Difference between revisions of "Head and neck cytopathology"
m (→Mucoepidermoid carcinoma: link to main) |
(+image) |
||
| (50 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
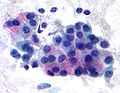
[[Image:Pleomorphic adenoma - cytology -- high mag.jpg|right|thumb|[[Micrograph]] showing a pleomorphic adenoma. [[Pap stain]].]] | |||
'''Head and neck cytopathology''' is a small part of cytopathology. Non-cytopathology head & neck pathology is dealt with in the ''[[head and neck pathology]]'' article. | '''Head and neck cytopathology''' is a small part of cytopathology. Non-cytopathology head & neck pathology is dealt with in the ''[[head and neck pathology]]'' article. | ||
Thyroid cytopathology is dealt with in the ''[[thyroid cytopathology]]'' article. An introduction to cytopathology is in the ''[[cytopathology]]'' article. | Thyroid cytopathology is dealt with in the ''[[thyroid cytopathology]]'' article. An introduction to cytopathology is in the ''[[cytopathology]]'' article. | ||
==Normal | ''Salivary gland cytopathology'' and ''salivary gland cytology'' redirect to here. | ||
=Proposed Milan system for reporting salivary gland cytopathology= | |||
:''Milan system'' and ''Milan classification'' redirect here. | |||
{| class="wikitable" | |||
|- | |||
! Category | |||
! Typical management | |||
! Comments | |||
|- | |||
| Nondiagnostic | |||
| repeat FNA | |||
| | |||
|- | |||
| Nonneoplastic | |||
| follow-up/discharge | |||
| | |||
|- | |||
| Atypia of undetermined significance (AUS) | |||
| repeat FNA | |||
| use should be minimized <br>- like [[FLUS]] and [[ASCUS]] | |||
|- | |||
| Neoplasm | |||
| excision | |||
| subdivided into: (a) benign (b) salivary gland neoplasm of uncertain malignant potential (SUMP) | |||
|- | |||
| Suspicious for malignancy | |||
| wide excision +/-lymph nodes (?) | |||
| | |||
|- | |||
| Malignant | |||
| wide excision & lymph nodes (?) | |||
| | |||
|} | |||
Notes: | |||
*This classification is still evolving.<ref>URL: [http://www.cytopathology.org/the-milan-system-for-reporting-salivary-gland-cytopathology/ http://www.cytopathology.org/the-milan-system-for-reporting-salivary-gland-cytopathology/]. Accessed on: 31 March 2016.</ref> The preliminary version (above) was presented by Dr. William Faquin at [[USCAP]] 2016 in Seattle.<ref>URL: [http://www.uscap.org/meetings/detail/2016-annual-meeting/sessions/2334 http://www.uscap.org/meetings/detail/2016-annual-meeting/sessions/2334]. Accessed on: 13 March 2016.</ref> | |||
*The goal is to complete the reporting system by the summer of 2017. | |||
=Normal= | |||
Depends on the structure that is needled. | Depends on the structure that is needled. | ||
| Line 12: | Line 51: | ||
*Nucleus: | *Nucleus: | ||
**Dispersed chromatin. | **Dispersed chromatin. | ||
**Indistinct nucleolus. | **Indistinct [[nucleolus]]. | ||
*Low NC ratio cells. | *Low [[NC ratio]] cells. | ||
Sticky lymphoid tissue: | Sticky lymphoid tissue: | ||
*Irregular globs of tissue with small cells. | *Irregular globs of tissue with small cells. | ||
==Salivary gland tumours - summary | [[Skeletal muscle]]: | ||
*Round red staining globs +/-apparent striations. | |||
*Nuclei more at edges (peripheral). | |||
===Images=== | |||
<gallery> | |||
Image: Skeletal muscle - FNA 1 - intermed mag.jpg | SM - intermed. mag. | |||
Image: Skeletal muscle - FNA 1a- high mag.jpg | SM - high mag. | |||
Image: Skeletal muscle - FNA 1a- very high mag.jpg | SM - very high mag. | |||
Image: Skeletal muscle - FNA 1b- very high mag.jpg | SM - very high mag. | |||
Image: Skeletal muscle - FNA 2a- high mag.jpg | SM - high mag. | |||
Image: Skeletal muscle - FNA 2b- high mag.jpg | SM - high mag. | |||
Image: Skeletal muscle - FNA 2a- very high mag.jpg | SM - very high mag. | |||
Image: Skeletal muscle - FNA 2b- very high mag.jpg | SM - very high mag. | |||
</gallery> | |||
=Salivary gland tumours - summary= | |||
===Benign=== | ===Benign=== | ||
{| class="wikitable" | {| class="wikitable" | ||
| Line 30: | Line 86: | ||
! Image | ! Image | ||
|- | |- | ||
| Pleomorphic adenoma | | [[Pleomorphic adenoma]] | ||
| '''Fluffy fibromyxoid material & cells''' and single (plasmacytoid-like) '''myoepithelial cells''' | | '''Fluffy fibromyxoid material & cells''' and single (plasmacytoid-like) '''myoepithelial cells''' | ||
| ? | | ? | ||
| Line 36: | Line 92: | ||
| DDx (?) | | DDx (?) | ||
| ? | | ? | ||
| [ | | [[Image:Pleomorphic_adenoma_-_cytology.jpg | thumb| center| 150px| Pleomorphic adenoma. (WC)]] | ||
|- | |- | ||
| Warthin tumour (papillary cystadenoma lymphomatosum) | | [[Warthin tumour]] (papillary cystadenoma lymphomatosum) | ||
| Sheets of uniformly spaced '''oncocytes''', lymphocytes, necrotic debris | | Sheets of uniformly spaced '''oncocytes''', lymphocytes, necrotic debris | ||
| Oncocytes (abundant, granular, eosinophilic tinge), well-defined cell borders | | Oncocytes (abundant, granular, eosinophilic tinge), well-defined cell borders | ||
| Line 44: | Line 100: | ||
| Acinic cell carcinoma (AcCC), oncocytoma | | Acinic cell carcinoma (AcCC), oncocytoma | ||
| AcCC: irregular spaced cells, lack well-defined cell borders | | AcCC: irregular spaced cells, lack well-defined cell borders | ||
| [ | | [[Image:Papillary_cystadenoma_lymphomatosum_cytology_high.jpg | thumb| center| 150px| Warthin tumour - high mag. (WC)]] | ||
|- | |- | ||
|} | |} | ||
| Line 59: | Line 115: | ||
! Image | ! Image | ||
|- | |- | ||
| Mucoepidermoid carcinoma | | [[Mucoepidermoid carcinoma]] | ||
| Clumps of cells | | Clumps of cells | ||
| '''Abundant whispy cytoplasm''' | | '''Abundant whispy cytoplasm''' | ||
| Line 65: | Line 121: | ||
| Mucocele ? | | Mucocele ? | ||
