Gynecologic cytopathology

Gynecologic cytopathology is a subset of cytopathology. Gynecologic usually refers to Pap test specimens, i.e. uterine cervix, vaginal vault; other gynecologic specimens are considered non-gynecologic.
This article deals only with cervical cytopathology. An introduction to cytopathology is in the cytopathology article.
Cervical cytology redirects to this article.
Preparation
The standard for Pap test is the Papanicolaou stain. It is described in the staining article and discussed in the context of cytopathology in the cytopathology article.
Slide marking conventions
Conventions are important for facilitating communication between various team members. They are discussed in the cytopathology article.
Normal cells
Squamous cell types:[1]
- Intermediate cells:
- In clusters or single.
- 30-50 micrometres in diameter.
- Associated with progesterone - (light) blue.
- This is the cell of reference in Pap test, i.e. other cells are measured against this cell when assessing a Pap test.
- Nucleus ~ 7-8 micrometers.
- Slightly smaller than a neutrophil.
- Nucleus ~ 7-8 micrometers.
- Parabasal cells:
- Blue-grey.
- Associated with atrophy.
- Basal cells:
- Small cells.
- Rarely seen.
- Superficial cell:[2]
- Nucleus smaller than for intermediate cell.
- Cytoplasm red.
- Orange staining superficial cells are hypermature - suggests (abnormal) keratinization.
Glandular cells:[3]
- Sheets of cells with regular spacing.
- Relatively high NC ratio (when compared to intermediate cells).
- Nucleoli (like most glandular cells).
- Nucleus approximately the size of an intermediate cell nucleus.
Images
-
 Endocervical epithelium - high mag. (WC)
Endocervical epithelium - high mag. (WC) -
 Endocervical epithelium - very high mag. (WC)
Endocervical epithelium - very high mag. (WC) -
 Endocervical epithelium - high mag. (WC)
Endocervical epithelium - high mag. (WC) -
 Endocervical epithelium - very high mag. (WC)
Endocervical epithelium - very high mag. (WC) -
 Endocervical epithelium - high mag. (WC)
Endocervical epithelium - high mag. (WC) -
 Endocervical epithelium - very high mag. (WC)
Endocervical epithelium - very high mag. (WC)






-
Endocervical cells and LSIL. (WC)
Mix of cells
The mix of cells is dependent on age and hormones:[4]
- Progesterone - makes the Pap test blue... more intermediate cells.
- Yonger patients have a mix of cells.
- Menopausal patients... more parabasal cells.
- Older patients... more estrogen, glycogen.
Less common non-malignant cells
- Clue cells.
- Squamous metaplastic cells.
- Endometrial cells.
- Atrophic cells.
- Tingible body macrophages.
- Navicular cells.
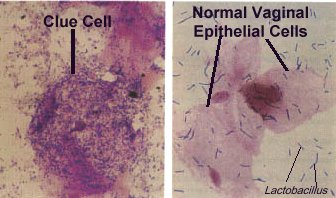
Clue cells
Features:
- Purple squamous cell covered with rod-shaped bacteria.
Notes:
- The cytologic finding of bacterial vaginosis.
Image:
Squamous metaplastic cells
Features:
- "Dense" cytoplasm.
- Nucleus ~2X the size of an intermediate cell nucleus.
- Nucleolus (small) - important.
- Regular/smooth nuclear membrane.
Note:
- Squamous metaplastic cells have a similar appearance to parabasal cells; they cannot be differentiated on morphologic grounds.
- Squamous metaplastic cells have a high NC ratio - they are differentiated from HSIL via nuclear features (dark staining + irregular nuclear contour = HSIL).
- Slight nuc. contour irregularies are accepted, may be darker staining.
Images
-
 SM - high mag. (WC)
SM - high mag. (WC) -
 SM - very high mag. (WC)
SM - very high mag. (WC) -
 SM - very high mag. (WC)
SM - very high mag. (WC)



Endometrial cells
Features:[5]
- Cluster of cells with a well-defined border that is bilayered, i.e. a clump of (epithelioid) stromal cells surrounded by (flatted) glandular cells. Classically described as a cluster with a double contour; known as exodus pattern.[6]
- Scant cytoplasm.
- Chromatin clumping.
- Raisin-like nuclei - approximately the size of an intermediate cell nucleus.
- Nuclei can be considered normal if nucleus less than 2X the size of an intermediate cell nucleus.
Notes:
- Endometrial cells may appear irregular in the context of an intrauterine device (IUD); abnormalities in the context of an IUD are often ignored.
- Cytology: cytoplasmic vacuolization, +/-multinucleation.
- May be signet ring cell-like.
- Cytology: cytoplasmic vacuolization, +/-multinucleation.
- The presence of endometrial cells on a Pap test on a woman >=40 years old (per Bethesda guidelines) should be noted in the pathology report[7] - this prompts an endometrial biopsy.
- The practise of reporting benign endometrial cells in premenopausal women is not backed by evidence that demonstrates a significant benefit.
Images
-
 Endometrial cells - very high mag.
Endometrial cells - very high mag. -
 Endometrial cells - very high mag.
Endometrial cells - very high mag. -
 Endometrial cells - very high mag.
Endometrial cells - very high mag. -
 Endometrial cells - very high mag.
Endometrial cells - very high mag.




