Difference between revisions of "Non-small cell lung carcinoma"
| (6 intermediate revisions by the same user not shown) | |||
| Line 39: | Line 39: | ||
In the clinical context, it is often referred to as '''non-small cell lung cancer'''; this ignores the fact that not all non-small cell lung cancer fits into the [[carcinoma]] category. | In the clinical context, it is often referred to as '''non-small cell lung cancer'''; this ignores the fact that not all non-small cell lung cancer fits into the [[carcinoma]] category. | ||
''Poorly differentiated carcinoma of the lung'' and ''poorly differentiated lung carcinoma'' redirect to this article. | ''Poorly differentiated carcinoma of the lung'', ''non-small cell carcinoma'' and ''poorly differentiated lung carcinoma'' redirect to this article. | ||
==General== | ==General== | ||
| Line 67: | Line 67: | ||
*[[Malignant melanoma]]. | *[[Malignant melanoma]]. | ||
*Other poorly differentiated neoplasms | *Other poorly differentiated neoplasms | ||
===Grading=== | |||
*''NSCC-NOS'', ''NSCC favour adenocarcinoma'', ''NSCC favour SCC'' are grade 4. | |||
Note: | |||
*In a large series of patients, there is no statistical difference in survival been grade 3 and grade 4.<ref name=pmid16678584>{{Cite journal | last1 = Sun | first1 = Z. | last2 = Aubry | first2 = MC. | last3 = Deschamps | first3 = C. | last4 = Marks | first4 = RS. | last5 = Okuno | first5 = SH. | last6 = Williams | first6 = BA. | last7 = Sugimura | first7 = H. | last8 = Pankratz | first8 = VS. | last9 = Yang | first9 = P. | title = Histologic grade is an independent prognostic factor for survival in non-small cell lung cancer: an analysis of 5018 hospital- and 712 population-based cases. | journal = J Thorac Cardiovasc Surg | volume = 131 | issue = 5 | pages = 1014-20 | month = May | year = 2006 | doi = 10.1016/j.jtcvs.2005.12.057 | PMID = 16678584 }}</ref> | |||
===Images=== | ===Images=== | ||
| Line 83: | Line 89: | ||
Note: | Note: | ||
* | *If immunostains favour adenocarcinoma or squamous cell carcinoma, the case should be sign as ''favour adenocarcinoma'' or ''favour squamous cell carcinoma'', see ''Sloan-Kettering algorithm'' below and ''Sign out'' section. | ||
===Adenocarcinoma versus squamous carcinoma=== | ===Adenocarcinoma versus squamous carcinoma=== | ||
| Line 116: | Line 122: | ||
|- | |- | ||
| Non-small cell carcinoma, favour adenocarcinoma | | Non-small cell carcinoma, favour adenocarcinoma | ||
| TTF-1 or napsin +ve | | [[TTF-1]] or napsin +ve | ||
|- | |- | ||
| Non-small cell carcinoma, favour squamous cell carcinoma | | Non-small cell carcinoma, favour squamous cell carcinoma | ||
| p40 or p63 +ve | | [[p40]] or [[p63]] +ve | ||
|- | |- | ||
| Non-small cell carcinoma-not otherwise specified | | Non-small cell carcinoma-not otherwise specified | ||
Latest revision as of 17:01, 18 June 2017
Non-small cell lung carcinoma, abbreviated NSCLC, is a malignant epithelial neoplasm of the lung that is not small cell carcinoma of the lung.
| Non-small cell lung carcinoma | |
|---|---|
| Diagnosis in short | |
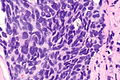
 Non-small cell lung carcinoma. H&E stain. | |
|
| |
| Synonyms | large cell carcinoma (term discouraged in the context of biopsies & FNAs) |
| Subtypes | NSCC favour adenocarcinoma, NSCC favour squamous cell carcinoma, NSCC-not otherwise specified |
| LM DDx | lung adenocarcinoma, lung squamous carcinoma, lung small cell carcinoma, poorly differentiated metastatic carcinoma, other poorly differentiated neoplasms |
| IHC | pankeratin +ve, CD56 -ve, chromogranin A -ve, synaptophysin -ve, TTF-1 +ve/-ve, p63 +ve/-ve |
| Staging | lung cancer staging |
| Site | lung - see lung tumours |
|
| |
| Clinical history | no history of malignancy or no suspicion of recurrence |
| Symptoms | +/-hemopytsis, +/-dyspnea |
| Prevalence | uncommon |
| Radiology | not suggestive of metastatic disease |
| Prognosis | usually poor |
| Clin. DDx | other lung tumours |
| Treatment | surgery if feasible |
It is umbrella term that includes squamous cell carcinoma of lung, adenocarcinoma of the lung and adenosquamous carcinoma of the lung.[1]
It is also known as large cell carcinoma; however, usage of large cell carcinoma is discouraged in the context of lung biopsies and lung cytopathology specimens.[2]
In the clinical context, it is often referred to as non-small cell lung cancer; this ignores the fact that not all non-small cell lung cancer fits into the carcinoma category.
Poorly differentiated carcinoma of the lung, non-small cell carcinoma and poorly differentiated lung carcinoma redirect to this article.
General
- Non-small cell lung carcinoma can be considered a waffle diagnosis and as such its use should be limited.
- It is preferable to be more specific if this is possible, i.e. call adenocarcinoma or squamous cell carcinoma.
- Historically, it was sufficient to differentiate between small cell and non-small cell carcinomas, as the treatment for all non-small cell lung carcinomas was the same.