| Nuclear atypia | | Nuclear atypia | ||
| [ | | [[Image:Mucoepidermoid_carcinoma_2_-_high_mag.jpg | thumb| center| 150px| Mucoepidermoid carcinoma. (WC)]] | ||
|- | |- | ||
| Acinic cell carcinoma (AcCC) | | [[Adenoid cystic carcinoma]] (AdCC) | ||
| '''Circular islands of abundant very small cells''' | |||
| Scant cytoplasm | |||
| Small nucleus - may have carrot shape | |||
| AcCC | |||
| Basement membrane material - PAS-D+ve<ref name=pmid62333>{{cite journal |author=Chen SY |title=Adenoid cystic carcinoma of minor salivary gland. Histochemical and electron microscopic studies of cystlike space |journal=Oral Surg. Oral Med. Oral Pathol. |volume=42 |issue=5 |pages=606–19 |year=1976 |month=November |pmid=62333 |doi= |url=}}</ref> | |||
| [[Image:Adenoid_cystic_carcinoma_cytology.jpg | thumb| center| 150px| Adenoid cystic carcinoma. (WC)]] | |||
|- | |||
| [[Acinic cell carcinoma]] (AcCC) | |||
| '''3-D clusters of small cells''' | | '''3-D clusters of small cells''' | ||
| Abundant orangeophilic granular cytoplasm | | Abundant orangeophilic granular cytoplasm | ||
| Line 73: | Line 137: | ||
| Warthin tumour | | Warthin tumour | ||
| AcCC missing lymphocytic background; irreg. spacing of cells | | AcCC missing lymphocytic background; irreg. spacing of cells | ||
| [ | | [[Image:Acinic_cell_carcinoma.jpg | thumb| center| 150px| Acinic cell carcinoma. (WC)]] | ||
| | |||
| | |||
| | |||
| | |||
|} | |} | ||
=Salivary gland= | |||
{{Main|Salivary gland}} | |||
==Sialoadenitis== | |||
{{main|Chronic sialadenitis}} | |||
===Cytology=== | |||
Features: | |||
*Inflammatory cells - lymphocytes, plasma cells - '''key features'''. | |||
*+/-Squamous metaplasia. | |||
*+/-Necrotic debris. | |||
*Benign ductal epithelium. | |||
DDx: | |||
*Squamous carcinoma. | |||
*Mucoepidermoid carcinoma. | |||
==Crystals in salivary gland specimens== | |||
===General=== | |||
*Uncommon in general. | |||
**Typical location is: parotid (>85% salivary gland specimens with crystals<ref name=pmid33296146>{{cite journal |authors=Sun T, Faquin WC, Torous VF |title=Crystalloids in FNA specimens of salivary gland lesions: A retrospective study in a single large institute |journal=Cancer Cytopathol |volume=129 |issue=6 |pages=432–438 |date=June 2021 |pmid=33296146 |doi=10.1002/cncy.22395 |url=}}</ref>). | |||
*May be seen in the context of any diagnostic category (non-diagnostic, benign, neoplastic, malignant). | |||
**Approximately 40% of cases with crystals are benign or non-diagnositic.<ref name=pmid33296146/> | |||
**Approximately 10% of cases with crystals are suspicious or malignant.<ref name=pmid33296146/> | |||
DDx: | |||
*Amylase crystalloids ~ 75%. | |||
*Tyrosine crystalloids ~ 11%. | |||
*Collagenous crystalloids ~ 3%. | |||
*Undetermined type ~ 11%. | |||
===Cytology=== | |||
Features:<ref name=pmid33296146/><ref>{{cite journal |authors=Kishore M, Kaushal M, Dogra S |title=Crystalloids in salivary gland lesion: A diagnostic clue |journal=J Lab Physicians |volume=11 |issue=1 |pages=100–101 |date=2019 |pmid=30983813 |pmc=6437830 |doi=10.4103/JLP.JLP_120_18 |url=}}</ref> | |||
*Amylase crystalloids: rhomboid (or polygonal) +/- "pointy" ends, nonbirefringent. | |||
*Tyrosine crystalloids: floret-like structures, refractile. | |||
*Collagenous crystalloids: needle-shaped, radially arranged. | |||
====Images==== | |||
<gallery> | |||
Image: Amylase crystals - parotid -- intermed mag.jpg | Amylase crystals - parotid - intermed. mag. | |||
Image: Amylase crystals - parotid - alt -- intermed mag.jpg | Amylase crystals - parotid - intermed. mag. | |||
Image: Amylase crystals - parotid -- high mag.jpg | Amylase crystals - parotid - high mag. | |||
Image: Amylase crystals - parotid - alt -- high mag.jpg | Amylase crystals - parotid - high mag. | |||
Image: Amylase crystals - parotid -- very high mag.jpg | Amylase crystals - parotid - very high mag. | |||
Image: Amylase crystals - parotid - alt -- very high mag.jpg | Amylase crystals - parotid - very high mag. | |||
Image: Amylase crystals - parotid - alt2 -- very high mag.jpg | Amylase crystals - parotid - very high mag. | |||
Image: Amylase crystals - parotid -- high mag.gif | Amylase crystals - parotid - animation - high mag. | |||
Image: Amylase crystals - parotid -- very high mag.gif | Amylase crystals - parotid - animation - very high mag. | |||
</gallery> | |||
===Sign out=== | |||
<pre> | |||
Crystalloid material is present and has a rhomboid/polygonal shape with occasional "pointy" ends; this is in keeping with amylase crystals. | |||
</pre> | |||
==Pleomorphic adenoma== | ==Pleomorphic adenoma== | ||
General | {{Main|Pleomorphic adenoma}} | ||
*Abbreviated ''PA''. | |||
===General=== | |||
*Common benign tumour. | *Common benign tumour. | ||
===Cytology=== | ===Cytology=== | ||
| Line 97: | Line 209: | ||
#Chondromyxoid stroma. | #Chondromyxoid stroma. | ||
#*Whispy/fluffy groups of spindle cells that overlap (fibromyxoid tissue) - blue-ish. | #*Whispy/fluffy groups of spindle cells that overlap (fibromyxoid tissue) - blue-ish. | ||
DDx: | DDx: | ||
*Adenoid cystic carcinoma. | *[[Adenoid cystic carcinoma]]. | ||
**Big circular globs (cysts) - common in AdCC. | **Big circular globs (cysts) - common in AdCC. | ||
====Images==== | |||
<gallery> | |||
Image: Pleomorphic adenoma - cytology -- high mag.jpg | PA - high mag. (WC) | |||
Image: Pleomorphic adenoma - cytology - alt -- high mag.jpg | PA - high mag. (WC) | |||
Image: Pleomorphic adenoma - cytology -- very high mag.jpg | PA - very high mag. (WC) | |||
Image: Pleomorphic adenoma - cytology - alt -- very high mag.jpg | PA - very high mag. (WC) | |||
</gallery> | |||
<gallery> | |||
Image:Pleomorphic_adenoma_-_cytology.jpg | Pleomorphic adenoma. (WC) | |||
