Placenta
The placenta feeds the developing baby, breathes for it and disposes of its waste.
Clinical
Examination of the placenta
- Most placentas are not examined by a pathologist.
Some indications for exam by a pathologist:
- Abnormalities in the:
- Fetus:
- Bad fetal outcome.
- Suspected or known congenital abnormalities or chromosomal abnormalities.
- Mother:
- Infection/suspected infection.
- Pre-term labour.
- Maternal disease (e.g. SLE, coagulopathy).
- Complicated pregnancy (preclampsia, pregnancy induced hypertension, gestational diabetes).
- Placenta:
- Unusual gross characteristics.[1]
- Fetus:
A more detailed list is given by Hargitai et al.[2]
Bleeding in late pregnancy
DDx of bleeding in late pregnancy:
- Placental abruption (most common).
- Placenta previa.
- Vasa previa (fetus losing blood).
Clinical screening tests
- PAPP-A - low values seen in aneuploidy.[3]
Normal histology
Villi
This is dealt with in a separate article that also covers the types of trophoblast (cytotrophoblast, syncytiotrophoblast, intermediate trophoblast).
Cord
Omphalomesenteric duct remnant
- AKA vitelline duct.
- Benign embryologic remnant.
Features:
- Duct with benign looking cuboidal epithelium.
Allantoic duct remnant
- Benign embryologic remnant.
Features:
- Duct with benign looking flat epithelium.
Vitelline artery remnant
Features:
- Small artery in the cord.
Membranes
Amnion
General:
- Next to fetus, surrounds amniotic fluid, avascular.
Characteristics:
- Characterized by a single layer of cells.[4]
- Cuboidal/squamoid shape.
- Eosinophilic cytoplasm.
- Central nucleus.
- Squamous metaplasia may be seen at cord insertion.
- Basement membrane.
- 'Compact layer'.[4]
- 'Fibroblastic layer'.[4]
Chorion
General:
- Surrounds amnion.
Characteristics:
- Layers:[5]
- 'Reticular layer' - cellular (inner aspect).
- 'Pseudo-basemement membrane'.
- 'Outer trophoblastic layer'.
- Has blood vessels.
- Opposed to "trophoblastic X cells" on side opposite of amnion.[4]
- Beneath of the "trophoblastic X cells" is decidua (mnemonic NEW = nucleus central, eosinophilic, well-defined cell border), which is maternal tissue.
Common terms
- Chorionic plate - fetal aspect of placenta.
- Basal plate - maternal aspect of placenta.
- Has extravillous trophoblast.
- Place to look for maternal vessels.
Grossing
This is often very quick. The gross is quite important, as some things cannot be diagnosed microscopically.
General
- Dimensions:
- Disc.
- Length of cord, diameter of cord.
- Accessory lobes - dimensions.
- Two lobes of equal size + cord arises in between = bilobate placenta.
- Mass (weight).
- Should be done 'trimmed' (cord cut-off, membrane cut-off).
- Should be done when placenta is "fresh", i.e. not fixed -- as mass tables are based on fresh state.
- Umbilical cord
- Attachment.
- Location: central, eccentric, marginal.
- Marginal attachment assoc. with hypertension[6]
- Membranous or velamentous (veil-like) insertion.
- Vessels separate/branch prior to reaching placental disc.
- Furcate insertion - vessel run on fetal surface (more exposed to trauma).
- Location: central, eccentric, marginal.
- Knots (false vs. true).
- False knots are nothing to worry about -- look like a knot but aren't really one.
- Twisting/coiling - 1-3 coils/10 cm is normal.
- Number of vessels.
- Normal: 2 arteries, 1 vein.
- Attachment.
- Membranes - shiny & translucent - normal (green, opaque/dull - chorioamnionitis).
- Attachment: marginal (normal), circummarginate (inside edge), circumvallated (folding on self).
- Site of rupture - if obvious; low point of rupture suggests low-lying placenta.
- Placental disc.
