Difference between revisions of "An introduction to gynecologic pathology"
| Line 182: | Line 182: | ||
DDx: | DDx: | ||
*Muellerian cyst - most common vaginal cyst. | |||
*[[Vaginal inclusion cyst]]. | |||
*[[Cervical adenocarcinoma]], not otherwise specified. | *[[Cervical adenocarcinoma]], not otherwise specified. | ||
*[[Minimal deviation adenocarcinoma of the uterine cervix]]. | *[[Minimal deviation adenocarcinoma of the uterine cervix]]. | ||
*[[Mesonephric adenocarcinoma]] - has cellular atypia. | *[[Mesonephric adenocarcinoma]] - has cellular atypia. | ||
*[[Wolffian duct hyperplasia]]. | *[[Wolffian duct hyperplasia]]. | ||
Images: | Images: | ||
Revision as of 11:44, 9 December 2013
Gynecologic pathology, informally gyne path, is a big part of surgical pathology. Radiologists have a lot of trouble in this area. On CT it is not infrequently hard to pick-out the ovaries... and it is a reason they don't comment on 'em. The ovary is affected by a huge number of tumours.
Site specific
Vulva
This covers the topic of vulva.
Vagina
This covers the topic of vagina.
Cervix
The most common type of cervical cancer is: squamous cell carcinoma.
Common benign cause of bleeding.
Gynecologic cytology is mostly cervical cytology and cervical cytology is the biggest part of cytology.
Ovary
The ovary has a wealth of pathology. It has benign tumours and malignant ones. The ovary article covers cysts of the ovary.
Uterine tube (Fallopian tube)
This was ignored in the past... current thinking is that it may be the real culprit in what is often labeled as "ovarian cancer".[1]
Uterus
The article covers uterine leiomyomas, uterine carcinosarcomas and endometrial stromal tumours.
Endometrium
Addresses dating of the endometrium.
Endometrial hyperplasia is considered the precursor of carcinoma.
A look at endometrial carcinoma.
Specific entities
Endometriosis
A common non-malignant affliction that causes infertility and morbidity.
Peritoneal inclusion cyst
This is dealt with in the omentum article. It is also known as benign multicystic mesothelioma[2] and inflammatory cyst of the peritoneum.
Endosalpingiosis
Female adnexal tumour of probable Wolffian origin
- Abbreviated FATWO.
- AKA Wolffian adnexal tumour.
Introduction to gynecologic tumours
Where to start when considering a malignant (epithelial) tumour of the gynecologic tract:
| Type | Histology | Differentiators | Associations | Typical age | Grade | IHC | Main DDx |
|---|---|---|---|---|---|---|---|
| Serous | cilia, columnar cells psammoma bodies, papillary arch. |
cilia, psammoma bodies | atrophy | usually 60s+ | typically high grade | p53+ diffuse, WT-1 +ve, D2-40 +ve, CA-125 +ve | poorly diff. endometrioid |
| Endometrioid | gland forming, endometrium-like | squamous metaplasia | endometriosis, endometrial hyperplasia | 40-60 | typically low grade | WT-1 -ve | serous |
| Mucinous | mucinous glands, colon-like | mucin, lack of necrosis | (?) | varies (?) | often low | metastatic tumour (usually GI) |
Benign stuff
Where to start when it looks benign:
| Entity | Morphology | Nucleus | Cytoplasm | Tumour | Other | Image |
|---|---|---|---|---|---|---|
| Hilus cells | well-defined cell borders, solid | eccentric, mild pleomorphism | eosinophilic | Hilus cell tumour | absent in childhood | Need one |
| Mesonephric remnant (AKA Wolffian duct) | cuboidal, glands/lumen present | ovoid, small | eosinophilic | FATWO, mesonephric adenocarcinoma | Develops into vas deferens in males. | mesonephric r., cat (uoguelph.ca) |
| Walthard cell rest | cuboidal, nested, solid | "coffee bean" shape | eosionphilic | Brenner tumour | nil | Coffee bean n. (WC), WCR (WC) |
Hilus cells
General
Features:[3]
- Present in embryo.
- Absent in childhood.
- Reappear at puberty.
- Common in post-menopausal women.
Associated pathology:
Microscopic
Features:[4]
- Similar to Leydig cells:
- Typically found in small clusters.
- Eosinophilic cytoplasm.
- Round nucleus +/- nucleolus.
Images:
Mesonephric duct remnant
- Gartner duct cyst, mesonephric duct cyst and Wolffian duct cyst redirect here.
General
Epidemiology:
- Embryological remnant - benign.
- Wolffian duct = precursor of male reproductive tract.[6]
Notes:
- This is not a finding that is reported. The importance of this finding is knowing it isn't something neoplastic.
- Lame way of remember the synonyms Gartner, Mesonephric, and Wolffian: GMW... it is trying to be a BMW but in girls.
Gross
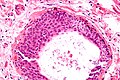
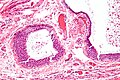
Microscopic
Features:[8]
- Small duct -- typically ~50-100 micrometres in diameter.
- Duct lined by cuboidal cells with moderate eosinophilic cytoplasm.
DDx:
- Muellerian cyst - most common vaginal cyst.
- Vaginal inclusion cyst.
- Cervical adenocarcinoma, not otherwise specified.
- Minimal deviation adenocarcinoma of the uterine cervix.
- Mesonephric adenocarcinoma - has cellular atypia.
- Wolffian duct hyperplasia.
Images:
- Mesonephric duct remnant - low mag. (webpathology.com).
- Mesonephric duct remnant - high mag. (webpathology.com).
IHC
Features:[9]
- CD10 +ve.
- CK7 +ve.
- PAX2 +ve (nuclear - strong & diffuse).[10]
- Cancers often lose staining.
Walthard cell rest
General
- AKA Walthard cell nest.
- Benign.
Epidemiology
- Thought to be related to Brenner tumour.
Microscopic
Features:[11]
- Collection of eosinophilic (i.e. pink) cuboidal cells; usually solid, may be cystic.
- Elliptical nucleus with single groove along major axis; "coffee bean" nucleus -- key feature.
Location:
- Usually in soft tissue of the uterine tube.
Images
WCR - very high mag.
WCR - high mag.