-
 Endometrial cells - high mag.
Endometrial cells - high mag. -
 Endometrial cells - very high mag.
Endometrial cells - very high mag. -
 Endometrial cells - very high mag.
Endometrial cells - very high mag.



www:
- Endometrial cells - double contour (techriver.net).
- Endometrial cells with "exodus" pattern (techriver.net).
Atrophic cells
Features:[8]
- Cells smaller.
- Cytoplasm grey/blue.
- No "dancing"/"sparkling" chromatin.
- +/-"Dirty" background - degenerated cells, inflammatory cells (neutrophils, histiocytes).
- May mimic "dirty" background of tumour, i.e. 'tumour diathesis'.
Notes:
- Usually older women.
- May be a cellular cluster.
DDx:
- HSIL - chromatin pattern irregular.
Tingible body macrophages
Features:
- Abundant cytoplasm with vacuolization.
- May be seen in the context of chlamydia.
Features:
- Intermediate cells with:
- Folded edges.
- Abundant cytoplasmic glycogen - central yellow.
Images
-
 NC - very high mag.
NC - very high mag. -
 NC - very high mag.
NC - very high mag. -
 NC - extremely high mag.
NC - extremely high mag. -
 NCs - extremely high mag.
NCs - extremely high mag.




Glycogen halos versus HPV effect
| HPV effect (koilocyte) | Glycogen halo | |
|---|---|---|
| Discolouration of halo | Clear | Yellow |
| Nuclear changes | Associated with nuc. changes | Normal nuclei |
| Cell-to-cell variability | No - all clear | Yes - some yellow some clear |
Gynecologic pathology in tables
Normal cells
| Cell | Architecture | Cell borders | Cytoplasm | DNA | DDx |
|---|---|---|---|---|---|
| Intermediate cell (IC) | Single cells | Irregular | Blue, abundant | Small nucleus (~ size of PMN), no nucleolus | - |
| Superficial cell (SC) | Single cells | Irregular | Red, abundant | Small nucleus, 1/2 size of IC nucleus, no nucleolus | - |
| Squamous metaplastic cell | Single cells/clumps of cells | Smooth/oviod shape | Dense, dark blue | 2X IC nucleus, nucleolus, no membrane irreg., no chromatin changes | DDx: HSIL, basal cell |
| Endometrial cell | Well-circumscribed clump/ball of cells with squamoid covering cells; referred to as "exodus" pattern[9] | Indistinct within cluster | Blue, small/very scant | Small, dark, nuclear moulding, degenerative changes (chromatin clumping) | DDx: HSIL, basal cell. |
| Glandular (endocervical) cell | Sheets of cells with regular spacing, columnar morphology may be apparent, +/-palisading at edge of clump | Often distict | Blue, scant-to-moderate | Nucleus ~ size of an IC nucleus, no membrane irreg., no chromatin changes | DDx: endometrial cell |
| Atrophy | Single cells/groups | Well-circumscribed | Grey/blue dense, may be scant | Large NC ratio, nuc. membrane irregularities, NO chromatin clumping[10] | DDx: HSIL |
| Radiation changes | Single cells/groups | Well-circumscribed | vacuolated, usu. abundant | Normal NC ratio, enlarged nucleus, no nuclear membrane irregularies, +/-multinucleation | DDx: LSIL, vitamin B12 def. |
Note:
- If only normal cells are present the diagnosis is negative for intraepithelial lesion and malignancy (NILM).
Abnormal cells
| Cell | Architecture | Cell borders | Cytoplasm | DNA | Other | Image |
|---|---|---|---|---|---|---|
| Low-grade squamous intraepithelial lesion (LSIL) | Single cells/groups | Irregular or moderately-circumscribed | Blue, abundant - NC ratio ~ 1:3 | Large nucleus (3-4X IC nuc. - see Note 1), perinuclear clearing, nuc. membrane irregularities, chromatin clumping | DDx: HSIL, reactive changes |  |
| High-grade squamous intraepithelial lesion (HSIL) | Often single cells, may be groups | Well-circumscribed | Dark blue, scant - NC ratio ~ 1:2 | Large nucleus (3-4X IC nuc. - see Note 1), nuc. membrane irregularities, clumping of coarse chromatin, dark nuc. staining, +/- small nucleoli | DDx: squamous metaplasia, atrophy with atypia, superficial endometrial cells |  |
| Atypical squamous cells of undetermined significance (ASC-US) | Single cells/groups | Irregular or moderately-circumscribed | Blue, abundant cytoplasm | Moderately enlarged nucleus (~2.5-3.0X IC nuc.), minimal changes in nuclear membrane and chromatin | DDx: LSIL, reactive changes | |
| Atypical squamous cells, cannot exclude HSIL (ASC-H) | Often single cells, may be groups | Irregular or moderately-circumscribed | Blue, moderate-to-scant cytoplasm | Moderately enlarged nucleus (~1.5-2.0X IC nuc.), minimal changes in nuclear membrane and chromatin | DDx: HSIL, AIS | |
| Atypical glandular cells (AGC) | Usu. groups of cells | Usually well-circumscribed (?) | Dark blue dense, scant | Moderately enlarged nucleus (~2X IC nuc.), nuc. membrane irregularities, chromatin clumping, dark nuc. staining, nucleoli | DDx: AIS, HSIL | |
| Adenocarcinoma in situ (AIS) | groups; rosette formation | Usually well-circumscribed | Dark blue dense, scant | Large nucleus (>=2X IC nuc.), nuc. membrane irregularities, chromatin clumping, dark nuc. staining, nucleoli (very common), pseudostratification (as in endocervical AIS) | DDx: AGC, HSIL |  |
