cytopathology of the thyroid gland is dealt with in the thyroid cytology article. It frustrates a significant number of pathologists, as the criteria for cancer are considered a bit wishy-washy.
Thyroid specimens
They come in 3 common varieties:
- Hemithyroid.
- Done to get a definitive diagnosis.
- May be a "completion" - removal of the other half following definitive diagnosis.
- Total thyroid.
- Done for malignancy or follicular lesion.
- FNA (fine needle aspiration).
- done to r/o malignancy.
Gross pathology:
- White nodules - think:
- Lymphoid tissue.
- Papillary thyroid carcinoma - may be calcified.[1]
Common diagnoses
- Nodular hyperplasia.
- Lymphocytic thyroiditis.
- Papillary thyroid carcinoma -- most common cancer.
- Follicular adenoma.
- Follicular thryoid carcinoma.
- Parathyroid tissue.
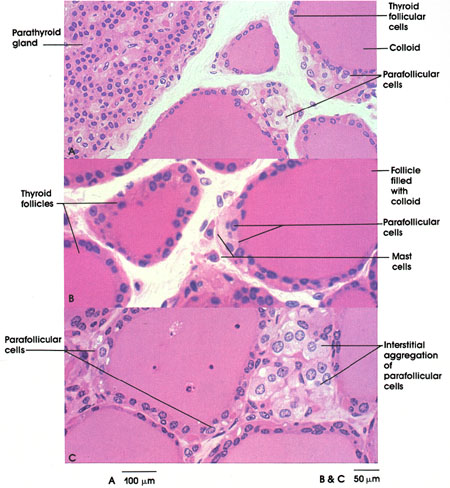
Parathyroid tissue
General:
- Identification of normal can be tricky.
Features:[2]
- Low power:
- May vaguely resemble lymphoid tissue - may have hyperchromatic cytoplasm.
- Does not have follicular centres like a lymph node.
- May form gland-like structure and vaguely resemble the thyroid at low power.
- Cytoplasm may be clear[3] - key feature.
- Surrounded by a thin fibrous capsule.
- May vaguely resemble lymphoid tissue - may have hyperchromatic cytoplasm.
- High power:
| Name | Staining (cytoplasm) | Quantity of cells | Cytoplasm (quantity) | Function |
| (parathyroid) chief cells | intense hyperchromatic to eosinophilic (see note) | abundant | moderate | manufacture PTH |
| oxyphil cells | moderate/light hyperchromatic to eosinophilic | rare | abundant | ? |
Notes:
- Cytoplasmic staining varies considerably on H&E preparations - it may vary from hyperchromatic[6] to clear to eosinophilic[7].
- Chief cells tend to stain more intensely than oxyphil cells.
Thyroid vs. parathyroid (see: parathyroid image):
{kind=link}
- Parathyroid cytoplasm:
- Hyperchromatic.
Parathyroid vs. lymphoid tissue (see parathyroid image):
{kind=link}
- Parathyroid:
- No germinal centres.
- Gland-like/follicular-like arrangement -- much smaller than normal follicles of
- Occasional cell with rim of clear cytoplasm (oxyphil?).
Images:
Parathyroid hyperplasia
- Parathyroid hyperplasia - classically assoc. with renal failure.
- Chief cell hyperplasia - associated with MEN I, MEN IIa.[8]
Parathryoid adenoma
MEN I:
- Parathyroid adenoma.
- Pancreatic neuroendocrine tumours.
- Pituitary adenoma.
MEN IIa/IIb (II/III):
- Parathyroid adenoma.
- Medullary thyroid carcinoma.
- Pheochromocytoma.
Image: [http://library.med.utah.edu/WebPath/jpeg4/ENDO091.jpg Parathyroid adenoma (med.utah.edu).[9]
{kind=link}
Benign
Nodular hyperplasia
- Very common benign diagnosis.
- If you've seen a handful of thyroids you've seen this.
- Follicles of variable size.
- Nodules maybe well circumscribed (on gross), but do not have a thick fibrous capsule.
- Negatives:
- No nuclear features suggestive of malignancy (papillary carcinoma).
- Not cellular.
Follicular adenoma
- Most common neoplasm of thyroid[10]
- Encapusled lesion (surrounded by fibrous capsule).
- Cellular.
- Negatives
- No nuclear features suggestive of papillary carcinoma.
Graves disease
- Often misspelled "Grave's disease".
- Hyperthyroidism.
- Etiology: autoimmune.
Gross
Features:[11]
- Enlarged 50-150 g.
- "Beefy-red" appearance, looks like raw beef.
Microscopic
Features:
- Papillae (may mimic papillary thyroid carcinoma in this respect).
Granulomatous thyoiditis
Features:[12]
- AKA de Quervain disease.
- Women > men.
Ridel thyroiditis
- Fibrosis.
- Specimen often fragmented as it was difficult to remove.
- Thought to be related to retroperitoneal fibrosis.
Hashimoto's thyroiditis
Clinical
Presentation:
- Hypothyroid
Associations:[13]
- Antimicrosomal (antithyroid peroxidase) +ve.
