Difference between revisions of "Mesothelial cytopathology"
| (16 intermediate revisions by the same user not shown) | |||
| Line 7: | Line 7: | ||
A general [[differential diagnosis]] of pleural effusion is given in the ''[[pleural effusion]]'' article. | A general [[differential diagnosis]] of pleural effusion is given in the ''[[pleural effusion]]'' article. | ||
''Pleural fluid'' | ''Pleural fluid'', ''pleural cytopathology'', ''peritoneal fluid'', and ''peritoneal cytopathology'' redirect to here. | ||
=Specimen types= | =Overview= | ||
*[[Sensitivity]] moderate for malignancy (60%).<ref name=pmid>{{Cite journal | last1 = Karoo | first1 = RO. | last2 = Lloyd | first2 = TD. | last3 = Garcea | first3 = G. | last4 = Redway | first4 = HD. | last5 = Robertson | first5 = GS. | title = How valuable is ascitic cytology in the detection and management of malignancy? | journal = Postgrad Med J | volume = 79 | issue = 931 | pages = 292-4 | month = May | year = 2003 | doi = | PMID = 12782778 }}</ref> | |||
===Specimen types=== | |||
*'''Wash''', e.g. ''peritoneal wash'': expect sheets of (benign squamous) cells. | *'''Wash''', e.g. ''peritoneal wash'': expect sheets of (benign squamous) cells. | ||
*'''Spontaneous''', e.g. ''pleural fluid'': usually no large sheets. | *'''Spontaneous''', e.g. ''pleural fluid'': usually no large sheets. | ||
Note: | Note: | ||
This distinction is important as ''wash'' specimens may have pseudopapillae. | This distinction is important as ''wash'' specimens may have pseudopapillae. | ||
=Approach= | ===Approach=== | ||
Look for: | Look for: | ||
#Two cell populations. | #Two cell populations. | ||
| Line 34: | Line 37: | ||
#Small cells with high [[NC ratio]]. | #Small cells with high [[NC ratio]]. | ||
==Features of malignancy== | ===Features of malignancy=== | ||
Strongly suggestive of malignancy: | Strongly suggestive of malignancy: | ||
*3-D clusters. | *3-D clusters. | ||
| Line 45: | Line 48: | ||
*High NC ratio. | *High NC ratio. | ||
=Differential diagnosis= | ===Differential diagnosis=== | ||
*[[Adenocarcinoma]] not otherwise specified (NOS) - most common. | *[[Adenocarcinoma]] not otherwise specified (NOS) - most common. | ||
*Reactive mesothelium. | *Reactive mesothelium. | ||
| Line 60: | Line 63: | ||
*[[Small cell carcinoma]]. | *[[Small cell carcinoma]]. | ||
===Peritoneal cavity specific=== | ====Peritoneal cavity specific==== | ||
*[[Hepatocellular carcinoma]] (HCC) may be associated with ascites... but it is rarely positive for malignant cells.<ref name=Ref_APBR679>{{Ref APBR|679}}</ref> | *[[Hepatocellular carcinoma]] (HCC) may be associated with ascites... but it is rarely positive for malignant cells.<ref name=Ref_APBR679>{{Ref APBR|679}}</ref> | ||
**HCC in ascites fluid is super rare -- ''I haven't seen a case''.<ref>SB. 8 January 2010.</ref> | **HCC in ascites fluid is super rare -- ''I haven't seen a case''.<ref>SB. 8 January 2010.</ref> | ||
=Normal mesothelium= | =Normal mesothelium= | ||
===General=== | |||
Often seen in the context of: | |||
*Gynecologic surgeries - done to exclude malignancy. | |||
*Taps for ascites. | |||
===Cytology=== | |||
Features:<ref name=Ref_APBR674>{{Ref APBR|674}}</ref> | Features:<ref name=Ref_APBR674>{{Ref APBR|674}}</ref> | ||
*"Window" or "space" between attached cells (due to microvilli). | *"Window" or "space" between attached cells (due to microvilli). | ||
