Dermatologic neoplasms
This article deals with dermatologic neoplasms. It includes dermatologic cancer, which can be deadly. Collectively, dermatologic cancers are the most common form of cancer.
An introduction to dermatopathy is found in the dermatopathology article. Non-malignant disease is covered in the non-malignant skin disease article.
The Big Three malignant
Basal cell carcinoma
- Abbreviated BCC.
General
- Very common.
- Sun exposed skin.
- Hair bearing area; tumour derived from hair follicle - a more appropriate name might be trichoblastic carcinoma.[1]
- Very rarely metastasizes:
- Dermatopathologists might see a couple in their career.
- There are only ~ 300 literature reports of metastatic BCC.[2]
Clinical
- Telangiectasias.
- Raised pearly nodule.
As part of a syndrome
- Nevoid basal cell carcinoma syndrome (NBCCS), AKA Gorlin syndrome.
- Bazex syndrome (X-linked).[3]
- Xeroderma pigmentosum.
Microscopic
- Basaloid cells - similar in appearance to basal cells:
- Moderate blue/grey cytoplasm.
- Dark ovoid/ellipsoid nucleus with uniform chromatin.
- Palisading of cells at the edge of the cell nests.
- Artefactual separation of cells (forming the nests) from the underlying stroma - key feature.
- Surrounded by blue (myxoid) stroma - key feature.
May be present:[5]
- Dystrophic calcification.
- Amyloid.
- Inflammation.
Notes:
- Palisading = the long axes of the cells are alined and the axes are perpendicular to the interface between the (basaloid cell) nests and stroma.
- Key elements in a list: Artefactual clefting (of nests), Basaloid cells, Peripheral palisading, Myxoid stroma.
- Memory device PAM: palisading, artefactual clefts, myxoid stroma.
DDx:
- Trichoepithelioma - no artefactual cleft.[4]
- Adenoid cystic carcinoma - no myxoid stroma, no peripheral palisading.
- Eccrine poroma - on palms & soles, BCC rarely found there.[6]
Images:
- WC:
- www:
{kind=link}
{kind=link}
Subtypes/unique features
- Many patterns exist.
- Recurrence higher in morpheaform (sclerosing), infiltrative, micronodular, and superficial patterns.[8]
- DG says the prognosis is similar for all BCC subtypes, except for sclerosing pattern and infiltrative pattern.[9]
The subtypes:[10]
| Pattern | Key histologic feature | Other histologic features | Other |
|---|---|---|---|
| Superficial pattern | connected to epidermis | ||
| Nodular pattern | nodules | partial detachment from epidermis | subgroup micronodular = nests equal size ~ 0.2 mm dia., >=25% of lesion |
| Morpheaform (sclerosing) pattern | stroma sclerosis | often seen with infiltrative pattern | |
| Infiltrative pattern | small irregular cell aggregates | often also sclerosing or morpheaform | |
| Fibroepitheliomatous pattern | cords and columns of basaloid cells | fibrous stroma | name of pattern comes from fibroepithelioma of Pinkus |
| Infundibulocystic pattern | small keratocysts (keratin cysts) | usu. small, often in cords | usu. indolent |
| Adenoidal pattern | cribriform / pseudoglandular arch. | myxoid stroma, peripheral palisading | DDx: adenoid cystic carcinoma |
Unique features/differentiation:[10]
| Differentiation / unique cell | Key histologic feature | Other histologic features | Other |
|---|---|---|---|
| Pigmented cells | any pattern can have pigmentation | pigment may be in malignant cell | DDx: collision lesion with melanocytic lesion |
| Squamous differentiation (metatypical BCC) | pink cytoplasm, keratinization | assoc. with ulceration/tumour recurrence | |
| Eccrine differentiation | focal duct formation | very rare, DDx: BCC engulfing sweat ducts | |
| Clear cells (Clear cell BCC) | clear cytoplasm | due to glycogen |
IHC
- CK5/6 +ve.
- Useful to assess margins... if very close.
- BerEP4 +ve.
- SCC usually negative.[11]
- CD10 +ve.
- Actin +ve.
