Vascular disease
The article covers vascular disease, i.e. diseases of blood vessels. These keep vascular surgeons and cardiac surgeon busy.
Vasculitides are covered in a separate article called vasculitides.
Normal blood vessels
Comparing arteries and veins:[1]
| Feature | Artery | Vein |
|---|---|---|
| Internal elastic lamina | prominent/thick, usu. complete | thin & incomplete |
| External elastic lamina | present, thick | absent |
| Shape | circular / lumen wide open | collapsed |
| Wall thickness | thick | thin |
Great vessels
When things go wrong here, you see a cardiac surgeon.
Atherosclerosis
General
- A leading cause of death, esp. in the Western world.
- May have multi-system manifestations.
Location and associated pathology:
- Coronary artery atherosclerosis (AKA coronary artery disease) -> myocardial infarction +/-coronary thrombosis.
- Atherosclerotic peripheral vascular disease -> leg amputations.
- Carotid artery atherosclerosis -> thrombotic stroke.
- Superior mesenteric artery atherosclerosis -> ischemic enteritis or ischemic colitis or ischemic enterocolitis.
- Penile artery atherosclerosis -> impotence.
Clinical risk factors:
- Age.
- Blood pressure (high) - modifiable (antihypertensives).
- Cholesterol - modifiable (statins, diet).
- Diabetes mellitus - modifiable (hypoglycemic medications, diet, lifestyle).
- Smoking - modifiable (cessation).
- Family history.
Microscopic
Features:
- Intimal hyperplasia.
- Lipid deposition.
- Foamy macrophages within intima & media.
- Cholesterol clefts
- Luminal narrowing.
Notes:
- Considered "complex" if any of the following are present:[2]
- Calcifications.
- Thrombosis.
- Haemorrhage.
Image
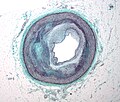
Right coronary artery with atherosclerosis. (WC/Nephron)

Stains
- Elastic trichrome stain or Movat stain - highlights duplication of internal elastic lamina, allows on to identify with ease intimal thickening.
Aortic dissection
- Abbreviated AoD.
General
Risk factors:
- Hypertension.[3]
- Atherosclerosis.[4]
- Cardiac surgery - rare, well-known complication.[5]
Note:
- Diabetes uncommon in AoD.[4]
Associations
Heritable:[6]
- Marfan's syndrome.
- Loeys-Dietz syndrome - a Marfan-like syndrome[7]
- Ehlers-Danlos syndrome.
- Bicuspid aortic valve.[4]
Others:
- Tertiary syphilis.[8]
- Turner syndrome.[9]
Classification
Two classification exist:
- DeBakey.
- Stanford.
Stanford dissection classification:[10]
- Type A - aortic root to the left subclavian artery.
- Considered a surgical emergency.
- Type B - distal to (left) subclavian artery.
- Generally, treated conservatively.
Gross
- Entry intimal tear +/- exit intimal tear.
- Blood between layers of the vessel wall.
Images

Aortic dissection. (WC)

www:
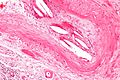
Microscopic
Images

Aortic dissection. Victoria blue-H&E. (WC/KGH)
_Victoria_blue-HE.jpg)
www:
Cystic medial degeneration
General
- Nonspecific finding - may be seen in a number of conditions.
Note about cystic medial necrosis:
- Often not cystic and not necrotic.
Microscopic
- Basophilic ground substance in the media (seen on Movat's stain).
- Disruption of the elastic lamina (seen on elastic trichrome stain).
- +/-Focal necrosis.
Images

Cystic medial degeneration - low mag. (WC/Nephron)

Cystic medial degeneration - high mag. (WC/Nephron)

Cystic medial degeneration - movat - low mag. (WC/Nephron)