| Line 84: | Line 93: | ||
=Reactive mesothelium= | =Reactive mesothelium= | ||
===General=== | |||
*May be due to any number of causes. | |||
*Can be severe in the context of [[chronic renal failure|(peritoneal) dialysis]].<ref name=pmid2323293>{{Cite journal | last1 = Selvaggi | first1 = SM. | last2 = Migdal | first2 = S. | title = Cytologic features of atypical mesothelial cells in peritoneal dialysis fluid. | journal = Diagn Cytopathol | volume = 6 | issue = 1 | pages = 22-6 | month = | year = 1990 | doi = | PMID = 2323293 }}</ref> | |||
===Cytology=== | |||
:''See [[Mesothelial_cytopathology#Malignant_mesothelioma|mesothelioma]]''. | |||
====Images==== | |||
<gallery> | |||
Image: Peritoneal fluid - post-DC insertion -- high mag.jpg | PF - high mag. (WC) | |||
Image: Peritoneal fluid - post-DC insertion -- very high mag.jpg | PF - very high mag. (WC) | |||
Image: Peritoneal fluid - post-DC insertion - alt -- very high mag.jpg | PF - very high mag. (WC) | |||
</gallery> | |||
===Sign out=== | ===Sign out=== | ||
<pre> | <pre> | ||
| Line 133: | Line 155: | ||
===Cytology=== | ===Cytology=== | ||
Features: | Features: | ||
*Lupus erythematosus cells, usually abbreviated ''LE | *Lupus erythematosus cells, usually abbreviated ''[[LE cell]]s'':<ref>URL:[http://www.tabers.com/tabersonline/ub/view/Tabers/143167/34/L_E__cell http://www.tabers.com/tabersonline/ub/view/Tabers/143167/34/L_E__cell]. Accessed on: 12 April 2012.</ref> | ||
**Pink blobs (representing a denatured nuclei) - phagocytosed by | **Pink blobs (representing a denatured nuclei) - phagocytosed by a [[neutrophil]].<ref>URL: [http://library.med.utah.edu/WebPath/IMMHTML/IMM008.html http://library.med.utah.edu/WebPath/IMMHTML/IMM008.html]. Accessed on: 12 April 2012.</ref> | ||
Image: | Image: | ||
| Line 208: | Line 230: | ||
===IHC=== | ===IHC=== | ||
* | *[[Calretinin]] +ve. | ||
*WT-1 +ve. | *WT-1 +ve. | ||
*[[D2-40]] +ve. | *[[D2-40]] +ve. | ||
*[[TTF-1]] -ve. | *[[TTF-1]] -ve. | ||
*CEA -ve. | *CEA -ve. | ||
*[[p63]] -ve.<ref name=pmid18064689>{{Cite journal | last1 = Pu | first1 = RT. | last2 = Pang | first2 = Y. | last3 = Michael | first3 = CW. | title = Utility of WT-1, p63, MOC31, mesothelin, and cytokeratin (K903 and CK5/6) immunostains in differentiating adenocarcinoma, squamous cell carcinoma, and malignant mesothelioma in effusions. | journal = Diagn Cytopathol | volume = 36 | issue = 1 | pages = 20-5 | month = Jan | year = 2008 | doi = 10.1002/dc.20747 | PMID = 18064689 }}</ref> | |||
==Adenocarcinoma== | ==Adenocarcinoma== | ||
| Line 251: | Line 274: | ||
Image: Adenocarcinoma - pleural fluid 3 - TTF-1 -- very high mag.jpg | Adenocarcinoma - TTF-1 - very high mag. (WC) | Image: Adenocarcinoma - pleural fluid 3 - TTF-1 -- very high mag.jpg | Adenocarcinoma - TTF-1 - very high mag. (WC) | ||
</gallery> | </gallery> | ||
===IHC=== | |||
Breast: | |||
*ER +ve/-ve. | |||
*Calretinin -ve. | |||
Colon: | |||
*CK20 +ve. | |||
*CDX2 +ve. | |||
*Calretinin -ve. | |||
Lung: | |||
*TTF-1 +ve. | |||
*Calretinin -ve. | |||
==Colorectal adenocarcinoma== | ==Colorectal adenocarcinoma== | ||
| Line 306: | Line 343: | ||
===IHC=== | ===IHC=== | ||
*WT-1 +ve. | *WT-1 +ve. | ||
*CA-125 +ve. | *[[CA-125]] +ve. | ||
*D2-40 +ve. | *D2-40 +ve. | ||
Latest revision as of 16:40, 15 May 2017


