Difference between revisions of "Small cell carcinoma of the lung"
(→IHC) |
(→Possible LCNEC: tweak) |
||
| (5 intermediate revisions by the same user not shown) | |||
| Line 8: | Line 8: | ||
| Subtypes = large cell neuroendocrine carcinoma (LCNEC) | | Subtypes = large cell neuroendocrine carcinoma (LCNEC) | ||
| LMDDx = poorly differentiated [[adenocarcinoma of the lung]], [[atypical carcinoid]], [[lung carcinoid]], metastatic [[small cell carcinoma]], [[lymphoma]], other [[small round blue cell tumours]] | | LMDDx = poorly differentiated [[adenocarcinoma of the lung]], [[atypical carcinoid]], [[lung carcinoid]], metastatic [[small cell carcinoma]], [[lymphoma]], other [[small round blue cell tumours]] | ||
| Stains = chromogranin +ve, synaptophysin +ve, CD56 +ve, NSE +ve, TTF-1 +ve | | Stains = | ||
| IHC = chromogranin +ve, synaptophysin +ve, CD56 +ve, NSE +ve, TTF-1 +ve, Ki-67 (>50%) | |||
| EM = | | EM = | ||
| Molecular = | | Molecular = | ||
| Line 104: | Line 104: | ||
*CK7 -ve.<ref name=pmid10874668>{{Cite journal | last1 = Gyure | first1 = KA. | last2 = Morrison | first2 = AL. | title = Cytokeratin 7 and 20 expression in choroid plexus tumors: utility in differentiating these neoplasms from metastatic carcinomas. | journal = Mod Pathol | volume = 13 | issue = 6 | pages = 638-43 | month = Jun | year = 2000 | doi = 10.1038/modpathol.3880111 | PMID = 10874668 }}</ref> | *CK7 -ve.<ref name=pmid10874668>{{Cite journal | last1 = Gyure | first1 = KA. | last2 = Morrison | first2 = AL. | title = Cytokeratin 7 and 20 expression in choroid plexus tumors: utility in differentiating these neoplasms from metastatic carcinomas. | journal = Mod Pathol | volume = 13 | issue = 6 | pages = 638-43 | month = Jun | year = 2000 | doi = 10.1038/modpathol.3880111 | PMID = 10874668 }}</ref> | ||
*[[CK20]] -ve.<ref name=pmid10874668/> | *[[CK20]] -ve.<ref name=pmid10874668/> | ||
*Ki-67 ~80% | *Ki-67 ~80% (>50% proposed as criteria for ''large cell neuroendocrine carcinoma''<ref name=pmid25318848>{{Cite journal | last1 = Liu | first1 = SZ. | last2 = Staats | first2 = PN. | last3 = Goicochea | first3 = L. | last4 = Alexiev | first4 = BA. | last5 = Shah | first5 = N. | last6 = Dixon | first6 = R. | last7 = Burke | first7 = AP. | title = Automated quantification of Ki-67 proliferative index of excised neuroendocrine tumors of the lung. | journal = Diagn Pathol | volume = 9 | issue = | pages = 174 | month = | year = 2014 | doi = 10.1186/s13000-014-0174-z | PMID = 25318848 }}</ref>). | ||
**Useful for separating from ''atypical carcinoid'' and ''typical carcinoid''. | **Useful for separating from ''atypical carcinoid'' and ''typical carcinoid''. | ||
| Line 111: | Line 111: | ||
==Sign out== | ==Sign out== | ||
===Biopsy=== | |||
<pre> | <pre> | ||
Lung, Left Lower Lobe, Core Biopsy: | Lung, Left Lower Lobe, Core Biopsy: | ||
| Line 116: | Line 117: | ||
</pre> | </pre> | ||
===Block letters=== | ====Possible LCNEC==== | ||
<pre> | |||
Lung, Left Lower Lobe, Core Biopsy: | |||
- NON–SMALL CELL CARCINOMA WITH NEUROENDOCRINE (NE) MORPHOLOGY AND POSITIVE NE MARKERS, POSSIBLE LARGE CELL NEUROENDOCRINE CARCINOMA (LCNEC). | |||
</pre> | |||
Note: | |||
*The above is the wording recommended by 2011 ATS/ERS/IASLC panel.<ref>{{cite journal |authors=Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger K, Yatabe Y, Ishikawa Y, Wistuba I, Flieder DB, Franklin W, Gazdar A, Hasleton PS, Henderson DW, Kerr KM, Petersen I, Roggli V, Thunnissen E, Tsao M |title=Diagnosis of lung cancer in small biopsies and cytology: implications of the 2011 International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification |journal=Arch Pathol Lab Med |volume=137 |issue=5 |pages=668–84 |date=May 2013 |pmid=22970842 |pmc=4509741 |doi=10.5858/arpa.2012-0263-RA |url=}}</ref> | |||