Cystic medial degeneration - movat - intermed. mag. (WC/Nephron)




www:
Stains
- Elastin stains (e.g. elastic trichrome stain) - disruption of the elastic lamina.
- Movat's stain - basophilic ground substance in the media.
Medial calcific sclerosis
- AKA Moenckeberg medial calcific sclerosis, calcific medial sclerosis of Monckeberg, and Monckeberg's arteriosclerosis.
General
- Usually of no clinical consequence.
Microscopic
Features:[14]
- Medial calcification (purple irregular stuff on H&E -- calcium phosphate).
Note:
- Lumen unaffected.
Images
www:
Hyperplastic arteriolosclerosis
General
- Associated with:[15]
- Malignant hypertension.
- Scleroderma.
- May be a consequence of thrombotic microangiopathy.[citation needed]
Note:
- Hyperplasia = proliferation of cells.
Microscopic
Features:[14]
- Onion-skin appearance of intima & media due to:
- Intimal hyperplasia.
- Smooth muscle hyperplasia.
Fibromuscular dysplasia
- Abbreviated FMD.
General
Etiology:
- Unknown, possibly genetic.
Gender:
- Women > men.
- May be seen in virtually any artery.
- Reported as a cause of sudden death with involvement of the artery supplying the AV node.[16]
Gross/radiologic
- Segmental - thinning and thickening.[17]
Classical locations:[17]
- Renal artery - leading to hypertension.
- Carotid artery.
Microscopic
Features:[17]
- Smooth muscle hyperplasia - key feature.
- Elastic fibre fragmentation.
- Luminal narrowing.
Images:
Stains
- Elastic trichrome or Movat stain - to demonstrate elastic fibre fragmentation.
Thromboangiitis obliterans
- AKA Buerger disease.
- Should not be confused with Berger disease (IgA nephropathy).
General
Typical symptoms/signs - progression:[20]
- Intermittent claudication -> ulcers -> gangrene -> amputation.
Treatment:
- Stop smoking.[20]
Gross
- Afflicts small and medium-sized vessels of the extremities.
- Corkscrew vessels - seen on angiography.[19]
Microscopic
Features:[21]
- Acute inflammation:
- Endarteritis - neutrophils at the internal elastic lamina (IEL).
- Periarteritis - neutrophils around the arteries.
- Obliteration of the lumen - intimal thickening.
Notes:
- Typically segmental.[20]
DDx:
- Peripheral vascular disease (atherosclerosis) - typically lacks the acute inflammation around the IEL and around the vessels.
- Vasculitis - have fibrinoid necrosis.
Sign out
MIDDLE FINGER DISTAL PHALYNX, LEFT, AMPUTATION: - GANGRENE WITH ENDARTERITIS, PERIARTERITIS AND LUMINAL OBLITERATION/NARROWING CONSISTENT WITH THROMOANGITIS OBLITERANS (BUERGER'S DISEASE).
Thrombosis
- See also: Cerebral venous thrombosis.
General
Definition:
- Blood clot formation within a vessel.
Complications:
- Embolism - see: Pulmonary thromboembolism.
Risk factors:
- The classic pimping question is what "Virchow's triad?"
- Stasis, hypercoagulability, endothelial injury.
- A long list is found in: risk factors for VTE.
Gross
Microscopic
Features:
- Lines of Zahn.
- Fibrin - pink acellular stuff on a H&E stain.
Image

Intravascular fibrin - high mag. (WC/Nephron)

Cholesterol embolism
- Abbreviated CE.
General
- Strong association with atherosclerosis - found in ~3% of individuals in an autopsy series of 267 older individuals (mean age ~65 years).[22]
- Significant CEs are often iatrogenic.
- Known complication of coronary catherization (incidence ~ 1%).[23]
- May complicate any vascular surgery, CABG.
Microscopic
Features:[24]
- Intravascular cholesterol clefts (biconvex white spaces) - key feature.
- Typically ~ 100-500 micrometers (long axis) x 50-100 micrometers (short axis). (?)
- +/-Macrophages and giant cells.
- +/-Eosinophils.
Note:
- May be associated with ischemic changes and necrosis.
- Usually in the context of severe atherosclerosis.
Note (trivia):
- Cholesterol crystals dissolve with routine processing (paraffin embedding); this is why one talks of "cholesterol clefts".
Images