Squamous cell carcinoma
General
Precursor:[12]
- Actinic keratosis (solar keratosis).
- Clinical: yellow-brown scaly, patches, sandpaper sensation.
Risk factors:[12]
- Sun exposure.
- Immune suppression (e.g. organ transplant recipients).
Notes:
- Keratoacanthoma.
- Some don't believe this entity exists.
- These people sign this entity as low grade squamous cell carcinoma, keratoacanthoma type.[13]
- Some don't believe this entity exists.
Microscopic
Bowen disease
Bowen disease is squamous cell carcinoma in situ of the skin.
- Its histomorphologic appearance may be similar to Paget disease, Toker cell hyperplasia and melanoma.
- IHC is used to separate the entities definitively.
Histologic DDx of Bowen disease:
- Benign Toker cell hyperplasia.
- Malignant melanoma.
- Eccrine carcinoma.
Images:
{kind=link}
{kind=link}
IHC
Bowen's disease panel:
- CK5/6 +ve.[14]
- Usu. -ve in Paget disease of the breast/Extramammary Paget disease.
- S100 -ve, HMB-45 -ve.
- Both typically +ve in melanoma.
- CEA -ve[15] (+ve in Paget disease of the breast/Extramammary Paget disease, -ve in Toker cells).
- CK7 -ve.
- Toker cells CK7 +ve.[16]
Melanoma
General
- Known as the great mimicker in pathology; it may look like many things.
Microscopic
Features:
- Classic appearance of melanoma:
- Loosely cohesive; mix of small nests of cells, single cells.
- Mixed of spindle and ovoid cell morphology.
- +/-Occasional large binucleated cells.
- Cytoplasm: brown pigment (melanin).
- Prominent (large) red nucleoli (like in serous carcinoma of the ovary).
- Marked nuclear pleomorphism - variation in cell size, shape & staining (like in serous carcinoma of the ovary).
- Nuclear pseudoinclusions (like in papillary thyroid carcinoma).
Less common malignant
Dermatofibrosarcoma protuberans
- Abbreviated DFSP.
General
- Dermal location.
- Destroys adnexal structures.
- Occasionally transforms to a (more aggressive) fibrosarcoma.[17]
Treatment:[18]
- Wide excision.
- May include imatinib (Gleevec).
Microscopic
Features:[18]
- Dermal spindle cell lesion with storiform pattern.
- Spokes of the wheel-pattern.
- Contains adipose tissue within the tumour -- key feature.
- Described as "honeycomb pattern" and "Swiss cheese pattern".
Notes:
- Adnexal structure within tumour are preserved -- this is unusual for a malignant tumour -- important.
Main DDx:
- Dermatofibroma - has entrapment of collagen bundles at the edge of the lesion.
DDx of storiform pattern:
- DFSP, dermatofibroma, solitary fibrous tumour, undifferentiated pleomorphic sarcoma.
Images:
{kind=link}
{kind=link}
IHC
Panel:[19]
- CD34 +ve.
- Factor XIIIa -ve.
- S100 -ve (screen for melanoma).
- Caldesmin -ve (screen for muscle differentiation).
- Beta-catenin. (???)
- MIB-1 (proliferation marker).
- Should not be confused with MIB1 a gene that regulates apoptosis.
Molecular
A characteristic translocation is seen:[22] t(17;22)(q22;q15) COLA1/PDGFB.
Cutaneous B-cell lymphoma
- Abbreviated CBCL.
General
- CBCL is less common than cutaneous T-cell lymphoma (CTCL).[23]
Microscopic
Features:
- Dermal lymphoid infiltrate.
- "Grenz zone" - space between the epidermis and the dermal infiltrate - key feature.
IHC
- B cell and T cell markers.
Cutaneous T-cell lymphoma
- Abbreviated CTCL.
General
- Mycosis fungoides - is a subtype (???).
- CTCL is more common than cutaneous B-cell lymphoma (CBCL).[24][25]
Stages - like Kaposi sarcoma:
- Patch.
- Plaque.
- Nodular.
Microscopic
- Atypical lymphocytes:
- Have folded "cerebriform" nuclei; Sezary-Lutzner cells.[26]
- Grouping:
DDx:
Images:
{kind=link}
{kind=link}
IHC
Key stain:
- CD4 +ve.[28]
Other stains:
- CD3 +ve.