Mesothelial cytopathology is a large part of cytopathology. The article deals with cytopathology specimens from spaces lined with mesothelium, i.e. it deals with pericardial fluid, peritoneal fluid and pleural fluid.
An introduction to cytopathology is in the cytopathology article.
A general differential diagnosis of pleural effusion is given in the pleural effusion article.
Pleural fluid, pleural cytopathology, peritoneal fluid, and peritoneal cytopathology redirect to here.
Overview
- Sensitivity moderate for malignancy (60%).[1]
Specimen types
- Wash, e.g. peritoneal wash: expect sheets of (benign squamous) cells.
- Spontaneous, e.g. pleural fluid: usually no large sheets.
Note: This distinction is important as wash specimens may have pseudopapillae.
Approach
Look for:
- Two cell populations.
- Large dark objects.
- Boerner's red flags.
Boerner's red flags:
- 3-D clusters.
- Doublet & triplets common.
- Quads-to-Quints - sweat breaks-out.
- Sextuplets... very nervous.
- "Busy" slide:
- Nuclear pleomorphism.
- Too many "intermediate cells".
- Mitoses - 1-2/slide is "many".
- Vacuolated cytoplasm.
- Small cells with high NC ratio.
Features of malignancy
Strongly suggestive of malignancy:
- 3-D clusters.
- Large clusters.
- Highly cellularity.
- Irregular nucleoli.
- Group pleomorphism.
May be suggestive:
- High NC ratio.
Differential diagnosis
- Adenocarcinoma not otherwise specified (NOS) - most common.
- Reactive mesothelium.
- Malignant mesothelioma.
- Serous carcinoma.
- Lymphoma.
Less common:
- Squamous carcinoma.
- Rheumatoid pleuritis.
- Systemic lupus erythematosus pleurisy.
- Endosalpingiosis.
- Endometriosis.
- Small cell carcinoma.
Peritoneal cavity specific
- Hepatocellular carcinoma (HCC) may be associated with ascites... but it is rarely positive for malignant cells.[2]
- HCC in ascites fluid is super rare -- I haven't seen a case.[3]
Normal mesothelium
General
Often seen in the context of:
- Gynecologic surgeries - done to exclude malignancy.
- Taps for ascites.
Cytology
Features:[4]
- "Window" or "space" between attached cells (due to microvilli).
- Cytoplasmic blebs.
- Bleb = "drop" of cytoplasm at cell periphery.
- +/-Multinucleated.
- Variable size (normal).
- Nucleoli (in reactive cells).
Note - abnormal features:
- Large clusters of cells, e.g. 150+ micrometres.
Images