</gallery> | |||
==Warthin tumour== | ==Warthin tumour== | ||
*AKA ''papillary cystadenoma lymphomatosum''. | *AKA ''papillary cystadenoma lymphomatosum''. | ||
===General=== | |||
*Usual smokers. | |||
*May be bilateral. | |||
=== | ===Cytology=== | ||
Features:<ref>[http://sciencelinks.jp/j-east/article/200123/000020012301A0753392.php http://sciencelinks.jp/j-east/article/200123/000020012301A0753392.php]</ref> | Features:<ref>[http://sciencelinks.jp/j-east/article/200123/000020012301A0753392.php http://sciencelinks.jp/j-east/article/200123/000020012301A0753392.php]</ref> | ||
*Oncocytes. | *Oncocytes. | ||
| Line 114: | Line 236: | ||
***Granular cytoplasm. | ***Granular cytoplasm. | ||
***Nucleoli. | ***Nucleoli. | ||
**Oncocytes are often associated with ''mast | **Oncocytes are often associated with ''[[mast cell]]s'', i.e. on "top of" oncocytes. | ||
***Mast cells: very granular dark staining cytoplasm (on smears). | ***Mast cells: very granular dark staining cytoplasm (on smears). | ||
*Lymphocytes. | *Lymphocytes. | ||
*Necrotic material (cyst contents). | *Necrotic material (cyst contents). | ||
DDx: | DDx: | ||
*Acinic cell carcinoma. | *[[Acinic cell carcinoma]]. | ||
**Spacing of tumour in AcCC is more irregular and appear more crowded. | **Spacing of tumour in AcCC is more irregular and appear more crowded. | ||
**The cell borders in AcCC is less obvious. | **The cell borders in AcCC is less obvious. | ||
*Oncocytoma | *Oncocytoma. | ||
**Oncocytoma (vis-a-vis Warthin tumour) has more '''c'''ells, more '''c'''ytoplasm, more granularity of '''c'''ytoplasm, more '''c'''omplex architecture.<ref name=boerner2003/> | **Oncocytoma (vis-a-vis [[Warthin tumour]]) has more '''c'''ells, more '''c'''ytoplasm, more granularity of '''c'''ytoplasm, more '''c'''omplex architecture.<ref name=boerner2003/> | ||
====Images==== | |||
<gallery> | |||
Image:Papillary_cystadenoma_lymphomatosum_cytology_high.jpg | Warthin tumour - high mag. (WC) | |||
Image:Papillary_cystadenoma_lymphomatosum_cytology_intermed.jpg | Warthin tumour - intermed. mag. (WC) | |||
Image:Papillary_cystadenoma_lymphomatosum2.jpg | Warthin tumour - surgical specimen. (WC) | |||
</gallery> | |||
==Oncocytoma== | ==Oncocytoma== | ||
*May be confused with Warthin tumour. | {{Main|Oncocytoma of the salivary gland}} | ||
===General=== | |||
*May be confused with [[Warthin tumour]]. | |||
===Cytology=== | |||
Features: | Features: | ||
*Oncocytes. | *Oncocytes. | ||
| Line 149: | Line 276: | ||
==Mucoepidermoid carcinoma== | ==Mucoepidermoid carcinoma== | ||
{{Main|Mucoepidermoid carcinoma}} | {{Main|Mucoepidermoid carcinoma}} | ||
===General=== | |||
*A challenging FNA diagnosis.<ref name=pmid2296840>{{Cite journal | last1 = Cohen | first1 = MB. | last2 = Fisher | first2 = PE. | last3 = Holly | first3 = EA. | last4 = Ljung | first4 = BM. | last5 = Löwhagen | first5 = T. | last6 = Bottles | first6 = K. | title = Fine needle aspiration biopsy diagnosis of mucoepidermoid carcinoma. Statistical analysis. | journal = Acta Cytol | volume = 34 | issue = 1 | pages = 43-9 | month = | year = | doi = | PMID = 2296840 }}</ref> | |||
===Cytology=== | |||
Features: | Features: | ||
*Sheets of cells. | *Sheets of cells. | ||
| Line 156: | Line 288: | ||
**Cell borders are often distinct. | **Cell borders are often distinct. | ||
DDx: | |||
*[ | *[[Squamous cell carcinoma]] - extensive keratinization and squamous pearls.<ref name=Ref_FNAC25>{{Ref FNAC|25}}</ref> | ||
===Images=== | |||
<gallery> | |||
Image:Mucoepidermoid_carcinoma_2_-_high_mag.jpg | Mucoepidermoid carcinoma. (WC) | |||
Image:Mucoepidermoid_carcinoma_2_-_very_high_mag.jpg | Mucoepidermoid carcinoma - very high mag. (WC) | |||
</gallery> | |||
==Acinic cell carcinoma== | ==Acinic cell carcinoma== | ||
{{Main|Acinic cell carcinoma}} | |||
===General=== | |||
*Uncommon. | |||
===Cytology=== | |||
Features:<ref>SB. 12 January 2010.</ref> | Features:<ref>SB. 12 January 2010.</ref> | ||
*Abundant granular cytoplasm. | *Abundant granular cytoplasm. | ||
| Line 173: | Line 314: | ||
**Ductal structures (differentiates from normal). | **Ductal structures (differentiates from normal). | ||
Memory device: | |||
*[ | *AcCC - lots of "C"s: lots of cytoplasm, [[carcinoid]]-like (stippled chromatin, granular cytoplasm). | ||
====Image==== | |||
<gallery> | |||
Image:Acinic_cell_carcinoma.jpg | Acinic cell carcinoma - cytology. (WC) | |||
</gallery> | |||
==Adenoid cystic carcinoma== | ==Adenoid cystic carcinoma== | ||
===General=== | |||
*Usu. distinctive. | |||
*May be painful due the presence of [[perineural invasion]]. | |||
===Cytology=== | |||
Features: | Features: | ||
*Solid circular islands that are well-circumscribed. | *Solid circular islands that are well-circumscribed. | ||
| Line 194: | Line 342: | ||
*Memory device: A'''d'''CC = lotsa '''D'''NA in relation to cell. | *Memory device: A'''d'''CC = lotsa '''D'''NA in relation to cell. | ||
Image: | ====Image==== | ||
* | <gallery> | ||
Image:Adenoid_cystic_carcinoma_cytology.jpg | Adenoid cystic carcinoma - cytology. (WC) | |||
</gallery> | |||
==Epithelial-myoepithelial carcinoma== | |||
{{Main|Epithelial-myoepithelial carcinoma}} | |||
===Cytology=== | |||
Features: | |||
*Single cells/stripped nuclei. | |||
*3-dimensional clusters. | |||
*Two cell population: | |||
**Dark small cells. | |||
**Light large cells. | |||
=Common= | |||
==Squamous carcinoma== | |||
{{Main|Squamous cell carcinoma}} | |||
*AKA ''squamous cell carcinoma''. | |||
===Cytopathology=== | |||
Features: | |||
*Mix of spindle cells/epithelioid cells, present in clusters, +/-small number of single cells. | |||
*Keratinization: | |||