====Block letters==== | |||
<pre> | <pre> | ||
LOWER LOBE OF LUNG, LEFT, CORE BIOPSY: | LOWER LOBE OF LUNG, LEFT, CORE BIOPSY: | ||
Latest revision as of 21:53, 10 December 2021
| Small cell carcinoma of the lung | |
|---|---|
| Diagnosis in short | |
_by_core_needle_biopsy.jpg) Lung small cell carcinoma. H&E stain. | |
|
| |
| LM | stippled chromatin, high NC ratio with scant basophilic cytoplasm, typically small cells (~2x RBC diameter), +/-nuclear moulding, nuclei with smudgy appearance (Azzopardi phenomenon), necrosis, mitoses |
| Subtypes | large cell neuroendocrine carcinoma (LCNEC) |
| LM DDx | poorly differentiated adenocarcinoma of the lung, atypical carcinoid, lung carcinoid, metastatic small cell carcinoma, lymphoma, other small round blue cell tumours |
| IHC | chromogranin +ve, synaptophysin +ve, CD56 +ve, NSE +ve, TTF-1 +ve, Ki-67 (>50%) |
| Staging | lung cancer staging |
| Site | lung - see lung tumours |
|
| |
| Clinical history | smoking - usually a long history, heavy |
| Signs | +/-hemoptysis |
| Prevalence | not common |
| Radiology | lung mass, usu. central location |
| Prognosis | poor |
| Clin. DDx | other lung tumours (squamous cell carcinoma of the lung), metastatic tumours |
| Treatment | medical (chemotherapy) |
Small cell carcinoma of the lung, also small cell lung carcinoma (abbreviated SCLC)[1] is an aggressive malignant tumour of the lung. It is strongly associated with smoking.
Small cell carcinoma in general is dealt with in the small cell carcinoma article.
General
- Strong association with smoking.
- Typically treated with chemotherapy.
- Poor prognosis.
On a spectrum of lesions (benign to malignant):[1]
- Tumourlet.
- Carcinoid.
- Atypical carcinoid.
- Small cell carinoma/large cell neuroendocrine carcinoma (LCNEC).
Precursor lesion - uncommonly seen:
- Pulmonary neuroendocrine cell hyperplasia.[1]
Clinical:
- +/-Hemoptysis.
Gross
- Central location (close to large airways) - typical.
- Necrosis.
Images

Small cell carcinoma of the lung - centre of image. (WC/Rosen)
.jpg)
Microscopic
Features:
- Stippled chromatin.
- High NC ratio, scant basophilic cytoplasm.
- Typically small cells ~2x RBC diameter.
- +/-Nuclear moulding.
- Nuclei with a smudgy appearance (Azzopardi phenomenon).
- Necrosis.
- Mitoses.
Notes:
- There should be no nucleolus.
DDx:
- Poorly differentiated adenocarcinoma of the lung.
- Metastatic small cell carcinoma.
- Lymphoma.
- Atypical carcinoid.
- Basaloid squamous cell carcinoma of the lung.[2]
- Non-small cell carcinoma of the lung.
- Other small round blue cell tumours.
Subtypes
- Large cell neuroendocrine carcinoma (LCNEC).
Grading
As per CAP protocol (version 3.4.0.0):[3]
- G4 = undifferentiated - used for small cell carcinoma and large cell carcinoma.
Images
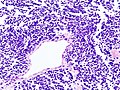
SCLC - low mag. (WC)
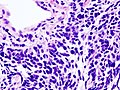
SCLC - high mag. (WC)
_by_core_needle_biopsy.jpg)
IHC
- Synaptophysin +ve.
- May be very weak.
- TTF-1 +ve
- CK7 -ve.[6]
- CK20 -ve.[6]
- Ki-67 ~80% (>50% proposed as criteria for large cell neuroendocrine carcinoma[7]).
- Useful for separating from atypical carcinoid and typical carcinoid.
Others:
Sign out
Biopsy
Lung, Left Lower Lobe, Core Biopsy: - SMALL CELL CARCINOMA.