Peritoneal wash - benign mesothelial cells in sheets (WC)

Peritoneal wash - benign mesothelial cells in sheets - high mag. (WC)
Pairs of mesothelial cells with an intercellular window. (WC)


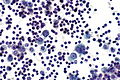
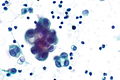
Reactive mesothelium
General
- May be due to any number of causes.
- Can be severe in the context of (peritoneal) dialysis.[5]
Cytology
- See mesothelioma.
Images

PF - high mag. (WC)

PF - very high mag. (WC)

PF - very high mag. (WC)



Sign out
Pleural Fluid, Right, Thoracentesis: - Negative for malignant cells. - Reactive mesothelial cells present in a background of abundant lymphocytes. Comment: Additional sampling should be considered within the clinical context.
Specific diagnoses - benign
Eosinophilic pleuritis
General
This has a large DDx:
- Trauma with air in the pleural cavity.
- Repeated tap in the context of pneumothorax.
- Pulmonary infarct.
- Pneumonia.
- Parasitic infections.
- Hodgkin lymphoma.
- Idiopathic - most common cause.
Cytology
Features:
- Eosinophils >10%.
Rheumatoid pleuritis
General
- History of rheumatoid arthritis.
- Cytologic appearance considered to be pathognomonic.[6]
Cytology
Features:[6]
- Large (single) multinucleated cells - classically spindled.
- May have epithelioid morphology.
- Necrotic debris - fluffy orange-to-blue crap.
Note:
- Necrotizing granulomatous inflammation.
Systemic lupus erythematosus pleurisy
- AKA systemic lupus erythematosus pleuritis.
General
- Not common.
- Distinctive cytology.
Cytology
Features:
- Lupus erythematosus cells, usually abbreviated LE cells:[7]
- Pink blobs (representing a denatured nuclei) - phagocytosed by a neutrophil.[8]
Image:
Specific diagnoses - malignant
Malignant mesothelioma
General
- Can be challenging to diagnose.
- NC ratio may be normal in mesothelioma.
- Large NC ratios may be seen in reactive mesothelial cells.
- Focal hyperchromasia is seen in reactive mesothelial cells.
- Focal macronucleoli are seen in reactive mesothelial cells.
Cytopathology
Features:[9]
- Nuclear membrane irregularies (rare).
- Hyperchromasia - diffuse.
- 3-D clusters of cells (strongly suggestive).
- Clusters of cells with "knobby" border; border is hobnail-like.
- Large clusters of cells; >10 cells in a cluster (rare in benign).
- Large NC ratio (common - not specific).
- Gigantic cells; cells 2X+ neighbouring mesothelial cell (uncommon - but strong).
- Nucleoli:
- Macronucleoli - must be widespread (not common - strong).
- Multiple nucleoli.
- Irregular nucleoli (strong).
Notes:
- Single cells/small clusters - suggestive of mesothelioma vs. serous carcinoma. (???)
Mesothelioma versus reactive mesothelium:[9]
| Characteristic | Reactive mesothelial cells | Mesothelioma |
|---|---|---|
| Architecture | Flat sheets | 3-D groups |
| Group size | Small, <10 cells | Large, >10 cells |
| Nuclear atypia - see Note 1. | +/-Hyperchromasia, +/-focal atypia | +/-Widespread atypia |
| Large cells | +/-Yes | No |
| Nucleoli | Common - small, focal large | +/-Large widespread, +/-multiple |
Note 1:
- Best assessed on single cells.
Images
www:

Mesothelioma - 1 (WC)

Mesothelioma - 2 (WC)


IHC
- Calretinin +ve.
- WT-1 +ve.
- D2-40 +ve.
- TTF-1 -ve.
- CEA -ve.
- p63 -ve.[10]
Adenocarcinoma
General
- Diagnosis represent a large number of distinct entities - see adenocarcinoma NOS.
Cytology
Adenocarcinoma in fluid - features:[11]
- Classically large morules (clusters of cells that are heaped/are "3-dimensional"), known as cannonballs, with "community borders".
- "Community border" = smooth, low surface area border; should be differentiated from a "knobby" border seen in mesothelioma.
- Intracytoplasmic "lumens"/inclusions (think lobular carcinoma).
DDx of cannonballs:[11]
- Breast.
- Ovary.
- Lung.
- GI.
Images
Case 1

Adenocarcinoma - high mag. (WC)
Adenocarcinoma - very high mag. (WC)



Lung adenocarcinoma - high mag. (WC)

Lung adenocarcinoma - very high mag. (WC)

Lung adenocarcinoma - high mag. (WC)

Lung adenocarcinoma - very high mag. (WC)



Case 2
Adenocarcinoma - high mag. (WC)
Adenocarcinoma - very high mag. (WC)
Adenocarcinoma - very high mag. (WC)

Adenocarcinoma - TTF-1 - high mag. (WC)

Adenocarcinoma - TTF-1 - very high mag. (WC)





IHC
Breast:
- ER +ve/-ve.
- Calretinin -ve.
Colon:
- CK20 +ve.
- CDX2 +ve.
- Calretinin -ve.
Lung:
- TTF-1 +ve.
- Calretinin -ve.
Colorectal adenocarcinoma
- May be abbreviated CRA.
General
- Cytology may be distinctive.
Cytology
Features:
- Cannonballs (non-specific).
- Suggestive of CRA:[11]
- Pseudostratified cells.
- Columnar cells.
Note:
- See adenocarcinoma section above for other types of adenocarcinoma.
Serous carcinoma
General
- S. Boerner believes one can and ought to separate adenocarcinoma from serous carcinoma.
Microscopic
Features:
- Large nucleoli.[12]
- Cilia.[13]
- Abnormal architecture:[14]
- Large clusters of cells / micropapillae (?).
- Nuclear overlap.
- +/-True papillae.[15]
Note 1 - classic features of serous (see gynecologic pathology article):
- Columnar cells.
- Cilia.
- Papillae.
- Psammoma bodies.
DDx of serous carcinoma (found in ascites fluid):
- Cervix.
- Endometrium.
- Intravacuolar neutrophils are erroneously believed to be indicative of this.[15]
- Uterine tube.
- Ovary.
- Primary peritoneal.
Images
www:

Serous carcinoma - cytology - low mag. (WC)
Serous carcinoma - histology - high mag. (WC)


IHC
- WT-1 +ve.
- CA-125 +ve.
- D2-40 +ve.
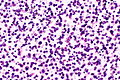
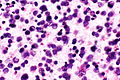
Lymphoma
General
- Can only be reasonably certain for large cell lymphomas, e.g. DLBCL.
- The diagnosis of small cell lymphomas relies on architecture and immunostains.
Cytology
Features:
- Dyscohesive cells ~2x a resting lymphocyte - usually with scant blue cytoplasm.
DDx:
Images
Lymphoma - intermed. mag.

Lymphoma - high mag.
Lymphoma - very high mag.
Lymphoma - high mag.
Lymphoma - very high mag.





See also
References
- ↑ Karoo, RO.; Lloyd, TD.; Garcea, G.; Redway, HD.; Robertson, GS. (May 2003). "How valuable is ascitic cytology in the detection and management of malignancy?". Postgrad Med J 79 (931): 292-4. PMID 12782778.
- ↑ Lefkowitch, Jay H. (2006). Anatomic Pathology Board Review (1st ed.). Saunders. pp. 679. ISBN 978-1416025887.
- ↑ SB. 8 January 2010.
- ↑ Lefkowitch, Jay H. (2006). Anatomic Pathology Board Review (1st ed.). Saunders. pp. 674. ISBN 978-1416025887.
- ↑ Selvaggi, SM.; Migdal, S. (1990). "Cytologic features of atypical mesothelial cells in peritoneal dialysis fluid.". Diagn Cytopathol 6 (1): 22-6. PMID 2323293.
- ↑ 6.0 6.1 Naylor, B.. "The pathognomonic cytologic picture of rheumatoid pleuritis. The 1989 Maurice Goldblatt Cytology award lecture.". Acta Cytol 34 (4): 465-73. PMID 2197838.
- ↑ URL:http://www.tabers.com/tabersonline/ub/view/Tabers/143167/34/L_E__cell. Accessed on: 12 April 2012.
- ↑ URL: http://library.med.utah.edu/WebPath/IMMHTML/IMM008.html. Accessed on: 12 April 2012.
- ↑ 9.0 9.1 Tadrous, Paul.J. Diagnostic Criteria Handbook in Histopathology: A Surgical Pathology Vade Mecum (1st ed.). Wiley. pp. 359-60. ISBN 978-0470519035.
- ↑ Pu, RT.; Pang, Y.; Michael, CW. (Jan 2008). "Utility of WT-1, p63, MOC31, mesothelin, and cytokeratin (K903 and CK5/6) immunostains in differentiating adenocarcinoma, squamous cell carcinoma, and malignant mesothelioma in effusions.". Diagn Cytopathol 36 (1): 20-5. doi:10.1002/dc.20747. PMID 18064689.
- ↑ 11.0 11.1 11.2 Lefkowitch, Jay H. (2006). Anatomic Pathology Board Review (1st ed.). Saunders. pp. 675. ISBN 978-1416025887.
- ↑ Kuebler, DL.; Nikrui, N.; Bell, DA.. "Cytologic features of endometrial papillary serous carcinoma.". Acta Cytol 33 (1): 120-6. PMID 2916358.
- ↑ http://www3.interscience.wiley.com/journal/112702002/abstract?CRETRY=1&SRETRY=0
- ↑ Weir, MM.; Bell, DA. (Oct 2001). "Cytologic identification of serous neoplasms in peritoneal fluids.". Cancer 93 (5): 309-18. PMID 11668465.
- ↑ 15.0 15.1 Boerner, S. 12 January 2010.