- Fetal surface - normal is shinny.
- Dull in chorioamnionitis.
- Maternal surface
- Are the cotyledons intact?
- Adherent clot?
- Parenchyma - after sectioning:
- White vs. red nodules.
- Fetal surface - normal is shinny.
Notes:
- Parenchymal nodules - a brief DDx:
- White: infarct (chronic), thrombi, chorangioma, perivillous fibrin deposition.
- Red: infarct (acute), thrombi.
Sections
- Cord two sections.
- Membranes (rolled).
- Cord at insertion + disc.
- Placenta - full thickness (maternal and fetal surface).
- Sections should not be taken at the margin of the disc.
Placental membranes
Appearance:[7]
- Normal - shiny.
- Choriomnionitis - opaque/dull.
- Meconium - green.
- Amnion nodosum - yellow patches.
- Some describe 'em as white.[8]
Placental mass
Placental mass by gestational age:[9]
| Gest. Age/Percentile | 25% | 50% | 75% |
| 32 weeks | 275 g | 318 g | 377 g |
| 36 weeks | 369 g | 440 g | 508 g |
| 40 weeks | 440 g | 501 g | 572 g |
Linear regression - placental mass-gestational age
Based on the table in the AFIP book[10] I generated the following regression lines:
| 50% | 10% | 90% | |
| slope (g/week) | 21.58088235 | 19.70588235 | 25.40196078 |
| y-intercept (g) | -357.4558824 | -397.2352941 | -366.7254902 |
| Pearson (r) | 0.988670724 | 0.988268672 | 0.982206408 |
placental mass = slope x gestational age + intercept
What to remember...
Extrapolated from the linear regression (see above):
- 50% at term = 500 grams.
- 50% at 26 weeks = 200 grams.
- The change in mass/week is approximately linear and equal to 300 grams / 14 weeks ~ 20 grams/week.
- The spread in mass between 10% and 90%, crudely estimated, is 200 grams (for GA=26-40).
Overview of placental pathology
Approach
The pathology of the placenta is diverse and is not easy to group.
It terms of remembering things. It is probably easiest to take a combined anatomical, etiologic and morphologic approach.
Anatomical basis:
- Cord.
- Membranes.
- Disc.
Etiologic:
- Congential.
- Infectious.
- Neoplastic.
- Endocrine.
- Trauma.
- Vascular.
- Degenerative.
- Autoimmune.
- Toxic.
- Idiopathic.
Compartmental:
- Vasculature.
- Membranes.
- Parenchyma:
- Maternal part (decidua).
- Fetal part (villi, cord).
Common entities/diagnoses
- Normal.
- Chorioamnionitis.
- Placental abruption.
- Meconium.
- Hypertensive changes.
Sign-out
What should be commented on...
- Placenta:
- Maturity of villi (2nd or 3rd trimester).
- Infarction?
- Subchorionic less important than maternal aspect.
- Peripheral aspect of placental disc less important than central region of disc.
- Blood vessels.
- Maternal.
- Fetal.
- Membranes.
- Membranitis?
- Chorioamnionitis?
- Cord:
- 3 vessel?
- Vasculitis/inflammation?
Mnemonic: chorio, cord, vessels, villi (maturity, infarction).
Cord pathology
- Two vessel cord.
- Hypercoiling/Hypocoiling.
- Abnormal insertion.
- Cord knots (true vs. false).
- Strictures.
- Hematoma.
- Hemangioma.
- Benign cyst.
Two vessel cord
- AKA single umbilical artery.
Associations
- Associated with congenital abnormalities, esp. cardiac - key point.[11]
- Thought to be an acquired defect (as prevalence is lower in early in gestation).
- May be seen in association of other cord abnormalities (e.g. marginal insertion, velamentous insertion).
- In apparently well (liveborn) infants it is associated with (occult) renal abnormalities, specifically vesico-ureteric reflux; there is no evidence for other abnormalities.[12]
- Associated with maternal diabetes.[13]
Image:
{kind=link}
Insertion
Marginal insertion
Definition:
- The umbilical cord is attached to the placental disc at its margin.