| Features of SCC (see Note 2) | Large clusters of cells with irreg. edge and "streaming", +/-blood, necrotic debris | Poorly seen | Dark blue dense, scant | Large NC ratio, nucleolus, nuc. membrane irregularities, chromatin clumping | DDx: HSIL |
Note 1:
- LSIL/HSIL nucleus - at least 3X IC nucleus.
- ASCUS nucleus - at least 2.5X IC nucleus.
- 3X is not an absolute requirement to call SIL, i.e. SIL may be called with a smaller nucleus in circumstances where other nuclear features are at the extremus of malignant.
- ASCUS nucleus - at least 2.5X IC nucleus.
- Large nuclear size, membrane irregularities, "clumpy" chromatin and dark nuc. staining - are the key features.
- Perinuclear clearing is quite subjective.
- The best perinuclear halos have a sharp punched-out edge.
- Perinuclear clearing is quite subjective.
Note 2:
- By definition, it is not possible to diagnose squamous cell carcinoma (SCC) on a pap test as one cannot demonstrate stromal invasion.
HSIL versus LSIL
| HSIL | LSIL | |
|---|---|---|
| NC ratio[11] - see Note 1 | ~1:2 | ~1:3 |
| Nuclear membrane irregularities | Marked - distinct notches | Moderate |
| Chromatin granularity | Coarse, clumped, +/-nucleolus (red) | Coarse, no nucleolus |
| Cytoplasmic staining | Dark | Light |
| Perinuclear clearing | Usually absent | Often present |
| Binucleation | Uncommon | May be present |
| Maturity of squamous cell | Normal maturity | Hypermature (orangeophilic cell present) |
| Images (example) |   |
 |
Note 1:
- The single most useful feature is NC ratio but it is not definitive; NC ratio should be evaluated in the context of nuclear irregularities (nuclear membrane smoothness, chromatin pattern, presence of nucleolus).[11]
- It may be easier to think in terms of cell size - approximate values are:
- HSIL cells: < 1/2 size of IC.
- LSIL cells: classically the size of IC.
Infectious organisms
| Disease | Organism | Group | Dx features | Associated features | Clinical | Reference | Image |
|---|---|---|---|---|---|---|---|
| Trichomoniasis | Trichomonas vaginalis | Protozoan | Pear-shaped pale-grey fluffy cytoplasm with well-defined nucleus, approx. 30 μm. | Acute inflammation (PMNs), may be seen with Leptothrix (hair-like appearance ~0.5 x 20 μm) | Sexually transmitted | [12] |   |
| Candidiasis | Candida albicans | Fungi | Branching hyphae ~= 1/2 the dia. of IC nucleus, red | PMNs | ? | ? |  |
| Herpes | Herpes simplex virus (HSV 1 - less commonly, HSV 2 - more commonly) | Virus | Large ground glass nuclei then multinucleation with moulding & inclusions with clear halo | ? | Sexually transmitted | ? |   |
| Actinomycetes | Actinomycetes | Gram-positive bacteria | Clusters of cocci in chains - hyphae-like appearance | low power: pom-pom or fuzzy ball-like appearance | Should prompt removal of IUD, if present. | [12] | Actinomycetes (gfmer.ch), Actinomycetes (quizlet.com) |
| Bacterial vaginosis (see Note 1) | Gardnerella vaginalis | Gram-variable rod | "Clue cell": bacterial clusters attached to a purple squamous cell | ? Assoc. | Fishy smell | ? |  |
Note 1:
- Usually not reported.
Adequacy of specimens
There is a generally accepted standard for cervical (liquid-based) cytology specimens:[13]
- >5000 squamous cells/slide, if no abnormality is present.
- If abnormal cells are present, any number of cells is acceptable.
- This works-out to approx. 4 cells/HPF.
- Where: HPF = area seen at 400X with an eye piece diameter is ~22 mm.
- 10 HPFs are counted and a table is used to see whether the sample is adequate.
- This works-out to approx. 4 cells/HPF.
- If abnormal cells are present, any number of cells is acceptable.
Note:
- The standard for conventional pap smears is: 8000-12000 (well-visualized) squamous cells.[14]
Transformation zone (TZ)
The presence of the TZ should be commented on:[15]
- An adequate TZ is 10 cells - endocervical cells or squamous metaplastic cells (per Bethesda).
Difficulties in obtaining a TZ may arise in the following populations:
- Pregnant (endocervical canal not sampled).
- Menopausal.
- Young nulliparous.
Specific entities - infectious
Candida
General
- Common.
- May be asymptomatic.
- Usually Candida albicans.
Cytology
Features:
- Typically in clusters - lead to darkened clusters of squamous cells (at low power).
- May appear to "shish kabob" the cell; may appear to puncture the cell membrane (as they overlie it).
- Red staining hyphae; width of hyphae ~= 1/2 the diameter of an intermediate cell nucleus; branches.
Notes:
- Presence should be noted in the pathology report.
Images
-
 Candida on Pap test - example 1. (WC)
Candida on Pap test - example 1. (WC) -
 Candida on Pap test - example 2. (WC)
Candida on Pap test - example 2. (WC)