**Orange/red staining on Pap stain. | |||
***Poorly differentiated SCC = not orange/red. | |||
**"Intense" (blue) staining of cells on rapid Romanowsky + pyknotic (small shriveled) nucleus.<ref>GS. 24 February 2010.</ref> | |||
*"Dense" appearing cytoplasm. | |||
**+/-Laminae (layers)/lines in the cytoplasm. | |||
*Nuclear features of malignancy (required for diagnosis): | |||
*#Irregular nuclear membrane, e.g. notches, sharp discontinuities. | |||
*#Nuclear hyperchromasia - "jet-black" nuclei on Pap stain '''key feature'''. | |||
*#Increased NC ratio. | |||
*#Variation of nuclear size from cell-to-cell. | |||
*#Granular chromatin. | |||
Notes: | |||
#One should see abnormal squamous cells to call it SCC. | |||
#Poorly differentiated SCC may look like [[adenocarcinoma]]. | |||
==Melanoma== | ==Melanoma== | ||
| Line 206: | Line 391: | ||
***Nucleus typically eccentric. | ***Nucleus typically eccentric. | ||
*Brown granular cytoplasm; usually fine granularity. | *Brown granular cytoplasm; usually fine granularity. | ||
*Large red nucleoli (classic finding). | *Large [[red nucleoli]] (classic finding). | ||
*+/-Intranuclear inclusions. | *+/-Intranuclear inclusions. | ||
*+/-Binucleation. | *+/-Binucleation. | ||
| Line 215: | Line 400: | ||
Notes: | Notes: | ||
#IHC stains are needed in many cases (S-100, HMB-45, Melan A). | #[[IHC]] stains are needed in many cases (S-100, HMB-45, Melan A). | ||
#The classic appearance of melanoma without pigment is closest to adenocarcinoma (which may have red nucleoli, large cells, abundant cytoplasm, occasional binucleation). | #The classic appearance of melanoma without pigment is closest to [[adenocarcinoma]] (which may have red nucleoli, large cells, abundant cytoplasm, occasional binucleation). | ||
#*Differentiating morphologic features: adenocarcinoma - 3-D clusters of cells, no spindle-shaped cells. | #*Differentiating morphologic features: adenocarcinoma - 3-D clusters of cells, no spindle-shaped cells. | ||
=Lymph nodes= | |||
==Normal lymph node== | |||
===Cytology=== | |||
*Mixed population of lymphoid cells. | *Mixed population of lymphoid cells. | ||
*+/-Lymphoglandular bodies. | |||
====Image==== | |||
*[http://moon.ouhsc.edu/kfung/jty1/CytoLearn/CytoQuiz/CQ-021-040/CI-Image-0803/FQ-044b.gif Lymphoglandular bodies in a DLBCL (ouhsc.edu)].<ref name=ouhsc_nine>URL: [http://moon.ouhsc.edu/kfung/jty1/CytoLearn/CytoQuiz/CQ-021-040/CQ-024-M.htm http://moon.ouhsc.edu/kfung/jty1/CytoLearn/CytoQuiz/CQ-021-040/CQ-024-M.htm]. Accessed on: 9 April 2012.</ref> | |||
==Non-Hodgkin's lymphoma== | |||
*[[AKA]] ''[[lymphoma]]''. | |||
== | ===Cytology=== | ||
Features: | Features: | ||
*Population of monomorphous lymphoid cells. | *Population of monomorphous lymphoid cells - usu. ~2x the size of a RBC. | ||
*Lymphoglandular bodies - blue-grey bodies. | *Lymphoglandular bodies - blue-grey bodies. | ||
**Often about 1/2 the size of a RBC. | **Often about 1/2 the size of a RBC. | ||
***These may be seen in benign tissue. | ***These may be seen in benign tissue. | ||
===Hodgkin's lymphoma=== | Note: | ||
*[[Small cell lymphoma]]s cannot be diagnosed definitively from cytology. | |||
====Image==== | |||
*[http://moon.ouhsc.edu/kfung/jty1/CytoLearn/CytoQuiz/CQ-021-040/CI-Image-0803/FQ-044b.gif DLBCL with lymphoglandular bodies (ouhsc.edu)].<ref name=ouhsc_nine>URL: [http://moon.ouhsc.edu/kfung/jty1/CytoLearn/CytoQuiz/CQ-021-040/CQ-024-M.htm http://moon.ouhsc.edu/kfung/jty1/CytoLearn/CytoQuiz/CQ-021-040/CQ-024-M.htm]. Accessed on: 9 April 2012.</ref> | |||
==Hodgkin's lymphoma== | |||
{{Main|Hodgkin lymphoma}} | |||
===Cytology=== | |||
Features: | Features: | ||
*Reed-Sternberg cell (diagnostic). | *Reed-Sternberg cell (diagnostic). | ||
**Classically binucleated. | **Classically binucleated. | ||
**Huge cell with macronucleus. | **Huge cell with macronucleus. | ||
**Each nucleus has a huge | **Each nucleus has a huge macro[[nucleolus]]. | ||
***Macronucleolus approximately the size of a RBC. | ***[[Macronucleolus]] approximately the size of a [[RBC]]. | ||
*Commonly seen with eosinophils. | *Commonly seen with eosinophils. | ||
==Cystic lesions of the neck | Note: | ||
*RSCs are usually found at the edge of smears.<ref name=ouhsc_q26>URL: [http://moon.ouhsc.edu/kfung/jty1/CytoLearn/CytoQuiz/CQ-021-040/CQ-026-M.htm http://moon.ouhsc.edu/kfung/jty1/CytoLearn/CytoQuiz/CQ-021-040/CQ-026-M.htm]. Accessed on: 9 April 2012.</ref> | |||
====Images==== | |||
<gallery> | |||
Image:Hodgkin_lymphoma_cytology_small.jpg | HL - higher mag. (WC) | |||
Image:Hodgkin_lymphoma_cytology_large.jpg | HL - lower mag. (WC) | |||
</gallery> | |||
www: | |||
*[http://moon.ouhsc.edu/kfung/jty1/CytoLearn/CytoQuiz/CQ-021-040-Ans/CI-Image-0803/FQ-046b.gif HL (ouhsc.edu)].<ref name=ouhsc_q26/> | |||
=Cystic lesions of the neck= | |||
===General=== | ===General=== | ||
*One should never sign-out a cytology specimen as: "[[branchial cleft cyst]]" or "[[thyroglossal duct cyst]]". | *One should never sign-out a cytology specimen as: "[[branchial cleft cyst]]" or "[[thyroglossal duct cyst]]". | ||
| Line 247: | Line 458: | ||
===DDx=== | ===DDx=== | ||
Lateral: | Lateral: | ||
* | *[[Branchial cleft cyst]]. | ||
*Cystic hygroma. | *[[Cystic hygroma]]. | ||
Medial: | Medial: | ||
*Thyroglossal duct cyst. | *[[Thyroglossal duct cyst]]. | ||
Both: | Both: | ||
*Epidermoid cyst. | *[[Epidermoid cyst]]. | ||
*Cystic | *Cystic [[squamous cell carcinoma]]. | ||
=See also= | |||
*[[Cytopathology]]. | *[[Cytopathology]]. | ||
*[[Thyroid]]. | *[[Thyroid]]. | ||
*[[Head and neck pathology]]. | *[[Head and neck pathology]]. | ||
=References= | |||
{{reflist|2}} | {{reflist|2}} | ||
[[Category:Cytopathology]] | [[Category:Cytopathology]] | ||
Latest revision as of 16:09, 4 November 2024