- CD8 -ve.
- CD20 -ve (to r/o significant B cell population).
- CD30 -ve.
- CD5 +ve.
- CD7 -ve (often lost first in T cell lymphomas).
- Ki-67 high.
- CD56 -ve.
Lymphomatoid papulosis
General
- Rare.
- Benign behaviour.
Microscopic
Features:
- Dermal lymphocytosis.
- No epidermal lymphocytes.
- Focal nuclear atypia.
DDx:
IHC
- CD30 +ve.[29]
Merkel cell carcinoma
- Abbreviated MCC.
General
- Aggressive.
- Rare.
- Increased risk in the immunodeficient.
- Most caused by Merkel cell polyomavirus.[30]
General
Features:[31]
- Rare.
- Aggressive course/poor prognosis.
- Neuroendocrine-like.[32]
Etiology:
- Polyomavirus (?).[31]
- Immunocompromised/immunosuppressed (e.g. organ transplant recipients).
Microscopic
Features:[33]
- Neuroendocrine nuclear features - round nucleus, small nucleoli/no nucleolus, stippled chromatin - key feature.
- Typically medium size cells ~3x resting lymphocyte.
- May be small or large.
- Architecture: nests, sheets or trabeculae.
- Scant cytoplasm.
- Abundant mitoses.
- +/-Nuclear moulding.
DDx:
- Basal cell carcinoma - no stippled chromatin, less mitoses active.
- Cutaneous Ewing sarcoma - sorted-out with immunostains.
- Lymphoma.
- Metastatic small cell carcinoma.
- Other small round cell tumours.
Images:
- www:
- WC:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
IHC
Features:
- CK7 -ve.
- CK20 +ve (perinuclear dot-like).[34]
- CAM5.2 +ve (dot-like pattern).
Others:
- TTF-1 -ve.
Eccrine carcinoma
General
- Arises from the proximal sweat duct.
Microscopic
Features:
- Pleomorphic nuclei with nucleoli.
- Duct-like structures - key feature.
- Extends from dermis into epidermis (follows path of a benign sweat duct).
Notes:
- May resemble Extramammary Paget's disease/Paget's disease of the breast.
Kaposi sarcoma
- See Kaposi sarcoma.
Sebaceous carcinoma
General
- Malignant.
- May arise in a salivary gland.[35]
Notes:
- Sebaceous lesions (from benign to malignant): sebaceous hyperplasia, sebaceous adenoma, sebaceoma, sebaceous carcinoma.
Microscopic
Features:
- Nuclear atypia.
- Sebaceous differentiation:
- Abundant pale fluffy cytoplasm.
Image:
{kind=link}
Microcystic adnexal carcinoma
General
- Low-grade tumour.
- Adults.
Microscopic
Features:[37]
- Small basaloid cells - often forming small cystic spaces - key feature.
- Fibrotic stroma.
DDx:
- Sclerosing basal cell carcinoma.
- Desmoplastic trichoepithelioma.
- Infiltrative squamous cell carcinoma.
Image:
{kind=link}
Trichilemmal carcinoma
General
- Super rare.
- Not well-described.
Microscopic
Features:[38]
- Clear (glycogen-rich) cytoplasm in center of lesion.
- Peripheral palisading at edge of lesion - root sheath differentiation (hair follicle).
- Contiguous with hair follicle or assoc. with trichilemmoma.
DDx:
- Squamous cell carcinoma, clear cell variant.
- Basal cell carcinoma, clear cell variant.
- Trichilemmoma.
Intermediate
Atypical fibroxanthoma
- Abbreviated AFX.
General
- Typically head & neck region.[39]
- Thought to be related to pleomorphic undifferentiated sarcoma;[40] some say it is the same thing.[41]
Clinical:
- Rapid growth.
- Elderly.
- Good prognosis.[42]
Microscopic
Features:[43]
- Dermal lesion - key point.
- Marked nuclear atypia.
- Mitoses.
- Mulitnucleated cells.
- Foamy cytoplasm - key feature.