Prevalence:
- Approximately 12% of placentas.[11]
Relevance:
- None according to WMSP.[11]
- In theory, the cord, dependent on its relation to the internal os, is at greater risk of injury (leading to vasa previa) and compression (fetal hypoxia). A retrospective study found cord position in relation to the internal os is predictive for vasa previa.[15]
Velamentous insertion
Definition:
- The umbilical cord inserts into the fetal membranes.[11]
- The vessels are not protected by Wharton's jelly.
- Wharton's jelly = the connective tissue surrounding the vessels in the cord.
- The vessels are not protected by Wharton's jelly.
Details:[11]
- 3/4 of the time the vessel also branch; in the remaining 1/4 the vessels stay together.
Relevance:
- Increased risk of vasa previa.[15]
Knots
General
Gross
Work-up:[17]
- Diameter measures and colour on both sides of the knot.
- Knot should be untied to assess for deformation of Wharton's jelly.
- Sections from both sides of the knot - to look for thrombi.
Note:
- False knots (large diameter - focally) are common - they cannot be untied.
Microscopic
Features:
- +/-Thrombi.
- Fibrin deposition.
- +/-Lines of Zahn.
Images:
Coiling
- Hypo- and hypercoiling are both considered problematic.[11]
- Normal: 1-3 coils/10 cm.[18]
- Associated with cord stricture, which is usu. at the fetal end of the cord.[19]
Notes:
- There is little uniformity in how coiling is assessed in the medical literature - though 10% and 90% are considered the cut-points for normal.[20]
- What are the 10% and 90% cut-points? They are not given in WMSP. UT access to a journal article[21] that might have it is screwed-up.
Cord hematoma
Features:[19]
- Rare ~ 1/5500.
- Mortality ~50% is severe.
Image: Hematoma (flylib.com).[22]
{kind=link}
Membranes
- Squamous metaplasia.
- Chorioamnionitis - see infection section.
Amnion nodosum
General
- Associated with (long-standing) oligohydramnios.[23]
- Should be separated from squamous metaplasia of amnion.
Gross
- Yellow patch or yellow nodules.
- Some think they are white.[24]
Image: Amnion nodosum (webpathology.com).
Microscopic
Features:
- Simple epithelium of amnion replaced by (non-keratinizing) stratified squamous epithelium.
Image: Amnion nodosum (webpathology.com).
Passage of meconium
General
- Associated with fetal distress.
- Small amount - at term - is considered to be normal.
Gross
- Green/green discolourization.
Microscopy
Features:[25]
- Meconium histiocytes - key feature.
- Macrophages with brown fine granular pigment.
- Pseudostratified epithelium (amnion) - low power.
- Amnion - columnar morphology (normally cuboidal).
- "Drop-out" of individual amnion cells / loss of individual cells.
Time of meconium passage:[26]
- <1 h - no staining of membranes.
- 1-3 h - amnion is stained.
- >3 h - chorion is stained.
DDx:
- Hemosiderin-laden macrophages.
- This is sorted-out with an iron stain -- see below.
Notes:
- The above time course is disputed - in vitro experiments suggest it is considerably longer.[27]
Images:
{kind=link}
{kind=link}
Special stains
- Hemosiderin +ve in hemosiderin-laden macrophages.
- PAS +ve in meconium-laden macrophages.[28]
Useful to differentiate hemosiderin-laden macrophages and meconium laden macrophages:
- Hemosiderin stain -- +ve for old blood.
- Prussian-blue stain = hemosiderin stain.[29]
Notes:
- PAS-D -- +ve in meconium... though may rarely stain hemosiderin.
- Meconium contains bile.[30]
Squamous metaplasia
- Benign common finding - no clinical significance.[31]
- Needs to be separated from amnion nodosum.[32]
Image:
{kind=link}
Twin placentas
These are often submitted... even if they are normal. In these specimens, usually, the chorion is the key.