Head and neck cytopathology is a small part of cytopathology. Non-cytopathology head & neck pathology is dealt with in the head and neck pathology article.
Thyroid cytopathology is dealt with in the thyroid cytopathology article. An introduction to cytopathology is in the cytopathology article.
Salivary gland cytopathology and salivary gland cytology redirect to here.
Proposed Milan system for reporting salivary gland cytopathology
- Milan system and Milan classification redirect here.
| Category | Typical management | Comments |
|---|---|---|
| Nondiagnostic | repeat FNA | |
| Nonneoplastic | follow-up/discharge | |
| Atypia of undetermined significance (AUS) | repeat FNA | use should be minimized - like FLUS and ASCUS |
| Neoplasm | excision | subdivided into: (a) benign (b) salivary gland neoplasm of uncertain malignant potential (SUMP) |
| Suspicious for malignancy | wide excision +/-lymph nodes (?) | |
| Malignant | wide excision & lymph nodes (?) |
Notes:
- This classification is still evolving.[1] The preliminary version (above) was presented by Dr. William Faquin at USCAP 2016 in Seattle.[2]
- The goal is to complete the reporting system by the summer of 2017.
Normal
Depends on the structure that is needled.
Parotid:[3]
- Acini - small globoid clusters.
- Separated by adipose tissue.
- Granular cytoplasm.
- Nucleus:
- Dispersed chromatin.
- Indistinct nucleolus.
- Low NC ratio cells.
Sticky lymphoid tissue:
- Irregular globs of tissue with small cells.
- Round red staining globs +/-apparent striations.
- Nuclei more at edges (peripheral).
Images
SM - intermed. mag.