- Small cell carcinoma is typically considered non-surgical disease; thus, non-small cell carcinoma or poorly differentiated carcinoma, as a diagnosis, is less likely to exclude surgery as an option.
Clinical:
- Radiologic findings should not be suggestive of a metastasis.
- No history of malignancy or no suspicion of recurrence.
- +/-Hemopytsis.
- +/-Dyspnea.
Microscopic
Features:
- Typically large cells with abundant cytoplasm.
- +/-Nucleoli.
- No stippled chromatin.
DDx:
- Squamous cell carcinoma of the lung.
- Adenocarcinoma of the lung.
- Small cell carcinoma of the lung.
- Large cell variant of small cell carcinoma of the lung.
- Lung metastasis - imaging suggestive of a metastasis or a history of malignancy.
- Malignant melanoma.
- Other poorly differentiated neoplasms
Grading
- NSCC-NOS, NSCC favour adenocarcinoma, NSCC favour SCC are grade 4.
Note:
- In a large series of patients, there is no statistical difference in survival been grade 3 and grade 4.[3]
Images
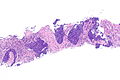
NSCLC - low mag. (WC)
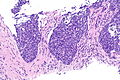
NSCLC - intermed mag. (WC)
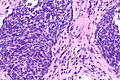
NSCLC - high mag. (WC)
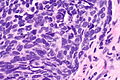
NSCLC - very high mag. (WC)
NSCLC - very high mag. (WC)




IHC
Features:
- Lack of staining with neuroendocrine markers (chromogranin A -ve, synaptophysin -ve, CD56 -ve).
- Keratins +ve.
Note:
- If immunostains favour adenocarcinoma or squamous cell carcinoma, the case should be sign as favour adenocarcinoma or favour squamous cell carcinoma, see Sloan-Kettering algorithm below and Sign out section.
Adenocarcinoma versus squamous carcinoma
Memorial Sloan-Kettering algorithm - Rekhtman et al.:[4]
| TTF-1\p63 | p63 -ve (0% of cells) | p63 +ve <50% of cells | p63 +ve >=50% of cells |
|---|---|---|---|
| TTF-1 +ve >=50% of cells | Adenocarcinoma | Adenocarcinoma | Adenocarcinoma |
| TTF-1 +ve <50% of cells | Adenocarcinoma | Adenocarcinoma | Squamous carcinoma |
| TTF-1 -ve (0% of cells) | Adenocarcinoma | CK5/6 to determine | Squamous carcinoma |
Sign out
International consensus terminology - Travis et al.:[2]
| Diagnosis | Stains |
|---|---|
| Non-small cell carcinoma, favour adenocarcinoma | TTF-1 or napsin +ve |
| Non-small cell carcinoma, favour squamous cell carcinoma | p40 or p63 +ve |
| Non-small cell carcinoma-not otherwise specified | -ve NE stains, -ve SCC stains, -ve adenoca stains |
Not otherwise specified
Lung, Left Lower Lobe, Core Biopsy: - NON-SMALL CELL CARCINOMA-NOT OTHERWISE SPECIFIED, see comment. COMMENT: The tumour stains as follows: POSITIVE: EMA, AE1/AE3. NEGATIVE: TTF-1, chromogranin A, synaptophysin, CD56, CD45, CK5/6, p63. The morphology would be compatible with small cell carcinoma or basaloid squamous cell carcinoma. The neuroendocrine markers (chromogranin A, synaptophysin, CD56) and the squamous markers (p63, CK5/6) are negative; thus, the tumour is not further classified.
Favour squamous
Lung, Left Upper Lobe, Core Biopsy: - NON-SMALL CELL CARCINOMA, favour squamous cell carcinoma, see comment. Comment: The tumour stains as follows: POSITIVE: AE1/AE3, CK5/6, CK7. NEGATIVE: TTF-1, napsin A, p63, CDX2, CK20, S-100. EGFR/ALK testing has been ordered. The immunostains favour squamous cell carcinoma.
See also
References
- ↑ Song, Z.; Lin, B.; Shao, L.; Zhang, Y. (Sep 2013). "Therapeutic efficacy of gefitinib and erlotinib in patients with advanced lung adenosquamous carcinoma.". J Chin Med Assoc 76 (9): 481-5. doi:10.1016/j.jcma.2013.05.007. PMID 23769878.
- ↑ 2.0 2.1 Travis, WD.; Brambilla, E.; Noguchi, M.; Nicholson, AG.; Geisinger, K.; Yatabe, Y.; Ishikawa, Y.; Wistuba, I. et al. (May 2013). "Diagnosis of lung cancer in small biopsies and cytology: implications of the 2011 International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification.". Arch Pathol Lab Med 137 (5): 668-84. doi:10.5858/arpa.2012-0263-RA. PMID 22970842.
- ↑ Sun, Z.; Aubry, MC.; Deschamps, C.; Marks, RS.; Okuno, SH.; Williams, BA.; Sugimura, H.; Pankratz, VS. et al. (May 2006). "Histologic grade is an independent prognostic factor for survival in non-small cell lung cancer: an analysis of 5018 hospital- and 712 population-based cases.". J Thorac Cardiovasc Surg 131 (5): 1014-20. doi:10.1016/j.jtcvs.2005.12.057. PMID 16678584.
- ↑ Rekhtman, N.; Ang, DC.; Sima, CS.; Travis, WD.; Moreira, AL. (Oct 2011). "Immunohistochemical algorithm for differentiation of lung adenocarcinoma and squamous cell carcinoma based on large series of whole-tissue sections with validation in small specimens.". Mod Pathol 24 (10): 1348-59. doi:10.1038/modpathol.2011.92. PMID 21623384.