It covers:
- Monozygotic vs. dizygotic twins.
- Twin-to-twin transfusion syndrome.
Diseases of the placental attachment
Placenta acreta/percreta/increta
Placenta attaches to the uterus deeper than it should.
Placental abruption
General
Classic clinical manifestations:[34]
- Vaginal bleeding (~70%).
- Abdominal pain (~50%).
- Fetal heart rate abnormalities (~70%).
Sign-out:
- Pathologists should sign-out this as "focal adherent retroplacental hematoma".
- The pathologic findings may be due to abruption or manual removal of the placenta.
Gross
Features:[35]
- Large adherent blood clot.
- Disc depression on maternal side.
Notes:
- Loosely attached clot less convincing.
- Central haemorrhage is the most worrisome.
Microscopic
Features:
- Decidual hemorrhage.
- Blood in the decidua.
- Intravillous hemorrhage, AKA villous stromal hemorrhage.
- "Bags of blood" - blood outside of vessels in the villi.
- Should not be confused with congested villi.
- "Bags of blood" - blood outside of vessels in the villi.
Notes:
- There are no definitive microscopic findings for placental abruption.
- Intravillous hemorrhage is non-specific - may arise in the following: early placental infarct, cord compression, abdominal trauma.
Inflammatory placenta
Infection
General:[36]
- Infection usually ascending, i.e. from vagina up through cervix.
- Associated with intercourse.
- Hematogenous rare - manifest as villitis.
- Think TORCH infections (toxoplasmosis, others (syphilis, TB, listeriosis), rubella, cytomegalovirus, herpes simplex virus).
- Funisitis usually follows chorioamnionitis.
- Inflammatory cells in umbilical cord are fetal (trivia).
Types (by site)[36]
- Fetal membranes: chorioamnionitis, membranitis.[37]
- Umbilical cord: funisitis.
- Placenta: placentitis, villitis.
Grading infection (chorioamnionitis, membranitis, funisitis)
Membranitis:[37]
- PMNs - decidua only.
- PMNs - in subamniotic tissue.
- 1 or 2 + necrosis in decidua or chorion/subamniotic tissue.
Chorioamnionitis:[37]
- placental chorionic plate only.
- 1 + subamniotic tissue.
- 1 or 2 + necrosis or abscess.
Sternberg separates vasculitis and funisitis without really explaining the terms[37] -- I presume: vasculitis = inflammation of vessels in the umbilical cord. funisitis = inflammation of the cord (vessels and Wharton jelly).
Umbilical cord vasculitis:[37]
- +0.5 for each vessel.
- +0.5 for each vessel with severe involvement.
Umbilical funisitis:[37]
- focal inflammation.
- diffuse inflammation.
- necrosis - in vessels or Wharton jelly.
Note: There is no such thing as chorionitis.[38]
Villitis of unknown etiology
- Abbreviated VUE.
General
Features:[39]
- Usually term placenta.
- Prevalence: 5% to 15% of all placentas.
- Associated with:
- Intrauterine growth restriction.
- Recurrent reproductive loss -- key point.
Etiology:
- Unknown - as the name of the entity suggests.
- Suspected to be immune-mediated.
Microscopic
Features:[39]
- Lymphocytes in villous stroma - key feature.
- Usually focal/patchy.
- Lymphocytes: maternal derivation, T-lymphocytes -- mostly CD8-positive.
- +/-Intervillositis (lymphocytes between villi).
- +/-Histiocytes.
- No plasma cells - this suggests an infectious etiology.[40]
- Plasma cells may be in the decidua.
Notes:
- Neutrophils are usually absent. A significant number of 'em is suggestive of an infectious villitis.
- Infective villitis is usu. B-cell predominant.
Images:
- VUE (bmj.com).[41]
- VUE (flickr.com).[42] **CHECK**
{kind=link}
{kind=link}
Infarction
True infarcts
General
- Associated with retroplacental hematoma.