SM - high mag.

SM - very high mag.

SM - very high mag.

SM - high mag.

SM - high mag.

SM - very high mag.

SM - very high mag.








Salivary gland tumours - summary
Benign
| Diagnosis | Architecture | Cytoplasm | Nucleus | Main DDx | Used to diff. from main DDx | Image |
|---|---|---|---|---|---|---|
| Pleomorphic adenoma | Fluffy fibromyxoid material & cells and single (plasmacytoid-like) myoepithelial cells | ? | Myoepithelial cells - plasmacytoid appearance | DDx (?) | ? | |
| Warthin tumour (papillary cystadenoma lymphomatosum) | Sheets of uniformly spaced oncocytes, lymphocytes, necrotic debris | Oncocytes (abundant, granular, eosinophilic tinge), well-defined cell borders | Oncocytes have nucleolus | Acinic cell carcinoma (AcCC), oncocytoma | AcCC: irregular spaced cells, lack well-defined cell borders |


Malignant
| Diagnosis | Architecture | Cytoplasm | Nucleus | Main DDx | Used to diff. from main DDx | Image |
|---|---|---|---|---|---|---|
| Mucoepidermoid carcinoma | Clumps of cells | Abundant whispy cytoplasm | Small oval nucleus, +/-distinct nucleolus | Mucocele ? | Nuclear atypia | |
| Adenoid cystic carcinoma (AdCC) | Circular islands of abundant very small cells | Scant cytoplasm | Small nucleus - may have carrot shape | AcCC | Basement membrane material - PAS-D+ve[4] | |
| Acinic cell carcinoma (AcCC) | 3-D clusters of small cells | Abundant orangeophilic granular cytoplasm | Stippled chromatin | Warthin tumour | AcCC missing lymphocytic background; irreg. spacing of cells |



Salivary gland
Sialoadenitis
Cytology
Features:
- Inflammatory cells - lymphocytes, plasma cells - key features.
- +/-Squamous metaplasia.
- +/-Necrotic debris.
- Benign ductal epithelium.
DDx:
- Squamous carcinoma.
- Mucoepidermoid carcinoma.
Crystals in salivary gland specimens
General
- Uncommon in general.
- Typical location is: parotid (>85% salivary gland specimens with crystals[5]).
- May be seen in the context of any diagnostic category (non-diagnostic, benign, neoplastic, malignant).
DDx:
- Amylase crystalloids ~ 75%.
- Tyrosine crystalloids ~ 11%.
- Collagenous crystalloids ~ 3%.
- Undetermined type ~ 11%.
Cytology
- Amylase crystalloids: rhomboid (or polygonal) +/- "pointy" ends, nonbirefringent.
- Tyrosine crystalloids: floret-like structures, refractile.
- Collagenous crystalloids: needle-shaped, radially arranged.
Images

Amylase crystals - parotid - intermed. mag.