WCR - intermed. mag.

WCR - low mag.

WCR - very low mag.





Paraurethral cyst
Luteinized follicular cyst
General
- Benign.
Microscopic
Features:[12]
- Stratified cuboidal/columnar epithelium-like cells with:
- Small nuclei and small nucleoli.
- Cytoplasm may be eosinophilic.
- Sit on spindled cells (theca interna) that is luteinized.
Image
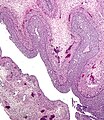
Luteinized follicular cyst. (WC/Nephron)

{kind=link}
{kind=link}
{kind=link}
Other
Pregnancy
Chorionic villi are the minimum needed to diagnose pregnancy histologically.
When reproduction goes wrong.
A big endocrine organ that gets completely ignored by almost everyone.
See also
References
- ↑ Hirst, JE.; Gard, GB.; McIllroy, K.; Nevell, D.; Field, M. (Jul 2009). "High rates of occult fallopian tube cancer diagnosed at prophylactic bilateral salpingo-oophorectomy.". Int J Gynecol Cancer 19 (5): 826-9. doi:10.1111/IGC.0b013e3181a1b5dc. PMID 19574767.
- ↑ Vallerie, AM.; Lerner, JP.; Wright, JD.; Baxi, LV. (May 2009). "Peritoneal inclusion cysts: a review.". Obstet Gynecol Surv 64 (5): 321-34. doi:10.1097/OGX.0b013e31819f93d4. PMID 19386139.
- ↑ Sternberg, Stephen S. (1997). Histology for Pathologists (2nd ed.). Lippincott Williams & Wilkins. pp. 953. ISBN 978-0397517183.
- ↑ URL: http://path.upmc.edu/cases/case394/dx.html. Accessed on: 16 January 2012.
- ↑ URL: http://webpathology.com/image.asp?n=3&Case=540. Accessed on: 22 October 2012.
- ↑ Hannema SE, Print CG, Charnock-Jones DS, Coleman N, Hughes IA (2006). "Changes in gene expression during Wolffian duct development". Horm. Res. 65 (4): 200–9. doi:10.1159/000092408. PMID 16567946.
- ↑ Nucci, Marisa R.; Oliva, Esther (2009). Gynecologic Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 97. ISBN 978-0443069208.
- ↑ Sternberg SE. Histology for Pathologists. 2nd Ed. P.893.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 442. ISBN 978-0781765275.
- ↑ Rabban, JT.; McAlhany, S.; Lerwill, MF.; Grenert, JP.; Zaloudek, CJ. (Feb 2010). "PAX2 distinguishes benign mesonephric and mullerian glandular lesions of the cervix from endocervical adenocarcinoma, including minimal deviation adenocarcinoma.". Am J Surg Pathol 34 (2): 137-46. doi:10.1097/PAS.0b013e3181c89c98. PMID 20061933.
- ↑ Nucci, Marisa R.; Oliva, Esther (2009). Gynecologic Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 332. ISBN 978-0443069208.
- ↑ URL: http://www.med-ed.virginia.edu/courses/path/gyn/ovary2.cfm. Accessed on: 20 May 2010.