- Antithyroglobulin +ve.
- Increased risk of B-cell lymphoma.
Etiology
- Autoimmune.
- Often genetic/part of a syndrome.
Diagnosis
Malignant neoplasm
There are a bunch of 'em. The most common, by far, is papillary.
Papillary
Clinical
Basic clinican knowledge - P's:
- Palpable nodes.
- Popular (most common malignant neoplasm of the thyroid).
- Prognosis is good.
- Pre-Tx iodine scan.
- Post-Sx iodine scan.
- Psammoma bodies.
Notes:
- Associated with radiation exposure.[16]
Microscopic
Features:
- Nuclear changes - key feature.
- "Shrivelled nuclei"/"raisin" like nuclei, nuclei with a wavy nuclear membrane.
- Nuclear grooves.
- Nuclear inclusions.
- Nuclear clearing (only on permanent section) - also known as "Orphan Annie eyes".
- Overlap of nuclei - "cells do not respect each other's borders" (easy to see at key feature at low power).
- Classically has papillae (nipple-like shape).
- Absence of papillae does not exclude diagnosis.
- Psammoma bodies.
- Circular, acellular, eosinophilic whorled bodies.
- Not necessary to make diagnosis.
- Arise from infarction & calcification of papilla tips.[17]
Notes:
- Psammoma bodies are awesome if you see 'em, i.e. useful for arriving at the diagnosis.
- If there are no papillae structures -- you're unlikely to see psammomas.
- At low power look for cellular areas/loss of follicles.
- Nuclear clearing seen in:
- Nuclear overlapping is easy to see at lower power-- should be the tip-off to look at high power for nuclear features.
- Nuclear inclusions are quite rare and not required to make the diagnosis -- but a very convincing feature if seen.
- Papillae may be seen in Graves disease.
Subtypes if papillary
There are many.
Tall cell variant
Features:[19]
- 50% of cells with height 2x the width.[20][21]
- There is some disagreement on these criteria.[21]
- Eosinophilic cytoplasm.
- Well-defined cell borders.
- Nucleus stratified; basal location, i.e. closer to the basement membrane.
Negative:
- Nuclei not pseudostratified, if pseudostratified consider columnar cell variant.
Columnar cell variant
Epidemiology:
- Poor prognosis.
Features:
- Elongated nuclei (similar to colorectal adenocarcinoma) - key feature.
- Pseudostratification of the nuclei (like in colorectal adenocarcinoma), differentiates from tall cell variant - key feature.
- "Minimal" papillary features.
- "Tall cells".
- Clear-eosinophilic cytoplasm.
- Mitoses common.
Image: Tall cell variant Pa ca (wiley.com).
Follicular variant
May be confused with follicular carcinoma or follicular adenoma.
Features:
- Prominent follicles.
Cribriform-morular variant
Features:
- Cribriform pattern.
- Morules - balls of tissue.
Insular carcinoma
General:[22]
- Rare - approximately 5% of all thyroid carcinomas.
- Thought to be a separate tumour from papillary thyroid carcinoma and follicular thyroid carcinoma with a focal insular pattern.
- Some lump this entity with papillary carcinoma, i.e. consider it a variant of papillary thyroid carcinoma.
Features:[22]
- Islands of cells - key feature.
- Scant cytoplasm.
- Nuclei monomorphic and round.
DDx:[23]
- Medullary thyroid carcinoma.
- Poorly differentiated thyroid carcinoma.
Follicular thyroid carcinoma
Clinical
- FNA NOT diagnosable.
- Far away mets (sometimes).
- Female predominant.
- Favourable prognosis.
Histology
- IMPOSSIBLE to differentiate from follicular adenoma on FNA (no cytologic differences).
- Defined by invasion through the capsule.
Medullary thyroid carcinoma
General
- Abbreviated MTC.
Clinical
3 M's:
- aMyloid.
- Median node dissection done.
- MEN IIa syndrome/MEN IIb syndrome.
- Medullary thyroid carcinoma.
- Pheochromocytoma.
- Parathyroid adenoma.
Epidemiology
- Very rare.
- Poor prognosis.
- May be genetic (MEN IIa/b syndrome).
- Arises from C cells (which produce calcitonin).
Histology
Features:
- Nuclei with "neuroendocrine features".
- Small, round nuclei.
- Coarse chromatin (salt and pepper nuclei).
- Amyloid deposits - fluffy appearing acellular eosinophilic material in the cytoplasm.
- C-cell hyperplasia (associated with familial forms of MTC).
- C cells (AKA parafollicular cell): abundant cytoplasm - clear/pale.
IHC:[24]
- Calcitonin +ve - it arises from C cells (which produce calcitonin).
- Congo-red +ve (amyloid present) - mnemonic: CRAP -- congo red amyloid protein.
- Neuroendocrine markers.
- CEA +ve (often better staining than calcitonin).[25]
Image:
{kind=link}
{kind=link}
Anaplastic thyroid carcinoma
Epidemiology
- Very rare.
- Horrible prognosis.