Amylase crystals - parotid - intermed. mag.

Amylase crystals - parotid - high mag.

Amylase crystals - parotid - high mag.

Amylase crystals - parotid - very high mag.

Amylase crystals - parotid - very high mag.

Amylase crystals - parotid - very high mag.

Amylase crystals - parotid - animation - high mag.

Amylase crystals - parotid - animation - very high mag.









Sign out
Crystalloid material is present and has a rhomboid/polygonal shape with occasional "pointy" ends; this is in keeping with amylase crystals.
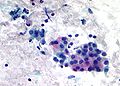
Pleomorphic adenoma
- Abbreviated PA.
General
- Common benign tumour.
Cytology
- Myoepithelial cells.
- Plasmacytoid-like cells.
- Single cells (very common) or small clumps - oval shape.
- Plasmacytoid-like cells.
- Epithelial cells.
- Chondromyxoid stroma.
- Whispy/fluffy groups of spindle cells that overlap (fibromyxoid tissue) - blue-ish.
DDx:
- Adenoid cystic carcinoma.
- Big circular globs (cysts) - common in AdCC.
Images

PA - high mag. (WC)
PA - high mag. (WC)

PA - very high mag. (WC)

PA - very high mag. (WC)




Pleomorphic adenoma. (WC)
Warthin tumour
- AKA papillary cystadenoma lymphomatosum.
General
- Usual smokers.
- May be bilateral.
Cytology
Features:[9]
- Oncocytes.
- Well-defined cell border.
- Granular cytoplasm.
- Nucleoli.
- Oncocytes are often associated with mast cells, i.e. on "top of" oncocytes.
- Mast cells: very granular dark staining cytoplasm (on smears).
- Lymphocytes.
- Necrotic material (cyst contents).
DDx:
- Acinic cell carcinoma.
- Spacing of tumour in AcCC is more irregular and appear more crowded.
- The cell borders in AcCC is less obvious.
- Oncocytoma.
- Oncocytoma (vis-a-vis Warthin tumour) has more cells, more cytoplasm, more granularity of cytoplasm, more complex architecture.[3]
Images

Warthin tumour - high mag. (WC)

Warthin tumour - intermed. mag. (WC)
Warthin tumour - surgical specimen. (WC)


Oncocytoma
General
- May be confused with Warthin tumour.
Cytology
Features:
- Oncocytes.
- Well-defined cell border.
- Granular cytoplasm.
- Nucleoli.
Vis-a-vis Warthin tumour:
- Oncocytoma has:[3]
- More cells,
- More cytoplasm,
- More granularity of cytoplasm,
- More complex architecture.
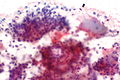
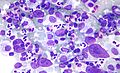
Mucoepidermoid carcinoma
General
- A challenging FNA diagnosis.[10]
Cytology
Features:
- Sheets of cells.
- Cells have a small oval nucleus with nucleolus.
- Fluffy cytoplasm with a pink tinge (on Pap stain) - key feature.
- Cytoplasm not seen in 3-D clusters - look for single layer of cells.
- Cell borders are often distinct.
DDx:
- Squamous cell carcinoma - extensive keratinization and squamous pearls.[11]
Images
Mucoepidermoid carcinoma. (WC)
Mucoepidermoid carcinoma - very high mag. (WC)

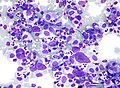
Acinic cell carcinoma
General
- Uncommon.
Cytology
Features:[12]
- Abundant granular cytoplasm.
- Stippled chromatin.
- +/-Nucleolus.
Notes:
- Often accompanied by stripped nuclei; may mimic lymphocytes (may lead to confusion with Warthin tumour).
- Lack:[3]
- Adipocytes between acini (differentiates from normal).
- Ductal structures (differentiates from normal).
Memory device:
- AcCC - lots of "C"s: lots of cytoplasm, carcinoid-like (stippled chromatin, granular cytoplasm).
Image

Acinic cell carcinoma - cytology. (WC)
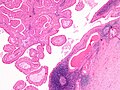
Adenoid cystic carcinoma
General
- Usu. distinctive.
- May be painful due the presence of perineural invasion.
Cytology
Features:
- Solid circular islands that are well-circumscribed.
- Classically forms cystic structures.
- Very cellular.
- Small cells - key feature.
- Nucleus - large relative to cell (high NC ratio)
- Often oval/triangular - may be carrot-shaped.
- +/-Nucleolus. (???)
- Chromatin NOT stippled.
- Scant cytoplasm - key feature.
Notes:
- Memory device: AdCC = lotsa DNA in relation to cell.
Image