Gross
Features:[19]
- Early - red.
- Late - white/grey.
Images:
Microscopic
Features:
- Necrosis of villi; hyaline material (acellular eosinophilic material) replaces the stroma of the villi.
- Loss of intervillous space.[19]
- Villi appear to be crowded.[43]
- Normal spacing is ~1x smallest villus or larger.
- In perivillous fibrin deposition - spacing usu. larger than normal.
- Normal spacing is ~1x smallest villus or larger.
- Villi appear to be crowded.[43]
- Prominent syncytial knots.
- Thickened trophoblastic basement membrance (below cytotrophoblasts).
- +/-Changes seen in decidual vasculopathy:
- Acute atherosis (vaguely like atherosclerosis).
- Fibrioid necrosis.
- Vessel wall lipid deposition.
- Acute atherosis (vaguely like atherosclerosis).
Images:
- Recent infarct (pathweb.uchc.edu).
- Placental infarct (umpmc.edu).[44]
- Placental infarct - necrotic villi (mda-sy.com).
{kind=link}
Significant infarcts
- > 3cm --or-- central location --or-- in 1st or 2nd trimester.
- Small foci are accepted in term placentae - typically at periphery.
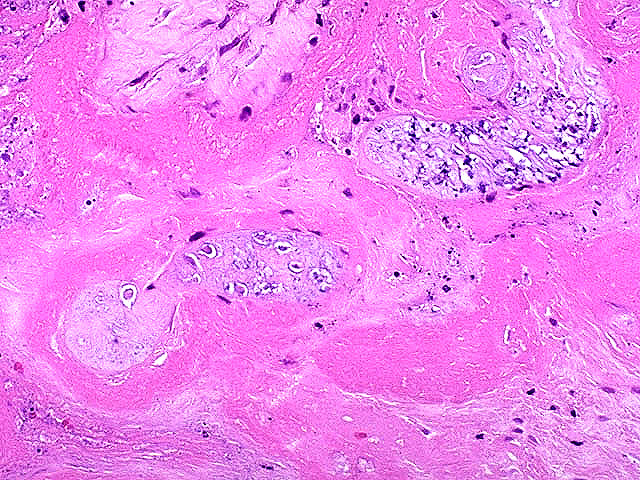
Perivillous fibrin deposition
- Massive perivillous fibrin deposition is assoc. with anti-phospholipid antibody (APLA) syndrome.[45]
- APLA is assoc. with recurrent miscarriage - can be treated with heparin + ASA.[45]
- Thought to be an immunologic problem - resulting in platelet activation and fibrin deposition.[45]
Gross
- Pale (white).
- Firm.
- White fibrous sepatae.
Microscopy
Features:
- Acellular eosinophilic material around formed villi.
- Obliteration of intervillous space.
- Intervillous distance increased vis-a-vis normal - key feature.
Notes:
- Nuclei of villi are usu. preserved.
- Villi may have secondary infarction, i.e. there may be nuclear destruction (karyolysis, karyorrhexis, pyknosis).
Fetal disease
Fetal thrombotic vasculopathy
General
- May cause IUGR.
- Associated with cerebral palsy and common in perinatal deaths.[46]
Microscopic
Features:
- Thrombus in the fetal vasculature +/- recanalization.
- Eosinophilic (light pink on H&E), moderately granular intravascular material (fibrin) with layering.
Images:
{kind=link}
{kind=link}
Hemorrhagic endovasculitis
- Abbreviated HEV.
General
- Associated with stillbirth.[49]
Microscopic
Features:[50]
- Walls of the (fetal) placental blood vessels (in the villi) are disrupted.
- +/-Intraluminal necrotic debris.
- RBC fragmentation.
Maternal disease
Hypertensive changes
General
Associated pathologic changes:[51]
- Placental infarcts.
- Increased syncytial knots.
- Hypovascularity of the villi.
- Cytotrophoblastic proliferation.