DDx:
- Melanoma.
- Pleomorphic undifferentiated sarcoma (MFH).
- Leiomyosarcoma.
- Sarcomatoid squamous carcinoma.
Notes:
- No Grenz zone. (???)
Image:
{kind=link}
IHC
Features:[43]
- S100 -ve (done to r/o melanoma).
- 34betaE12 -ve, p63 -ve (done to exclude SCC).
- Desmin -ve (done to r/o leiomyosarcoma).
Benign
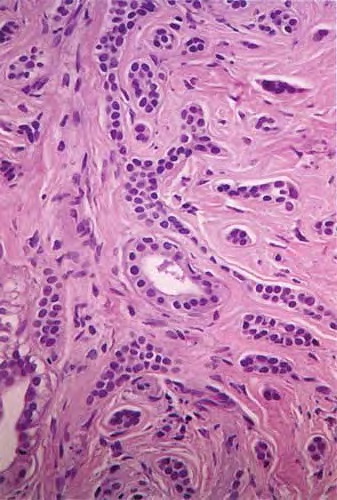
Syringoma
General
- Benign sweat duct tumour.
- Eccrine differentiation.
- Usually close to lower eyelid.[45]
Microscopic
Features:[46]
- Proliferation of benign ducts with lined by a bilayer (as in normal sweat ducts) with abnormal architecture:
- Tadpole like appearing ducts.
Images:
{kind=link}
Chondroid syringoma
- Used to be called mixed tumour of skin.[48]
General
- Mixed apocrine & eccrine tumour of skin, usu. in the head & neck[48], esp. nose and cheek.[49]
- May be in major and minor salivary glands.[49]
Microscopic
Features:
- Mix tumour with:[48]
- Epithelial component:
- Nests of cells with:
- Moderate dull eosinophilic cytoplasm.
- Round/ovoid nuclei with nucleoli.
- Nests of cells with:
- Mesenchymal component:
- Chondromyxoid stroma.
- Epithelial component:
Images:
{kind=link}
{kind=link}
Dermal cylindroma
General
- Benign skin lesion.
- Should not be confused with cylindroma (adenoid cystic carcinoma).
- May be related to ecrrine spiradenoma.[51][52]
Microscopic
Features:
- Nests that fit together like a jigsaw puzzle.
- The borders of the nests are opposed and undulate.
- Cells nests surrounded by hyaline (i.e. glassy, eosinophilic, acellular) material.
DDx:
Images:
{kind=link}
{kind=link}
Keratoacanthoma
- Abbreviated KA.
General
- Generally considered to be benign.
- Rare reports of metastases suggesting it may be a form of squamous cell carcinoma.[53]
Clinical
- May grow rapidly (weeks or months) then involute.
- Main DDx is squamous cell carcinoma.
- Exophytic lesion, well-circumscribed.
Microscopic
Features:[54]
- Expansion of stratum spinosum - pushing tongue-like downward growth of epidermis into the dermis.
- Keratin collection ("keratin plug") at the center of lesion-superficial aspect.
- Cells have glassy pink cytoplasm.
- Minimal/no nuclear atypia.
Note:
- Classically described as a "volcano lesion" with pale pink cells.
- May have features of regression - PMNs, fibrosis (???).
Image:
{kind=link}
Sebaceous adenoma
General
- Seen in Muir-Torre syndrome - a variant of Lynch syndrome (hereditary non-polyposis colon cancer).
Microscopic
Features:
- Abnormal sebaceous glands (pale fluffy cytoplasm):
- Increased basal epithelium.
- Multiple dilated glands - opening to the surface.
Images:
- www:
- WC:
{kind=link}
{kind=link}
Trichilemmoma
- May be spelled tricholemmoma.
General
- Benign neoplasm with features of the pilosebaceous follicular epithelium.[55]
- Associated with nevus sebaceous.[56]
- Muliple trichilemmomas associated with Cowden syndrome.[57]
Microscopic
Features:[57]
- Superficial dermal lesion contiguous with the epidermis:
- Core of lesion:
- Cuboidal cells with round nuclei, eosinophilic-clear cytoplasm.