-
 Candida - high mag. (WC)
Candida - high mag. (WC) -
 Candida - very high mag. (WC)
Candida - very high mag. (WC)


www
Trichomoniasis
General
- Caused by Trichomonas vaginalis - a protozoa.
- Sexually transmitted.
- Common.
- Occasionally found in urine cytology specimens.[16]
Cytopathology
Features:
- Low power: grey blob with a nucleus, may be pear-shaped:
- Size: approximately 30 micrometres.[12]
- Shape: usually oval, may have teardrop-shaped.
- Flagellum - hair-thin locomotive stucture, usu. barely visible at 200X - diagnostic feature.
Cytopathological associations:
- Acute inflammation (neutrophils), often marked - key feature at low power.
- Reactive squamous cells with:
- Nucleoli,
- Perinuclear halos, and
- Moth-eaten cytoplasm; cytoplasm that has multiple vacuoles with star-like spaces.
Notes:
- Trichomonas is tricky - it is easy to miss if one is not suspicious, in the context of inflammation.
- May vaguely resemble a neutrophil:
- Flagellum useful to differentiate.
- Neutrophil has multiple lobulations of the nucleus.
- May be seen in association of Leptothrix.
- Appearance: long, hair-like.
- Size: ~0.5 x 20 micrometres.
Images
-
 T. vaginalis - Pap stain. (WC)
T. vaginalis - Pap stain. (WC) -
 T. vaginalis - Pap stain. (WC)
T. vaginalis - Pap stain. (WC) -
 Trichomonas vaginalis - Giemsa stain. (WC)
Trichomonas vaginalis - Giemsa stain. (WC)


-
 Trichomonas - high mag.
Trichomonas - high mag. -
 Trichomonas - very high mag.
Trichomonas - very high mag.


-
 Trichomonas - high mag.
Trichomonas - high mag. -
 Trichomonas - very high mag.
Trichomonas - very high mag.