- Thickening of the trophoblastic basement membrane.
Microscopic
Features:[51]
- Enlarged endothelial cells - fetal capillaries.
- Atherosis of the spiral arteries - placental bed (maternal).
Notes:
- One should look for the changes in the membrane roll, not the maternal surface.[52]
Hypertrophic decidual vasculopathy
General
- A change seen in hypertension.
Microscopic
Features:[53]
- Mild or moderate:
- Perivascular inflammatory cells.
- +/-Vascular thrombosis.
- Smooth muscle hypertrophy.
- Endothelial hyperplasia.
- Above two lead to narrowing of the decidual spiral arteries[54] -- key feature.
- Severe:[53]
- Atherosis of maternal blood vessels.
- Foamy macrophages within vascular wall.
- Fibrinoid necrosis of vessel wall (amorphous eosinophilic material vessel wall).
- Atherosis of maternal blood vessels.
General:
- Seen in intrauterine growth restriction (IUGR).
Images:
{kind=link}
{kind=link}
HELLP syndrome
General
- Diagnosed clinically.
- Pathologically not the same as severe preclampsia.[55]
Definition:
- H = hemolysis.
- EL = elevated liver enzymes.
- LP = low platelets.
Microscopic
Features:[56]
- Thrombotic microangiopathic vasculopathy.
- In essence: severe hypertrophic decidual vasculopathy. (???)
Tumours
Chorangioma
General
- Hamartoma-like growth in the placenta consisting of blood vessels.[57]
Epidemiology:
- Often benign.
- May be association with:
- Fetal maternal haemorrhage.
- Hydrops.
- IUGR.
Gross
- White lesions.
- Occasionally red lesions.
Microscopic
Features:
- Mass of capillaries.
Image:
{kind=link}
Chorangiosis=
General
- Should not be confused with chorangioma.
- Rare.
Associations:
- Maternal hypoxia:
- Smoking.
- Altitude.
- Diabetes.
Microscopic
Features:
- Increased blood vessels in the terminal villi.
- Not well circumscribed.
Notes:
- Usually not seen on gross pathology.
See also
References
- ↑ Yetter JF (March 1998). "Examination of the placenta". Am Fam Physician 57 (5): 1045–54. PMID 9518951.
- ↑ Hargitai B, Marton T, Cox PM (August 2004). "Best practice no 178. Examination of the human placenta". J. Clin. Pathol. 57 (8): 785–92. doi:10.1136/jcp.2003.014217. PMC 1770400. PMID 15280396. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1770400/.
- ↑ URL: http://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=5069. Accessed on: 7 July 2010.
- ↑ 4.0 4.1 4.2 4.3 Sternberg, Stephen S. (1997). Histology for Pathologists (2nd ed.). Lippincott Williams & Wilkins. pp. 974. ISBN 978-0397517183.
- ↑ Sternberg, Stephen S. (1997). Histology for Pathologists (2nd ed.). Lippincott Williams & Wilkins. pp. 977. ISBN 978-0397517183.
- ↑ J Anat. Soc. India 49(2) 149-152 (2000). Available at: http://www.indmedica.com/anatomy/aindex1.cfm?anid=41. Accessed on: January 21, 2009.
- ↑ Lester, Susan Carole (2005). Manual of Surgical Pathology (2nd ed.). Saunders. pp. 461. ISBN 978-0443066450.
- ↑ CS. 7 February 2011.
- ↑ AFIP Placental pathol. ISBN: 1-881041-89-1. P.312
- ↑ AFIP Placental pathol. ISBN: 1-881041-89-1. P.312
- ↑ 11.0 11.1 11.2 11.3 11.4 11.5 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 464. ISBN 978-0781765275.
- ↑ Srinivasan R, Arora RS (January 2005). "Do well infants born with an isolated single umbilical artery need investigation?". Arch. Dis. Child. 90 (1): 100–1. doi:10.1136/adc.2004.062372. PMC 1720078. PMID 15613529. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1720078/.