- Periphery of lesion:
- Surrounded by hyaline band.
- Peripheral palisading.
- Core of lesion:
Images:
- Trichilemmoma - low mag. (cancer.gov).[58]
- Trichilemmoma - high mag. (cancer.gov).[58]
- Trichilemmoma (jhmi.edu).[59]
{kind=link}
{kind=link}
{kind=link}
DDx:
Eccrine poroma
- AKA nodular hidradenoma. (???)
General
- Benign tumour arising from the distal sweat duct.
- Erythematous - gross.
Microscopic
Features:[60]
- Broad sheets of basaloid cells containing ductal structures - key feature.
- Biphasic stroma:
- Edematous stroma.
- Sclerotic stroma.
- Moderate nuclear pleomorphism.
- +/-Occasional mitoses.
Notes:
- Area above gland appears crusted.
Images:
Trichoblastoma
- AKA trichoepithelioma.
- Trichoepithelioma is considered a superficial version of trichoblastoma; WHO lumps the two entities together.[61]
General
- Benign.
- Maligant counterpart of trichoepithelioma: trichilemmal carcinoma.
- May be familial:
- Multiple familial trichoepithelioma.[62]
- Brooke-Spiegler syndrome.
Microscopic
Features:[63]
- Well-circumscribed cell nest in the superficial dermis.
- Surrounding by a fibrous stroma.
- Basaloid cells with peripheral palisading.
- +/-Surround keratin-filled cysts.
- Fibroblasts-like cell aggregate, similar to a follicular papillae (papillary-mesenchymal body).
Notes:
- Very rarely an artefactual cleft - as in basal cell carcinoma.
Variants:
- Desmoplastic trichoblastoma.
DDx:
- Basal cell carcinoma - usu. mitoses, mucinous stroma and no papillary-mesenchymal bodies.
Images:
{kind=link}
{kind=link}
See also
References
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 389. ISBN 978-0443066542.
- ↑ Ting, PT.; Kasper, R.; Arlette, JP. (Jan 2005). "Metastatic basal cell carcinoma: report of two cases and literature review.". J Cutan Med Surg 9 (1): 10-5. doi:10.1007/s10227-005-0027-1. PMID 16208438.
- ↑ URL: http://emedicine.medscape.com/article/1101146-diagnosis. Accessed on: 6 May 2010.
- ↑ 4.0 4.1 Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1180-1. ISBN 978-1416031215.
- ↑ 5.0 5.1 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 390. ISBN 978-0443066542.
- ↑ Tadrous, Paul.J. Diagnostic Criteria Handbook in Histopathology: A Surgical Pathology Vade Mecum (1st ed.). Wiley. pp. 284. ISBN 978-0470519035.
- ↑ URL: http://missinglink.ucsf.edu/lm/DermatologyGlossary/basal_cell_carcinoma.html. Accessed on: 4 September 2011.
- ↑ Basal cell carcinoma. eMedicine. Prognosis section. URL: http://emedicine.medscape.com/article/276624-overview. Accessed on: 17 September 2011.
- ↑ DG. 14 September 2011.
- ↑ 10.0 10.1 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 392-5. ISBN 978-0443066542.
- ↑ Yu, L.; Galan, A.; McNiff, JM. (Oct 2009). "Caveats in BerEP4 staining to differentiate basal and squamous cell carcinoma.". J Cutan Pathol 36 (10): 1074-176. doi:10.1111/j.1600-0560.2008.01223.x. PMID 19187107.
- ↑ 12.0 12.1 Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1180. ISBN 978-1416031215.
- ↑ RS. 17 May 2010.
- ↑ RS. May 2010.
- ↑ URL: http://emedicine.medscape.com/article/1101235-workup#a0721. Accessed on: 2 September 2011.
- ↑ Nofech-Mozes, S.; Hanna, W.. "Toker cells revisited.". Breast J 15 (4): 394-8. doi:10.1111/j.1524-4741.2009.00743.x. PMID 19601945.