www
Herpes simplex virus
General
- May be HSV1 or HSV2.
- Classically HSV2 based on epidemiology and location.
Cytology
Features:[12]
- Early: Large "ground-glass" nuclei - nuclei with hazy & uniformly dull appearance.
- Late: multi-nucleation with moulding of nuclei and nuclear inclusions surrounded by a clear halo.
DDx:
- Reactive endocervical cells - may be multinucleated.
Image
-
 HSV on pap test. (WC)
HSV on pap test. (WC)
Actinomycetes
General
- Presence should prompt removal of intrauterine device (IUD), if present.[12]
- Gram-positive bacteria.
- Microorganism part of the large Actinobacteria group.
Cytopathology
Features:[12]
- Clusters of filamentous bacteria.
- Hyphae-like appearance/"filamentous".
Notes:
- Mycete = fungus.[17]
DDx - sulfur granule:[18]
- Hematoidin (cockleburr) crystal - radiating crystal, refractile, classically golden-brown.
Bacterial vaginosis
General
Clinical:
- Fishy odor.
Treatment:
- Antibiotics (metronidazole or clindamycin).[20]
Cytopathology
Features:
- Purple squamous cell covered with rod-shaped micro-organisms.
Image:
Stains
- Gram stain +ve/-ve.
- Gardnerella vaginalis is a gram variable rod.[21]
Sign out
- Usually not reported.
Squamous intraepithelial lesions
- Abbreviated SIL.
General:
- The nucleus makes it SIL.
- The cytoplasm determines the grade (LSIL vs. HSIL).
Management (in short):
- LSIL = repeat Pap test in 6 months.
- HSIL = referral for coloposcopy.
Low-grade squamous intraepithelial lesion
- Abbreviated LSIL.
General
- Usually regress, i.e. will disappear on their own.
- Low inter-rater concordance.[22]
Cytopathology
Features:
- Nuclei 3x size of intermediate cell - key feature. †
- Irregular nuclear border.
- +/-Perinuclear 'cavity' (clearing).
- The best perinuclear halos have a sharp punched-out edge.
- Chromatin clumping/irregular & granular.
Note:
- † Nucleus diameter ~21-24 μm.
- In the context of exams: 2 of criteria 1-3 is enough to call LSIL.[23]
Images
-
 LSIL with HPV effect. (WC)
LSIL with HPV effect. (WC) -
 LSIL. (WC)
LSIL. (WC) -
 LSIL. (WC)
LSIL. (WC)


www:
Sign out
Low grade squamous intraepithelial lesion (LSIL).
Cannot exclude HSIL
At least low grade squamous intraepithelial lesion; CANNOT EXCLUDE high-grade squamous intraepithelial lesion.
High-grade squamous intraepithelial lesion
- Abbreviated HSIL.
General
- Often progress to cervical cancer.
Cytopathology
Features:
- Often single cells, may be in clusters.
- Blue cells - nucleus and cytoplasm.
- Increased NC ratio - key feature.
- Irregular nuclear border.
- Chromatin clumping.
Note:
- Nucleoli uncommon - should prompt consideration of squamous carcinoma.
DDx:
Images
-
 HSIL. (WC)
HSIL. (WC) -
 HSIL. (WC/Nephron)
HSIL. (WC/Nephron)

Squamous cell carcinoma
- Abbreviated SCC.
- Some believe that one can diagnosis SCC on a pap test.
- This is nonsense, as SCC implies invasion which cannot be seen on a pap test.
Features suggestive of invasion:
- Loose clumps of ovoid-to-spindled cells with:
- +/-Orange/red cytoplasm (orangeophilic cytoplasm).
- Nucleoli - key feature.
- Coarse chromatin.
- Nuclear hyperchromasia.
- Necrotic debris - often obscures cell borders:
- Anucleate, fragmented cells - cytoplasm-like material.
- Neutrophils.
Note:
- Nucleoli DDx:
- Reactive changes.
- Glandular lesions (adenocarcinoma in situ, atypical glandular cells).
Image:
Glandular lesions
Adenocarcinoma in situ
- Abbreviated AIS.
Adenocarcinoma in situ on Pap test is classically divided into:
- Endocervical.
- Uterine.
- Extra-uterine.
Adenocarcinoma vs. squamous carcinoma:
- Adenocarcinoma:
- Mucin vacuole.
- Eccentric nucleus.
- Endocervical adenocarcinoma in situ:
- Squamous carcinoma:
- Orangeophilic cytoplasm.
- Central nucleus.
Images
www:
Endocervical adenocarcinoma in situ
- AKA adenocarcinoma in situ of the endocervix.
General
- Associated with HPV.
- May be seen in conjunction with a SIL.
- Management - like AGC and other types of AIS: coloscopy +/- endometrial biopsy.
Cytopathology
Features:
- Cluster of small cells with:
- Moderate nuclear enlargement.
- Coarse chromatin.
- Nucleoli - prominent - key feature.
- +/-Mitoses.
- "Feathering" - picket fence-like arrangement of the cells at the edge of the cell cluster.
- Apoptotic/necrotic cells.
Negatives:
- Lack cilia.
- Cilia on cells is a feature of benignancy and should sway the pathologist away from adenocarcinoma.
DDx:
- AGC - no prominent nucleoli, not 3-dimensional.
- Endometrial adenocarcinoma in situ.
- Metastatic colorectal adenocarcinoma.
- Lower uterine segment epithelium[26] - esp. proliferative phase endometrium - mitoses rare, NC ratio normal.
Image
-
 ECAIS - high mag. (WC)
ECAIS - high mag. (WC) -
 ECAIS - very high mag. (WC)
ECAIS - very high mag. (WC) -
 ECAIS - very high mag. (WC)
ECAIS - very high mag. (WC) -
 ECAIS - high mag. (WC)
ECAIS - high mag. (WC) -
 ECAIS - very high mag. (WC)
ECAIS - very high mag. (WC)