- ↑ Lilja M (July 1994). "Infants with single umbilical artery studied in a national registry. 3: A case control study of risk factors". Paediatr Perinat Epidemiol 8 (3): 325–33. PMID 7997408.
- ↑ URL: http://www.glowm.com/?p=glowm.cml/section_view&articleid=151. Accessed on: 8 January 2011.
- ↑ 15.0 15.1 Hasegawa J, Farina A, Nakamura M, et al. (December 2010). "Analysis of the ultrasonographic findings predictive of vasa previa". Prenat. Diagn. 30 (12-13): 1121–5. doi:10.1002/pd.2618. PMID 20872421.
- ↑ 16.0 16.1 Airas U, Heinonen S (April 2002). "Clinical significance of true umbilical knots: a population-based analysis". Am J Perinatol 19 (3): 127–32. doi:10.1055/s-2002-25311. PMID 12012287.
- ↑ 17.0 17.1 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 464. ISBN 978-0781765275.
- ↑ CS. 7 February 2011.
- ↑ 19.0 19.1 19.2 19.3 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 465. ISBN 978-0781765275.
- ↑ Khong TY (December 2010). "Evidence-based pathology: umbilical cord coiling". Pathology 42 (7): 618–22. doi:10.3109/00313025.2010.520309. PMID 21080869.
- ↑ PMID 16076615.
- ↑ URL: http://flylib.com/books/en/2.953.1.49/1/. Accessed on: 10 January 2011.
- ↑ URL: http://library.med.utah.edu/WebPath/PLACHTML/PLAC042.html. Accessed on: 12 January 2011.
- ↑ CS. 7 February 2011.
- ↑ ALS. 6 Febraury 2009.
- ↑ Miller PW, Coen RW, Benirschke K (October 1985). "Dating the time interval from meconium passage to birth". Obstet Gynecol 66 (4): 459–62. PMID 2413412.
- ↑ Funai EF, Labowsky AT, Drewes CE, Kliman HJ (January 2009). "Timing of fetal meconium absorption by amnionic macrophages". Am J Perinatol 26 (1): 93–7. doi:10.1055/s-0028-1103028. PMID 19031358.
- ↑ Povýsil C, Bennett R, Povýsilová V (January 2001). "CD 68 positivity of the so-called meconium corpuscles in human foetal intestine". Cesk Patol 37 (1): 7–9. PMID 11268705.
- ↑ Sienko A, Altshuler G (September 1999). "Meconium-induced umbilical vascular necrosis in abortuses and fetuses: a histopathologic study for cytokines". Obstet Gynecol 94 (3): 415?0. PMID 10472870.
- ↑ Sienko A, Altshuler G (September 1999). "Meconium-induced umbilical vascular necrosis in abortuses and fetuses: a histopathologic study for cytokines". Obstet Gynecol 94 (3): 415?0. PMID 10472870.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 463. ISBN 978-0781765275.
- ↑ CS. 7 February 2011.
- ↑ URL: http://flylib.com/books/en/2.953.1.49/1/. Accessed on: 10 January 2011.
- ↑ Tikkanen M, Nuutila M, Hiilesmaa V, Paavonen J, Ylikorkala O (2006). "Clinical presentation and risk factors of placental abruption". Acta Obstet Gynecol Scand 85 (6): 700–5. doi:10.1080/00016340500449915. PMID 16752262.
- ↑ CS. 7 February 2011.
- ↑ 36.0 36.1 Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 1106. ISBN 0-7216-0187-1.
- ↑ 37.0 37.1 37.2 37.3 37.4 37.5 Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Oberman, Harold A; Reuter, Victor E (2004). Sternberg's Diagnostic Surgical Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 2311. ISBN 978-0781740517.
- ↑ ALS. February 2009.
- ↑ 39.0 39.1 Redline RW (October 2007). "Villitis of unknown etiology: noninfectious chronic villitis in the placenta". Hum. Pathol. 38 (10): 1439–46. doi:10.1016/j.humpath.2007.05.025. PMID 17889674.