- ↑ Stacchiotti, S.; Pedeutour, F.; Negri, T.; Conca, E.; Marrari, A.; Palassini, E.; Collini, P.; Keslair, F. et al. (Oct 2011). "Dermatofibrosarcoma protuberans-derived fibrosarcoma: clinical history, biological profile and sensitivity to imatinib.". Int J Cancer 129 (7): 1761-72. doi:10.1002/ijc.25826. PMID 21128251.
- ↑ 18.0 18.1 Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1183. ISBN 978-1416031215.
- ↑ AP. May 2009.
- ↑ 20.0 20.1 Abenoza P, Lillemoe T (October 1993). "CD34 and factor XIIIa in the differential diagnosis of dermatofibroma and dermatofibrosarcoma protuberans". Am J Dermatopathol 15 (5): 429–34. PMID 7694515.
- ↑ 21.0 21.1 Goldblum JR, Tuthill RJ (April 1997). "CD34 and factor-XIIIa immunoreactivity in dermatofibrosarcoma protuberans and dermatofibroma". Am J Dermatopathol 19 (2): 147–53. PMID 9129699.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1249. ISBN 978-1416031215.
- ↑ URL: http://emedicine.medscape.com/article/1099540-overview. Accessed on: 24 August 2010.
- ↑ URL: http://emedicine.medscape.com/article/1099540-overview. Accessed on: 24 August 2010.
- ↑ URL: http://emedicine.medscape.com/article/1098342-overview. Accessed on: 24 August 2010.
- ↑ 26.0 26.1 Klatt, Edward C. (2006). Robbins and Cotran Atlas of Pathology (1st ed.). Saunders. pp. 385. ISBN 978-1416002741.
- ↑ URL: http://www.mdconsult.com/das/book/body/199872830-2/0/1709/I4-u1.0-B978-0-443-06694-8..50117-2--f2.fig. Accessed on: 6 May 2010.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1185. ISBN 978-1416031215.
- ↑ URL: http://path.upmc.edu/cases/case513/dx.html. Accessed on: 25 January 2012.
- ↑ Feng, H.; Shuda, M.; Chang, Y.; Moore, PS. (Feb 2008). "Clonal integration of a polyomavirus in human Merkel cell carcinoma.". Science 319 (5866): 1096-100. doi:10.1126/science.1152586. PMID 18202256.
- ↑ 31.0 31.1 Calder, KB.; Smoller, BR. (May 2010). "New insights into merkel cell carcinoma.". Adv Anat Pathol 17 (3): 155-61. doi:10.1097/PAP.0b013e3181d97836. PMID 20418670.
- ↑ Pulitzer, MP.; Amin, BD.; Busam, KJ. (May 2009). "Merkel cell carcinoma: review.". Adv Anat Pathol 16 (3): 135-44. doi:10.1097/PAP.0b013e3181a12f5a. PMID 19395876.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 491. ISBN 978-0781765275.
- ↑ Leech, SN.; Kolar, AJ.; Barrett, PD.; Sinclair, SA.; Leonard, N. (Sep 2001). "Merkel cell carcinoma can be distinguished from metastatic small cell carcinoma using antibodies to cytokeratin 20 and thyroid transcription factor 1.". J Clin Pathol 54 (9): 727-9. PMID 11533085.
- ↑ 35.0 35.1 URL: http://www.ispub.com/journal/the_internet_journal_of_otorhinolaryngology/volume_9_number_2_11/article/sebaceous_adenocarcinoma_of_the_parotid_gland_a_case_report_and_literature_review.html. Accessed on: 8 September 2011.
- ↑ 36.0 36.1 URL: http://www.dermaamin.com/site/histopathology-of-the-skin/65-m/1926-microcystic-adnexal-carcinoma-.html. Accessed on: 16 September 2011.
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 412. ISBN 978-0443066542.
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 399-400. ISBN 978-0443066542.
- ↑ URL: http://emedicine.medscape.com/article/1056204-overview. Accessed on 2 September 2011.
- ↑ Withers, AH.; Brougham, ND.; Barber, RM.; Tan, ST. (Jun 2011). "Atypical fibroxanthoma and malignant fibrous histiocytoma.". J Plast Reconstr Aesthet Surg. doi:10.1016/j.bjps.2011.05.004. PMID 21664889.