-
 Endocervical AIS. (WC/euthman)
Endocervical AIS. (WC/euthman)

Endometrial adenocarcinoma in situ
- AKA adenocarcinoma in situ of the endometrium.
General
- Management - like AGC and other types of AIS: coloscopy + endometrial biopsy.
Cytopathology
Features:
- Single cells or cluster of small cells with:
- Moderate nuclear enlargement ~2x intermediate cell nucleus.
- Nuclear hyperchromasia.
- Coarse chromatin.
- Nucleoli - prominent - key feature.
- +/-Mitoses.
- +/-Intracytoplasmic neutrophils.
- Apoptotic/necrotic cells.
- +/-Psammoma bodies.
- Suggestive of serous carcinoma of the endometrium.
DDx:
- AGC - no prominent nucleoli, not 3-dimensional.
- Endocervical adenocarcinoma in situ.
Waffle categories
- Like all waffle diagnoses, these should be used sparingly.
Atypical squamous cells of undetermined significance
- Abbreviated ASC-US or ASCUS.
General
- This is a waffle category that should be used sparingly.
- Diagnosis may be an indication for HPV testing.
Cytology
Features:
- Squamous differentiation:
- Central nucleus.
- Dense/solid-appearing cytoplasm.
- Nuclear size >2.5X IC nucleus, but <3X IC nucleus.
- +/-Orange/red cytoplasmic (orangeophilic cytoplasm).[29]
Note:
- One should not see nucleoli.
- Nucleoli are seen in reactive changes and squamous cell carcinoma of the uterine cervix.
- The IC nucleus is ~ 8 μm.[30]
DDx:
Images
-
 ASCUS - high mag. (WC)
ASCUS - high mag. (WC) -
 ASCUS - very high mag. (WC)
ASCUS - very high mag. (WC) -
 ASCUS - high mag. (WC)
ASCUS - high mag. (WC) -
 ASCUS - very high mag. (WC)
ASCUS - very high mag. (WC) -
 ASCUS - very high mag. (WC)
ASCUS - very high mag. (WC)