Histology
Features:
- Cytologically malignant:
- Huge NC ratio.
- Mitoses.
- +/-Necrosis.
Image: Anaplastic thyroid carcinoma with a component of papillary thyroid carcinoma (WC).
{kind=link}
IHC
Thyroid IHC - general comments
- Not really useful.
- Papers with very small sample sizes abound.
Follicular thyroid carcinoma vs. papillary thyroid carcinoma
See also
References
- ↑ BEC. 20 October 2009.
- ↑ http://www.medicalhistology.us/twiki/pub/Main/ChapterFourteenSlides/b56b_parathyroid_40x_he_labeled.jpg
- ↑ http://pathology.mc.duke.edu/research/Histo_course/parathyroid2.jpg
- ↑ http://www.bu.edu/histology/p/15002loa.htm
- ↑ http://dictionary.reference.com/search?q=oxyphil%20cell
- ↑ http://www.deltagen.com/target/histologyatlas/atlas_files/endocrine/parathyroid_and_thyroid_glands_20x.jpg
- ↑ http://instruction.cvhs.okstate.edu/Histology/HistologyReference/hrendo.htm
- ↑ URL: http://www.pathconsultddx.com/pathCon/diagnosis?pii=S1559-8675%2806%2970475-2. Accessed on: 29 July 2010.
- ↑ URL: http://library.med.utah.edu/WebPath/EXAM/IMGQUIZ/enfrm.html. Accessed on: 6 December 2010.
- ↑ Thompson, Lester D. R. (2006). Endocrine Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 51. ISBN 978-0443066856.
- ↑ Thompson, Lester D. R. (2006). Endocrine Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 30. ISBN 978-0443066856.
- ↑ Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Oberman, Harold A; Reuter, Victor E (2004). Sternberg's Diagnostic Surgical Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 559. ISBN 978-0781740517.
- ↑ Poropatich C, Marcus D, Oertel YC (1994). "Hashimoto's thyroiditis: fine-needle aspirations of 50 asymptomatic cases". Diagn. Cytopathol. 11 (2): 141–5. PMID 7813361. http://www3.interscience.wiley.com/journal/112701408/abstract?CRETRY=1&SRETRY=0.
- ↑ Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Oberman, Harold A; Reuter, Victor E (2004). Sternberg's Diagnostic Surgical Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 560. ISBN 978-0781740517.
- ↑ Lefkowitch, Jay H. (2006). Anatomic Pathology Board Review (1st ed.). Saunders. pp. 672. ISBN 978-1416025887.
- ↑ Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Oberman, Harold A; Reuter, Victor E (2004). Sternberg's Diagnostic Surgical Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 564. ISBN 978-0781740517.
- ↑ Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Oberman, Harold A; Reuter, Victor E (2004). Sternberg's Diagnostic Surgical Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 565. ISBN 978-0781740517.
- ↑ Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Oberman, Harold A; Reuter, Victor E (2004). Sternberg's Diagnostic Surgical Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 566. ISBN 978-0781740517.
- ↑ Urano M, Kiriyama Y, Takakuwa Y, Kuroda M (April 2009). "Tall cell variant of papillary thyroid carcinoma: Its characteristic features demonstrated by fine-needle aspiration cytology and immunohistochemical study". Diagn. Cytopathol.. doi:10.1002/dc.21086. PMID 19373912.
- ↑ http://pathologyoutlines.com/thyroid.html#tallcellvariant
- ↑ 21.0 21.1 Ghossein R, Livolsi VA (November 2008). "Papillary thyroid carcinoma tall cell variant". Thyroid 18 (11): 1179–81. doi:10.1089/thy.2008.0164. PMID 18925842.
- ↑ 22.0 22.1 Rufini V, Salvatori M, Fadda G, et al. (September 2007). "Thyroid carcinomas with a variable insular component: prognostic significance of histopathologic patterns". Cancer 110 (6): 1209–17. doi:10.1002/cncr.22913. PMID 17665497.
- ↑ Endo. fellow. 17 September 2009.
- ↑ http://pathologyoutlines.com/thyroid.html#medullary
- ↑ SB. 7 January 2010.
- ↑ 26.0 26.1 Ordóñez NG, El-Naggar AK, Hickey RC, Samaan NA (July 1991). "Anaplastic thyroid carcinoma. Immunocytochemical study of 32 cases". Am. J. Clin. Pathol. 96 (1): 15–24. PMID 1712540.
- ↑ 27.0 27.1 Rydlova, M.; Ludvikova, M.; Stankova, I. (Jun 2008). "Potential diagnostic markers in nodular lesions of the thyroid gland: an immunohistochemical study.". Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 152 (1): 53-9. PMID 18795075.
- ↑ Papotti, M.; Rodriguez, J.; De Pompa, R.; Bartolazzi, A.; Rosai, J. (Apr 2005). "Galectin-3 and HBME-1 expression in well-differentiated thyroid tumors with follicular architecture of uncertain malignant potential.". Mod Pathol 18 (4): 541-6. doi:10.1038/modpathol.3800321. PMID 15529186.
{kind=link}
{kind=link}