Adenoid cystic carcinoma - cytology. (WC)
Epithelial-myoepithelial carcinoma
Cytology
Features:
- Single cells/stripped nuclei.
- 3-dimensional clusters.
- Two cell population:
- Dark small cells.
- Light large cells.
Common
Squamous carcinoma
- AKA squamous cell carcinoma.
Cytopathology
Features:
- Mix of spindle cells/epithelioid cells, present in clusters, +/-small number of single cells.
- Keratinization:
- Orange/red staining on Pap stain.
- Poorly differentiated SCC = not orange/red.
- "Intense" (blue) staining of cells on rapid Romanowsky + pyknotic (small shriveled) nucleus.[13]
- Orange/red staining on Pap stain.
- "Dense" appearing cytoplasm.
- +/-Laminae (layers)/lines in the cytoplasm.
- Nuclear features of malignancy (required for diagnosis):
- Irregular nuclear membrane, e.g. notches, sharp discontinuities.
- Nuclear hyperchromasia - "jet-black" nuclei on Pap stain key feature.
- Increased NC ratio.
- Variation of nuclear size from cell-to-cell.
- Granular chromatin.
Notes:
- One should see abnormal squamous cells to call it SCC.
- Poorly differentiated SCC may look like adenocarcinoma.
Melanoma
Features:
- Usually mixed population of:
- Spindle cells.
- Often single/detacted cells.
- Epithelioid cells - usually predominant.
- Nucleus typically eccentric.
- Spindle cells.
- Brown granular cytoplasm; usually fine granularity.
- Large red nucleoli (classic finding).
- +/-Intranuclear inclusions.
- +/-Binucleation.
Minimal (for morphologic diagnosis):
- Nuclear features of malignancy in epithelioid cells (with an eccentric nucleus) or spindle cells.
- Brown granular cytoplasm.
Notes:
- IHC stains are needed in many cases (S-100, HMB-45, Melan A).
- The classic appearance of melanoma without pigment is closest to adenocarcinoma (which may have red nucleoli, large cells, abundant cytoplasm, occasional binucleation).
- Differentiating morphologic features: adenocarcinoma - 3-D clusters of cells, no spindle-shaped cells.
Lymph nodes
Normal lymph node
Cytology
- Mixed population of lymphoid cells.
- +/-Lymphoglandular bodies.
Image
Non-Hodgkin's lymphoma
Cytology
Features:
- Population of monomorphous lymphoid cells - usu. ~2x the size of a RBC.
- Lymphoglandular bodies - blue-grey bodies.
- Often about 1/2 the size of a RBC.
- These may be seen in benign tissue.
- Often about 1/2 the size of a RBC.
Note:
- Small cell lymphomas cannot be diagnosed definitively from cytology.
Image
Hodgkin's lymphoma
Cytology
Features:
- Reed-Sternberg cell (diagnostic).
- Classically binucleated.
- Huge cell with macronucleus.
- Each nucleus has a huge macronucleolus.
- Macronucleolus approximately the size of a RBC.
- Commonly seen with eosinophils.
Note:
- RSCs are usually found at the edge of smears.[15]
Images
HL - higher mag. (WC)
HL - lower mag. (WC)


{kind=link}
www:
{kind=link}
Cystic lesions of the neck
General
- One should never sign-out a cytology specimen as: "branchial cleft cyst" or "thyroglossal duct cyst".
- The proper verbiage is "cystic squamous lesion".
DDx
Lateral:
Medial:
Both:
- Epidermoid cyst.
- Cystic squamous cell carcinoma.
See also
References
- ↑ URL: http://www.cytopathology.org/the-milan-system-for-reporting-salivary-gland-cytopathology/. Accessed on: 31 March 2016.
- ↑ URL: http://www.uscap.org/meetings/detail/2016-annual-meeting/sessions/2334. Accessed on: 13 March 2016.
- ↑ 3.0 3.1 3.2 3.3 Boerner SL. Patterns and pitfalls in fine needle aspiration of salivary gland. Current Diagnostic Pathology. 9:339-354. 2003. URL (abstract only): http://www.journals.elsevierhealth.com/periodicals/ycdip/article/PIIS0968605303000711/abstract.
- ↑ Chen SY (November 1976). "Adenoid cystic carcinoma of minor salivary gland. Histochemical and electron microscopic studies of cystlike space". Oral Surg. Oral Med. Oral Pathol. 42 (5): 606–19. PMID 62333.
- ↑ 5.0 5.1 5.2 5.3 Sun T, Faquin WC, Torous VF (June 2021). "Crystalloids in FNA specimens of salivary gland lesions: A retrospective study in a single large institute". Cancer Cytopathol 129 (6): 432–438. doi:10.1002/cncy.22395. PMID 33296146.
- ↑ Kishore M, Kaushal M, Dogra S (2019). "Crystalloids in salivary gland lesion: A diagnostic clue". J Lab Physicians 11 (1): 100–101. doi:10.4103/JLP.JLP_120_18. PMC 6437830. PMID 30983813. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6437830/.
- ↑ Thompson, Lester D. R. (2006). Head and Neck Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 295-319. ISBN 978-0443069604.
- ↑ SM. 13 January 2010.
- ↑ http://sciencelinks.jp/j-east/article/200123/000020012301A0753392.php
- ↑ Cohen, MB.; Fisher, PE.; Holly, EA.; Ljung, BM.; Löwhagen, T.; Bottles, K.. "Fine needle aspiration biopsy diagnosis of mucoepidermoid carcinoma. Statistical analysis.". Acta Cytol 34 (1): 43-9. PMID 2296840.
- ↑ Sidawy, Mark K.; Ali, Syed Z. (2007). Fine Needle Aspiration Cytology: A Volume in Foundations in Diagnostic Pathology (1st ed.). Churchill Livingstone. pp. 25. ISBN 978-0443067310.
- ↑ SB. 12 January 2010.
- ↑ GS. 24 February 2010.
- ↑ 14.0 14.1 URL: http://moon.ouhsc.edu/kfung/jty1/CytoLearn/CytoQuiz/CQ-021-040/CQ-024-M.htm. Accessed on: 9 April 2012.
- ↑ 15.0 15.1 URL: http://moon.ouhsc.edu/kfung/jty1/CytoLearn/CytoQuiz/CQ-021-040/CQ-026-M.htm. Accessed on: 9 April 2012.