Possible LCNEC
Lung, Left Lower Lobe, Core Biopsy: - NON–SMALL CELL CARCINOMA WITH NEUROENDOCRINE (NE) MORPHOLOGY AND POSITIVE NE MARKERS, POSSIBLE LARGE CELL NEUROENDOCRINE CARCINOMA (LCNEC).
Note:
- The above is the wording recommended by 2011 ATS/ERS/IASLC panel.[9]
Block letters
LOWER LOBE OF LUNG, LEFT, CORE BIOPSY: - SMALL CELL CARCINOMA.
Resection
Left Lower Lobe, Lobectomy:
- LARGE CELL NEUROENDOCRINE CARCINOMA.
-- Margins clear.
- Two lymph nodes NEGATIVE for malignancy (0/2).
- Please see synoptic report.
Comment:
The tumour stains as follows:
POSITIVE: CD56, synaptophysin, p63 (scattered).
NEGATIVE: chromogranin A, CK5/6, TTF-1, napsin A.
Micro
The sections show large cells epithelioid cells (~3-4x the size of a lymphocyte) with salt and pepper chromatin, scant basophilic cytoplasm, and focally streaming. Mitotic activity is brisk and multifocal zonal necrosis is present.
See also
References
- ↑ 1.0 1.1 1.2 Travis, WD. (Oct 2010). "Advances in neuroendocrine lung tumors.". Ann Oncol 21 Suppl 7: vii65-71. doi:10.1093/annonc/mdq380. PMID 20943645.
- ↑ Maleki, Z. (Mar 2011). "Diagnostic issues with cytopathologic interpretation of lung neoplasms displaying high-grade basaloid or neuroendocrine morphology.". Diagn Cytopathol 39 (3): 159-67. doi:10.1002/dc.21351. PMID 21319315.
- ↑ CAP Lung protocol. Version: 3.4.0.0. URL: http://www.cap.org/ShowProperty?nodePath=/UCMCon/Contribution%20Folders/WebContent/pdf/cp-lung-16protocol-3400.pdf. Accessed on: March 23, 2016.
- ↑ Misch, D.; Blum, T.; Boch, C.; Weiss, T.; Crolow, C.; Griff, S.; Mairinger, T.; Bauer, TT. et al. (Apr 2015). "Value of thyroid transcription factor (TTF)-1 for diagnosis and prognosis of patients with locally advanced or metastatic small cell lung cancer.". Diagn Pathol 10: 21. doi:10.1186/s13000-015-0250-z. PMID 25889870.
- ↑ Wu, M.; Szporn, AH.; Zhang, D.; Wasserman, P.; Gan, L.; Miller, L.; Burstein, DE. (Oct 2005). "Cytology applications of p63 and TTF-1 immunostaining in differential diagnosis of lung cancers.". Diagn Cytopathol 33 (4): 223-7. doi:10.1002/dc.20337. PMID 16138374.
- ↑ 6.0 6.1 Gyure, KA.; Morrison, AL. (Jun 2000). "Cytokeratin 7 and 20 expression in choroid plexus tumors: utility in differentiating these neoplasms from metastatic carcinomas.". Mod Pathol 13 (6): 638-43. doi:10.1038/modpathol.3880111. PMID 10874668.
- ↑ Liu, SZ.; Staats, PN.; Goicochea, L.; Alexiev, BA.; Shah, N.; Dixon, R.; Burke, AP. (2014). "Automated quantification of Ki-67 proliferative index of excised neuroendocrine tumors of the lung.". Diagn Pathol 9: 174. doi:10.1186/s13000-014-0174-z. PMID 25318848.
- ↑ Au, NH.; Gown, AM.; Cheang, M.; Huntsman, D.; Yorida, E.; Elliott, WM.; Flint, J.; English, J. et al. (Sep 2004). "P63 expression in lung carcinoma: a tissue microarray study of 408 cases.". Appl Immunohistochem Mol Morphol 12 (3): 240-7. PMID 15551738.
- ↑ Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger K, Yatabe Y, Ishikawa Y, Wistuba I, Flieder DB, Franklin W, Gazdar A, Hasleton PS, Henderson DW, Kerr KM, Petersen I, Roggli V, Thunnissen E, Tsao M (May 2013). "Diagnosis of lung cancer in small biopsies and cytology: implications of the 2011 International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification". Arch Pathol Lab Med 137 (5): 668–84. doi:10.5858/arpa.2012-0263-RA. PMC 4509741. PMID 22970842. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4509741/.