- ↑ DG. 16 September 2011.
- ↑ Beer, TW.; Drury, P.; Heenan, PJ. (Aug 2010). "Atypical fibroxanthoma: a histological and immunohistochemical review of 171 cases.". Am J Dermatopathol 32 (6): 533-40. doi:10.1097/DAD.0b013e3181c80b97. PMID 20526171.
- ↑ 43.0 43.1 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 521. ISBN 978-0443066542.
- ↑ Vandergriff, TW.; Reed, JA.; Orengo, IF. (2008). "An unusual presentation of atypical fibroxanthoma.". Dermatol Online J 14 (1): 6. PMID 18319023.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1177. ISBN 978-1416031215.
- ↑ URL: http://emedicine.medscape.com/article/1059871-diagnosis. Accessed on: 12 May 2010.
- ↑ Nosrati, N.; Coleman, NM.; Hsu, S. (2008). "Axillary syringomas.". Dermatol Online J 14 (4): 13. PMID 18627735.
- ↑ 48.0 48.1 48.2 Kumar, B. (Jan 2010). "Chondroid syringoma diagnosed by fine needle aspiration cytology.". Diagn Cytopathol 38 (1): 38-40. doi:10.1002/dc.21159. PMID 19693940.
- ↑ 49.0 49.1 Rauso, R.; Santagata, M.; Tartaro, G.; Filipi, M.; Colella, G.. "Chondroid syringoma: a rare tumor of orofacial region.". Minerva Stomatol 58 (7-8): 383-8. PMID 19633639.
- ↑ 50.0 50.1 URL: http://www.ispub.com/journal/the_internet_journal_of_dermatology/volume_7_number_2_23/article/cutaneous_mixed_tumor.html. Access on: 21 September 2011.
- ↑ Gerber, JE.; Descalzi, ME. (Feb 1983). "Eccrine spiradenoma and dermal cylindroma.". J Cutan Pathol 10 (1): 73-8. PMID 6302142.
- ↑ Lee, MW.; Kelly, JW. (Feb 1996). "Dermal cylindroma and eccrine spiradenoma.". Australas J Dermatol 37 (1): 48-9. PMID 8936072.
- ↑ Mandrell JC, Santa Cruz D (August 2009). "Keratoacanthoma: hyperplasia, benign neoplasm, or a type of squamous cell carcinoma?". Semin Diagn Pathol 26 (3): 150–63. PMID 20043514.
- ↑ Klatt, Edward C. (2006). Robbins and Cotran Atlas of Pathology (1st ed.). Saunders. pp. 378. ISBN 978-1416002741.
- ↑ URL: http://emedicine.medscape.com/article/1059940-overview. Accessed on: 2 September 2011.
- ↑ Baykal, C.; Buyukbabani, N.; Yazganoglu, KD.; Saglik, E. (Jan 2006). "[Tumors associated with nevus sebaceous].". J Dtsch Dermatol Ges 4 (1): 28-31. doi:10.1111/j.1610-0387.2006.05855.x. PMID 16503928.
- ↑ 57.0 57.1 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 386. ISBN 978-0443066542.
- ↑ 58.0 58.1 URL: http://ccr.cancer.gov/staff/gallery.asp?profileid=12822. Accessed on: 2 September 2011.
- ↑ URL: http://dermatlas.med.jhmi.edu/derm/indexDisplay.cfm?ImageID=667496720. Accessed on: 2 September 2011.
- ↑ URL: http://www.pathconsultddx.com/pathCon/diagnosis?pii=S1559-8675(06)70190-5. Accessed on: 2 July 2010.
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 383. ISBN 978-0443066542.
- ↑ Salhi, A.; Bornholdt, D.; Oeffner, F.; Malik, S.; Heid, E.; Happle, R.; Grzeschik, KH. (Aug 2004). "Multiple familial trichoepithelioma caused by mutations in the cylindromatosis tumor suppressor gene.". Cancer Res 64 (15): 5113-7. doi:10.1158/0008-5472.CAN-04-0307. PMID 15289313.
- ↑ URL: http://emedicine.medscape.com/article/1060049-workup#a0723. Accessed on: 31 August 2011.