Cholesterol embolus - intermed. mag. (WC)
Cholesterol embolus - high mag. (WC)


Coarctation of the aorta
- AKA aortic coarctation.
General
- Uncommon.
Classification:
- Preductal.
- Postductal.
Associations:
Clinical
Presentation:[27]
- Heart failure.
- Hypertension - esp. upper extremity vs. lower extremity.
Gross
- Narrowing (stenosis) of the aorta proximal or distal to the ductus arteriosis.
Image
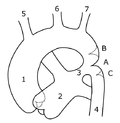
Pre- and postductal coarctation of the aorta - schematic (WC)

Intracranial berry aneurysm
See also
References
- ↑ URL: http://www.lab.anhb.uwa.edu.au/mb140/corepages/vascular/vascular.htm. Accessed on: 13 January 2011.
- ↑ Klatt, Edward C. (2006). Robbins and Cotran Atlas of Pathology (1st ed.). Saunders. pp. 4. ISBN 978-1416002741.
- ↑ Braverman, AC. (Oct 2011). "Aortic dissection: prompt diagnosis and emergency treatment are critical.". Cleve Clin J Med 78 (10): 685-96. doi:10.3949/ccjm.78a.11053. PMID 21968475.
- ↑ 4.0 4.1 4.2 LeMaire, SA.; Russell, L. (Feb 2011). "Epidemiology of thoracic aortic dissection.". Nat Rev Cardiol 8 (2): 103-13. doi:10.1038/nrcardio.2010.187. PMID 21173794.
- ↑ Leontyev, S.; Borger, MA.; Legare, JF.; Merk, D.; Hahn, J.; Seeburger, J.; Lehmann, S.; Mohr, FW. (Mar 2012). "Iatrogenic type A aortic dissection during cardiac procedures: early and late outcome in 48 patients.". Eur J Cardiothorac Surg 41 (3): 641-6. doi:10.1093/ejcts/ezr070. PMID 22345184.
- ↑ Gleason TG (2005). "Heritable disorders predisposing to aortic dissection". Semin. Thorac. Cardiovasc. Surg. 17 (3): 274-81. doi:10.1053/j.semtcvs.2005.06.001. PMID 16253833.
- ↑ Loeys BL, Schwarze U, Holm T, et al (August 2006). "Aneurysm syndromes caused by mutations in the TGF-beta receptor". N. Engl. J. Med. 355 (8): 788-98. doi:10.1056/NEJMoa055695. PMID 16928994. http://content.nejm.org/cgi/content/full/355/8/788.
- ↑ Cruz, RP.; Marrone, LC.; Marrone, AC. (Nov 2010). "Chronic syphilitic aortic aneurysm complicated with chronic aortic dissection.". Am J Surg 200 (5): e64-6. doi:10.1016/j.amjsurg.2010.02.017. PMID 20864080.
- ↑ Carlson, M.; Silberbach, M. (2009). "Dissection of the aorta in Turner syndrome: two cases and review of 85 cases in the literature.". BMJ Case Rep 2009: bcr0620091998. doi:10.1136/bcr.06.2009.1998. PMID 21731587.
- ↑ Finkelmeier BA (September 1997). "Dissection of the aorta: a clinical update". J Vasc Nurs 15 (3): 88-93. PMID 9362838.
- ↑ URL: http://emedicine.medscape.com/article/756835-overview. Accessed on: 12 August 2010.
- ↑ URL: http://emedicine.medscape.com/article/756835-overview. Accessed on: 12 August 2010.
- ↑ Ha HI, Seo JB, Lee SH, et al. (2007). "Imaging of Marfan syndrome: multisystemic manifestations". Radiographics 27 (4): 989–1004. doi:10.1148/rg.274065171. PMID 17620463. http://radiographics.rsna.org/content/27/4/989.full.
- ↑ 14.0 14.1 Klatt, Edward C. (2006). Robbins and Cotran Atlas of Pathology (1st ed.). Saunders. pp. 7. ISBN 978-1416002741.