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sign out
Atypical squamous cells of undetermined significance (ASC-US).
Atypical squamous cells, cannot exclude high-grade squamous intraepithelial lesion
- Abbreviated ASC-H.
General
- This is a waffle category that should be used very rarely.
- Higher HPV positivity vs. ASC-US.[31]
- Management - like HSIL: colposcopy.
Cytology
Features:
- Atypia that falls short of diagnosing HSIL:
- Increased NC ratio.
- Architecture: cell clusters or rare single cells.
DDx:[32]
Atypical glandular cells
- Abbreviated AGC.
- Previously atypical glandular cells of undetermined significance, abbreviated AGUS.
General
- Waffle diagnosis.
- Clinical management, like AIS: coloscopy +/- endometrial biopsy.
May represent either:
- Endocervical cells, i.e. atypical endocervical cells (AEC).
- Endometrial cells, i.e. atypical endometrial cell (AEM).
Microscopic
Features:
- Atypical glandular cells:
- Cell cluster with cells with a diameter <= 2x intermediate cell nucleus.
- Some features of nuclear atypia, e.g. irregular nuclear membrane, granular chromatin, nuclear hyperchromasia, nuclear enlargement.
DDx:
- Adenocarcinoma in situ.
Uncommon stuff
Follicular cervicitis
General
- Uncommon. (???)
- Finding may be associated with Chlamydia trachomatis.[33]
Cytology
Features:[34]
- Discohesive clusters of small (lymphoid) cells with interspersed:
- Tingible-body macrophages.
- Plasma cells.
DDx:
- AGC - nuclei larger, more cohesive
Image:
Hematoidin crystal
General
- Rare.
- Benign.
- Associated with hemorrhage in pregnancy.[35]
Note:
- Overlap with crystalline bodies. (???)
- Crystalline bodies associated with pregnancy, and OCP use.[35]
Cytology
- Radiating crystal.
- Refractile.
- Classically golden-brown.
- +/-Surrounded by macrophages.
DDx:
- Sulfur granule of Actinomycetes.
Images:
- Cockleburr crystal (cytology-asc.com).[18]
- Cockleburr crystal (cytology-asc.com).
- Cockleburr crystal (cytology-asc.com).
{kind=link}
{kind=link}
{kind=link}
Carpet beetle larval parts
General
- Uncommon distinctive contaminant.[37]
- Fragment of a beetle.
- Benign.
Cytology
Features:
- Slender long structure - fern-like.
Note:
- One may have a complete insect.[38]
Image:
{kind=link}
Radiation changes in cervical cytology
General
- Radiation is used to treat cervical cancer.
Cytology
Features:[39]
- Architecture: single cells/groups.
- Cell borders: well-circumscribed.
- Cytoplasm: vacuolated, usually abundant.
- Nucleus:
- Enlarged nucleus - but normal NC ratio.
- No nuclear membrane irregularies.
- Chromatin: "smudgy".
- +/-Multinucleation.
DDx:
- LSIL.
- Vitamin B12 deficiency.
Images:
Cornflaking artifact
General
- Processing artifact - due to air under the cover slip.[40]
Cytology
Features:[40]
- Central brown discolourization in squamous cells.
Images:
{kind=link}
{kind=link}
Endocervical repair
General
- Benign.
Cytology
Features:
- Cluster of (2-dimensional) glandular cells with:
- Streaming (school of fish-appearance).
- Prominent nucleoli.
- Neutrophils.
Image:
Historical
Maturation index
- Abbreviated MI.
General
- Based on vaginal wall scrape.
Definition
.
Where:
- P = number of parabasal cells / 300 squamous cells * 100 %.
- I = number of intermediate cells / 300 squamous cells * 100 %.
- S = number of superficial cells / 300 squamous cells * 100 %.
Interpretation
Common patterns:
- Superficial predominant, no parabasal = high estrogen effect.
- Parabasal predominant, no superficial = atrophy.
Examples:
- 70 : 30 : 0 is an atrophic pattern.
- 0 : 30 : 70 is a high estrogen pattern.
Note:
- Significant inflammation distorts the result.
See also
References
- ↑ Half-day. 10 November 2008.
- ↑ SM. 14 January 2010.
- ↑ SM. 14 January 2010.
- ↑ GR. 4 February 2010.
- ↑ SM. 14 January 2010.
- ↑ URL: http://nih.techriver.net/view.php?patientId=78. Accessed on: 31 March 2012.
- ↑ Thrall MJ, Kjeldahl KS, Savik K, Gulbahce HE, Pambuccian SE (August 2005). "Significance of benign endometrial cells in papanicolaou tests from women aged >=40 years". Cancer 105 (4): 207-16. doi:10.1002/cncr.21156. PMID 15900572.
- ↑ DeMay, RM. The Art & Science of Cytopathology: Exfoliative Cytology. 1996. ISBN 0-89189-322-9. PP.116-7.
- ↑ URL: http://nih.techriver.net/view.php?patientId=221. Accessed on: 26 November 2011.
- ↑ DeMay, RM. The Art & Science of Cytopathology: Exfoliative Cytology. 1996. ISBN 0-89189-322-9. PP.116-7.
- ↑ 11.0 11.1 Slater, DN.; Rice, S.; Stewart, R.; Melling, SE.; Hewer, EM.; Smith, JH. (Aug 2005). "Proposed Sheffield quantitative criteria in cervical cytology to assist the diagnosis and grading of squamous intra-epithelial lesions, as some Bethesda system definitions require amendment.". Cytopathology 16 (4): 168-78. doi:10.1111/j.1365-2303.2005.00264.x. PMID 16048503. http://www3.interscience.wiley.com/journal/118661591/abstract?CRETRY=1&SRETRY=0.
