Hemangioma
| Hemangioma | |
|---|---|
| Diagnosis in short | |
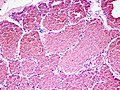
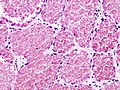
 Capillary hemangioma. H&E stain. | |
|
| |
| LM | channels lined by benign endothelium containing RBCs |
| Subtypes | soft tissue (capillary, cavernous, arteriovenous, venous, intramuscular, synovial), childhood (tufted, microvenular hemangioma, glomeruloid hemangioma, epithelioid hemangioma (see angiolymphoid hyperplasia with eosinophilia), targetoid hemosideric hemangioma, infantile hemangioma) |
| LM DDx | lymphangioma, angiokeratoma, lobular capillary hemangioma (pyogenic granuloma). |
| IHC | CD31 +ve, D2-40 -ve, GLUT-1 +ve -- juvenile hemangioma |
| Site | soft tissue, skin, liver, others |
|
| |
| Associated Dx | Castleman disease - for glomeruloid hemangioma |
| Syndromes | POEMS syndrome - for glomeruloid hemangioma |
|
| |
| Prevalence | common vascular lesion |
| Prognosis | benign |
| Hemangioma | |
|---|---|
| External resources | |
| EHVSC | 10172 |
Hemangioma is a very common benign vascular tumour.
General
Hemangiomas to remember - if you're only going remember a few:
- Glomeruloid, infantile, caverous, capillary, arteriovenous, venous and intramuscular.
Childhood
Common childhood hemangiomas:[2]
- Tufted - small clusters of blood vessels.
- Microvenular hemangioma.
- Glomeruloid hemangioma - associated with POEMS syndrome, Castleman disease.[3][4]
- Epithelioid hemangioma - see angiolymphoid hyperplasia with eosinophilia.
- Targetoid hemosideric hemangioma.
- Infantile hemangioma (AKA juvenile hemangioma[5]) - these tumours are GLUT-1 +ve. They tumours grow and then spontaneously regress.[6]
Soft tissue
Several types are seen in soft tissue:[7]
- Capillary.
- Cavernous.
- Arteriovenous.
- Venous.
- Intramuscular.
- Synovial.
Microscopic
Features:
- Channels lined by benign endothelium containing RBCs.
DDx:
- Lymphangioma.
- Angiokeratoma.
- Lobular capillary hemangioma (pyogenic granuloma).
Images
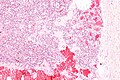
Capillary hemangioma - intermed. mag. (WC/Nephron)
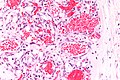
Capillary hemangioma - very high mag. (WC/Nephron)
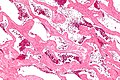
Cavernous liver hemangioma - intermed. mag. (WC/Nephron)
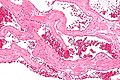
Cavernous liver hemangioma - high mag. (WC/Nephron)
Cavernous hemangioma. (WC/KGH)
Cavernous hemangioma. (WC/KGH)



.jpg)
.jpg)
www:
IHC
- CD31 +ve.
- D2-40 -ve.[8]
Juvenile hemangioma:[5]
- GLUT-1 +ve.
Sign out
SUBCUTANEOUS NECK LESION, LEFT, EXCISION: - CAVERNOUS HEMANGIOMA. - NEGATIVE FOR MALIGNANCY.
LESION, LEFT SIDE OF FACE, EXCISION: - CAPILLARY HEMANGIOMA. - NEGATIVE FOR MALIGNANCY.
Micro
The sections show hair-bearing skin with abundant small superficial vascular channels containing red blood cells. The endothelial cells of the vascular channels do not have atypia. No mitotic activity is appreciated. The overlying epidermis is unremarkable. Extensive solar elastosis is present. No nevus is identified.
See also
References
- ↑ Vokaer, B.; Kothonidis, K.; Delatte, P.; De Cooman, S.; Pector, JC.; Liberale, G.. "Should ruptured liver haemangioma be treated by surgery or by conservative means? A case report.". Acta Chir Belg 108 (6): 761-4. PMID 19241936.
- ↑ Prieto VG, Shea CR (July 1999). "Selected cutaneous vascular neoplasms. A review". Dermatol Clin 17 (3): 507–20, viii. PMID 10410855.
- ↑ Uthup S, Balachandran K, Ammal VA, et al. (August 2006). "Renal involvement in multicentric Castleman disease with glomeruloid hemangioma of skin and plasmacytoma". Am. J. Kidney Dis. 48 (2): e17–24. doi:10.1053/j.ajkd.2006.04.089. PMID 16860182.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 618. ISBN 978-0781765275.
- ↑ 5.0 5.1 North, PE.; Waner, M.; Mizeracki, A.; Mihm, MC. (Jan 2000). "GLUT1: a newly discovered immunohistochemical marker for juvenile hemangiomas.". Hum Pathol 31 (1): 11-22. PMID 10665907.
- ↑ Dadras, SS.; North, PE.; Bertoncini, J.; Mihm, MC.; Detmar, M. (Sep 2004). "Infantile hemangiomas are arrested in an early developmental vascular differentiation state.". Mod Pathol 17 (9): 1068-79. doi:10.1038/modpathol.3800153. PMID 15143338.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 602. ISBN 978-0781765275.
- ↑ Kahn, HJ.; Bailey, D.; Marks, A. (Apr 2002). "Monoclonal antibody D2-40, a new marker of lymphatic endothelium, reacts with Kaposi's sarcoma and a subset of angiosarcomas.". Mod Pathol 15 (4): 434-40. doi:10.1038/modpathol.3880543. PMID 11950918.