- ↑ CS. 7 February 2011.
- ↑ URL: http://jcp.bmj.com/content/61/12/1254.abstract. Accessed on: 11 January 2011.
- ↑ URL: http://www.flickr.com/photos/jian-hua_qiao_md/3954021698/. Accessed on: 11 January 2011.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 1109. ISBN 0-7216-0187-1.
- ↑ URL: http://path.upmc.edu/cases/case75/micro.html. Accessed on: 6 January 2011.
- ↑ 45.0 45.1 45.2 Sebire NJ, Backos M, Goldin RD, Regan L (May 2002). "Placental massive perivillous fibrin deposition associated with antiphospholipid antibody syndrome". BJOG 109 (5): 570–3. PMID 12066949. http://www3.interscience.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=1470-0328&date=2002&volume=109&issue=5&spage=570.
- ↑ Kraus FT, Acheen VI (July 1999). "Fetal thrombotic vasculopathy in the placenta: cerebral thrombi and infarcts, coagulopathies, and cerebral palsy". Hum. Pathol. 30 (7): 759–69. PMID 10414494.
- ↑ URL: http://jcp.bmj.com/content/61/12/1254.abstract. Accessed on: 12 January 2011.
- ↑ URL: http://gut.bmj.com/content/41/3/354.full. Accessed on: 12 January 2011.
- ↑ Stevens NG, Sander CH (October 1984). "Placental hemorrhagic endovasculitis: risk factors and impact on pregnancy outcome". Int J Gynaecol Obstet 22 (5): 393–7. PMID 6151926.
- ↑ Sander CM, Gilliland D, Akers C, McGrath A, Bismar TA, Swart-Hills LA (February 2002). "Livebirths with placental hemorrhagic endovasculitis: interlesional relationships and perinatal outcomes". Arch. Pathol. Lab. Med. 126 (2): 157–64. PMID 11825110.
- ↑ 51.0 51.1 Soma H, Yoshida K, Mukaida T, Tabuchi Y (1982). "Morphologic changes in the hypertensive placenta". Contrib Gynecol Obstet 9: 58–75. PMID 6754249.
- ↑ CS. 7 February 2011.
- ↑ 53.0 53.1 Roberts, DJ.; Post, MD. (Dec 2008). "The placenta in pre-eclampsia and intrauterine growth restriction.". J Clin Pathol 61 (12): 1254-60. doi:10.1136/jcp.2008.055236. PMID 18641412.
- ↑ AFIP - Placental Pathology. P.122. ISBN: 1-881041-89-1. 2004.
- ↑ Vinnars MT, Wijnaendts LC, Westgren M, Bolte AC, Papadogiannakis N, Nasiell J (May 2008). "Severe preeclampsia with and without HELLP differ with regard to placental pathology". Hypertension 51 (5): 1295–9. doi:10.1161/HYPERTENSIONAHA.107.104844. PMID 18362224.
- ↑ Ornstein MH, Rand JH (July 1994). "An association between refractory HELLP syndrome and antiphospholipid antibodies during pregnancy; a report of 2 cases". J. Rheumatol. 21 (7): 1360–4. PMID 7966086.
- ↑ Amer HZ, Heller DS (2010). "Chorangioma and related vascular lesions of the placenta--a review". Fetal Pediatr Pathol 29 (4): 199–206. doi:10.3109/15513815.2010.487009. PMID 20594143.
Recommended reading
- Langston C, Kaplan C, Macpherson T, et al. (May 1997). "Practice guideline for examination of the placenta: developed by the Placental Pathology Practice Guideline Development Task Force of the College of American Pathologists". Arch. Pathol. Lab. Med. 121 (5): 449–76. PMID 9167599.
- Baergen, Rebecca N. (2005). Manual of Benirschke and Kaufmann's Pathology of the Human Placenta (1st ed.). Springer. ISBN 978-0387220895.