- ↑ URL: http://library.med.utah.edu/WebPath/IMMHTML/IMM028.html. Accessed on: 11 May 2011.
- ↑ 16.0 16.1 Lee, S.; Chae, J.; Cho, Y. (Dec 2006). "Causes of sudden death related to sexual activity: results of a medicolegal postmortem study from 2001 to 2005.". J Korean Med Sci 21 (6): 995-9. PMID 17179675.
- ↑ 17.0 17.1 17.2 Hata, D. (Sep 2001). "Fibromuscular dysplasia.". Intern Med 40 (9): 978-9. PMID 11579971.
- ↑ Highlander, P.; Southerland, CC.; VonHerbulis, E.; Gonzalez, A. (Jan 2011). "Buerger disease (thromboangiitis obliterans): a clinical diagnosis.". Adv Skin Wound Care 24 (1): 15-7. doi:10.1097/01.ASW.0000392923.37852.43. PMID 21173586.
- ↑ 19.0 19.1 Fujii, Y.; Soga, J.; Nakamura, S.; Hidaka, T.; Hata, T.; Idei, N.; Fujimura, N.; Nishioka, K. et al. (Aug 2010). "Classification of corkscrew collaterals in thromboangiitis obliterans (Buerger's disease): relationship between corkscrew type and prevalence of ischemic ulcers.". Circ J 74 (8): 1684-8. PMID 20534945.
- ↑ 20.0 20.1 20.2 Dargon, PT.; Landry, GJ. (Aug 2012). "Buerger's disease.". Ann Vasc Surg 26 (6): 871-80. doi:10.1016/j.avsg.2011.11.005. PMID 22284771.
- ↑ Kurata, A.; Schulz, A.; Franke, FE. (2004). "Reappraisal of thromboangiitis obliterans--a pathological contribution.". Verh Dtsch Ges Pathol 88: 231-6. PMID 16892557.
- ↑ Flory CM (1945). "Arterial occlusions produced by emboli from eroded aortic atheromatous plaques". Am J Pathol 21 (3): 549–565. PMC 1934118. PMID 19970827. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1934118/.
- ↑ Fukumoto Y, Tsutsui H, Tsuchihashi M, Masumoto A, Takeshita A (July 2003). "The incidence and risk factors of cholesterol embolization syndrome, a complication of cardiac catheterization: a prospective study". J. Am. Coll. Cardiol. 42 (2): 211–6. doi:10.1016/S0735-1097(03)00579-5. PMID 12875753. http://linkinghub.elsevier.com/retrieve/pii/S0735109703005795.
- ↑ Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Reuter, Victor E; Stoler, Mark H (2009). Sternberg's Diagnostic Surgical Pathology (5th ed.). Lippincott Williams & Wilkins. pp. 1735-6. ISBN 978-0781779425.
- ↑ Braverman, AC.; Güven, H.; Beardslee, MA.; Makan, M.; Kates, AM.; Moon, MR. (Sep 2005). "The bicuspid aortic valve.". Curr Probl Cardiol 30 (9): 470-522. doi:10.1016/j.cpcardiol.2005.06.002. PMID 16129122.
- ↑ Hjerrild, BE.; Mortensen, KH.; Sørensen, KE.; Pedersen, EM.; Andersen, NH.; Lundorf, E.; Hansen, KW.; Hørlyck, A. et al. (2010). "Thoracic aortopathy in Turner syndrome and the influence of bicuspid aortic valves and blood pressure: a CMR study.". J Cardiovasc Magn Reson 12: 12. doi:10.1186/1532-429X-12-12. PMID 20222980.
- ↑ Peres, A.; Martins, JD.; Paramés, F.; Gil, R.; Matias, C.; Franco, J.; Freitas, I.; Trigo, C. et al. (Jan 2010). "Isolated aortic coarctation: experience in 100 consecutive patients.". Rev Port Cardiol 29 (1): 23-35. PMID 20391897.