- ↑ 12.0 12.1 12.2 12.3 12.4 12.5 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 446. ISBN 978-0781765275.
- ↑ UHN PCY50001.08 P.10.
- ↑ Sheffield, MV.; Simsir, A.; Talley, L.; Roberson, AJ.; Elgert, PA.; Chhieng, DC. (Mar 2003). "Interobserver variability in assessing adequacy of the squamous component in conventional cervicovaginal smears.". Am J Clin Pathol 119 (3): 367-73. PMID 12645338.
- ↑ GR. 4 February 2010.
- ↑ Doxtader EE, Elsheikh TM (January 2017). "Diagnosis of trichomoniasis in men by urine cytology". Cancer Cytopathol 125 (1): 55–59. doi:10.1002/cncy.21778. PMID 27636204.
- ↑ URL: http://en.wiktionary.org/wiki/-mycete#English. Accessed on: 14 September 2011.
- ↑ 18.0 18.1 18.2 URL: http://www.cytology-asc.com/cec/normal/index.htm#cockle. Accessed on: 10 April 2012.
- ↑ Scott TG, Smyth CJ, Keane CT (February 1987). "In vitro adhesiveness and biotype of Gardnerella vaginalis strains in relation to the occurrence of clue cells in vaginal discharges". Genitourinary medicine 63 (1): 47–53. PMC 1194007. PMID 3493202. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1194007/.
- ↑ 20.0 20.1 Polatti, F. (Feb 2012). "Bacterial vaginosis, Atopobium vaginae and nifuratel.". Curr Clin Pharmacol 7 (1): 36-40. PMID 22082330.
- ↑ Taylor-Robinson D (1984). "The bacteriology of Gardnerella vaginalis". Scand J Urol Nephrol Suppl 86: 41–55. PMID 6399409.
- ↑ Bigras, G.; Wilson, J.; Russell, L.; Johnson, G.; Morel, D.; Saddik, M. (Feb 2013). "Interobserver concordance in the assessment of features used for the diagnosis of cervical atypical squamous cells and squamous intraepithelial lesions (ASC-US, ASC-H, LSIL and HSIL).". Cytopathology 24 (1): 44-51. doi:10.1111/j.1365-2303.2011.00930.x. PMID 22007754.
- ↑ Chan, S. 26 April 2012.
- ↑ URL: http://www.cytology-asc.com/cec/endocx/. Accessed on: 13 September 2011.
- ↑ Belsley, NA.; Tambouret, RH.; Misdraji, J.; Muzikansky, A.; Russell, DK.; Wilbur, DC. (Apr 2008). "Cytologic features of endocervical glandular lesions: comparison of SurePath, ThinPrep, and conventional smear specimen preparations.". Diagn Cytopathol 36 (4): 232-7. doi:10.1002/dc.20782. PMID 18335553.
- ↑ Nucci, Marisa R.; Oliva, Esther (2009). Gynecologic Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 167. ISBN 978-0443069208.
- ↑ Duggan, MA. (Mar 2000). "Cytologic and histologic diagnosis and significance of controversial squamous lesions of the uterine cervix.". Mod Pathol 13 (3): 252-60. doi:10.1038/modpathol.3880046. PMID 10757336.
- ↑ URL: http://www.cap.org/apps/docs/proficiency_testing/CYP07600.pdf. Accessed on: 2 May 2012.
- ↑ Owens, CL.; Ali, SZ. (Dec 2005). "Atypical squamous cells in exfoliative urinary cytology: clinicopathologic correlates.". Diagn Cytopathol 33 (6): 394-8. doi:10.1002/dc.20344. PMID 16299739.
- ↑ URL: http://www.curran.pwp.blueyonder.co.uk/cytology.htm. Accessed on: 5 November 2012.
- ↑ Srodon, M.; Parry Dilworth, H.; Ronnett, BM. (Feb 2006). "Atypical squamous cells, cannot exclude high-grade squamous intraepithelial lesion: diagnostic performance, human papillomavirus testing, and follow-up results.". Cancer 108 (1): 32-8. doi:10.1002/cncr.21388. PMID 16136595.
- ↑ Chivukula, M.; Shidham, VB. (2006). "ASC-H in Pap test--definitive categorization of cytomorphological spectrum.". Cytojournal 3: 14. doi:10.1186/1742-6413-3-14. PMC 1524979. PMID 16686950. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1524979/.
- ↑ Hare, MJ.; Toone, E.; Taylor-Robinson, D.; Evans, RT.; Furr, PM.; Cooper, P.; Oates, JK. (Feb 1981). "Follicular cervicitis--colposcopic appearances and association with Chlamydia trachomatis.". Br J Obstet Gynaecol 88 (2): 174-80. PMID 6893939.
- ↑ Halford, JA. (Dec 2002). "Cytological features of chronic follicular cervicitis in liquid-based specimens: a potential diagnostic pitfall.". Cytopathology 13 (6): 364-70. PMID 12485172.
- ↑ 35.0 35.1 Minassian, H.; Schinella, R.; Reilly, JC.. "Crystalline bodies in cervical smears. Clinicocytologic correlation.". Acta Cytol 37 (2): 149-52. PMID 8465632.
- ↑ Zaharopoulos, P.; Wong, JY.; Keagy, N.. "Hematoidin crystals in cervicovaginal smears. Report of two cases.". Acta Cytol 29 (6): 1029-34. PMID 3866455.
- ↑ Bechtold, E.; Staunton, CE.; Katz, SS.. "Carpet beetle larval parts in cervical cytology specimens.". Acta Cytol 29 (3): 345-52. PMID 3859134.
- ↑ URL: http://www.cytology-asc.com/cec/normal/index.htm#dustmite. Accessed on: 10 April 2012.
- ↑ Gupta, S.; Mukherjee, K.; Gupta, YN.; Kumar, M. (Aug 1987). "Sequential radiation changes in cytology of vaginal smears in carcinoma of cervix uteri during radiotherapy.". Int J Gynaecol Obstet 25 (4): 303-8. PMID 2887465.
- ↑ 40.0 40.1 40.2 URL: http://www.cytology-asc.com/cec/normal/index.htm#cornflake. Accessed on: 10 April 2012.