Difference between revisions of "Non-small cell lung carcinoma"
(fix wierd term) |
|||
| (49 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
''' | {{ Infobox diagnosis | ||
| Name = {{PAGENAME}} | |||
| Image = Non-small cell lung carcinoma -- high mag.jpg | |||
| Width = | |||
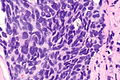
| Caption = Non-small cell lung carcinoma. [[H&E stain]]. | |||
| Synonyms = large cell carcinoma (term discouraged in the context of biopsies & FNAs) | |||
| Micro = | |||
| Subtypes = NSCC favour adenocarcinoma, NSCC favour squamous cell carcinoma, NSCC-not otherwise specified | |||
| LMDDx = [[lung adenocarcinoma]], [[squamous cell carcinoma of the lung|lung squamous carcinoma]], [[lung small cell carcinoma]], poorly differentiated metastatic [[carcinoma]], other poorly differentiated neoplasms | |||
| Stains = | |||
| IHC = pankeratin +ve, [[CD56]] -ve, chromogranin A -ve, synaptophysin -ve, [[TTF-1]] +ve/-ve, [[p63]] +ve/-ve | |||
| EM = | |||
| Molecular = | |||
| IF = | |||
| Gross = | |||
| Grossing = | |||
| Staging = [[lung cancer staging]] | |||
| Site = [[lung]] - see ''[[lung tumours]]'' | |||
| Assdx = | |||
| Syndromes = | |||
| Clinicalhx = no history of malignancy or no suspicion of recurrence | |||
| Signs = | |||
| Symptoms = +/-hemopytsis, +/-dyspnea | |||
| Prevalence = uncommon | |||
| Bloodwork = | |||
| Rads = not suggestive of metastatic disease | |||
| Endoscopy = | |||
| Prognosis = usually poor | |||
| Other = | |||
| ClinDDx = other [[lung tumours]] | |||
| Tx = surgery if feasible | |||
}} | |||
'''Non-small cell lung carcinoma''', abbreviated '''NSCLC''', is a [[carcinoma|malignant epithelial neoplasm]] of the [[lung]] that is ''not'' [[small cell carcinoma of the lung]]. | |||
It can be | It is umbrella term that includes [[squamous cell carcinoma of lung]], [[adenocarcinoma of the lung]] and [[adenosquamous carcinoma of the lung]].<ref>{{Cite journal | last1 = Song | first1 = Z. | last2 = Lin | first2 = B. | last3 = Shao | first3 = L. | last4 = Zhang | first4 = Y. | title = Therapeutic efficacy of gefitinib and erlotinib in patients with advanced lung adenosquamous carcinoma. | journal = J Chin Med Assoc | volume = 76 | issue = 9 | pages = 481-5 | month = Sep | year = 2013 | doi = 10.1016/j.jcma.2013.05.007 | PMID = 23769878 }}</ref> | ||
It is also known as '''large cell carcinoma'''; however, usage of ''large cell carcinoma'' is discouraged in the context of lung biopsies and [[pulmonary cytopathology|lung cytopathology]] specimens.<ref name=pmid22970842>{{Cite journal | last1 = Travis | first1 = WD. | last2 = Brambilla | first2 = E. | last3 = Noguchi | first3 = M. | last4 = Nicholson | first4 = AG. | last5 = Geisinger | first5 = K. | last6 = Yatabe | first6 = Y. | last7 = Ishikawa | first7 = Y. | last8 = Wistuba | first8 = I. | last9 = Flieder | first9 = DB. | title = Diagnosis of lung cancer in small biopsies and cytology: implications of the 2011 International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification. | journal = Arch Pathol Lab Med | volume = 137 | issue = 5 | pages = 668-84 | month = May | year = 2013 | doi = 10.5858/arpa.2012-0263-RA | PMID = 22970842 }}</ref> | |||
In the clinical context, it is often referred to as '''non-small cell lung cancer'''; this ignores the fact that not all non-small cell lung cancer fits into the [[carcinoma]] category. | |||
''Poorly differentiated carcinoma of the lung'', ''non-small cell carcinoma'' and ''poorly differentiated lung carcinoma'' redirect to this article. | |||
==General== | |||
*''Non-small cell lung carcinoma'' can be considered a [[waffle diagnosis]] and as such its use should be limited. | |||
**It is preferable to be more specific if this is possible, i.e. call ''adenocarcinoma'' or ''squamous cell carcinoma''. | |||
*Historically, it was sufficient to differentiate between [[small cell carcinoma of the lung|small cell]] and non-small cell carcinomas, as the treatment for all non-small cell lung carcinomas was the same. | |||
*''Small cell carcinoma'' is typically considered non-surgical disease; thus, ''non-small cell carcinoma'' or ''poorly differentiated carcinoma'', as a diagnosis, is less likely to exclude surgery as an option. | |||
Clinical: | |||
*Radiologic findings should not be suggestive of a metastasis. | |||
*No history of malignancy or no suspicion of recurrence. | |||
*+/-Hemopytsis. | |||
*+/-Dyspnea. | |||
==Microscopic== | |||
Features: | |||
*Typically large cells with abundant cytoplasm. | |||
*+/-[[Nucleoli]]. | |||
*No stippled chromatin. | |||
DDx: | |||
*[[Squamous cell carcinoma of the lung]]. | |||
*[[Adenocarcinoma of the lung]]. | |||
*[[Small cell carcinoma of the lung]]. | |||
*Large cell variant of [[small cell carcinoma of the lung]]. | |||
*[[Lung metastasis]] - imaging suggestive of a metastasis or a history of malignancy. | |||
*[[Malignant melanoma]]. | |||
*Other poorly differentiated neoplasms | |||
===Grading=== | |||
*''NSCC-NOS'', ''NSCC favour adenocarcinoma'', ''NSCC favour SCC'' are grade 4. | |||
Note: | |||
*In a large series of patients, there is no statistical difference in survival been grade 3 and grade 4.<ref name=pmid16678584>{{Cite journal | last1 = Sun | first1 = Z. | last2 = Aubry | first2 = MC. | last3 = Deschamps | first3 = C. | last4 = Marks | first4 = RS. | last5 = Okuno | first5 = SH. | last6 = Williams | first6 = BA. | last7 = Sugimura | first7 = H. | last8 = Pankratz | first8 = VS. | last9 = Yang | first9 = P. | title = Histologic grade is an independent prognostic factor for survival in non-small cell lung cancer: an analysis of 5018 hospital- and 712 population-based cases. | journal = J Thorac Cardiovasc Surg | volume = 131 | issue = 5 | pages = 1014-20 | month = May | year = 2006 | doi = 10.1016/j.jtcvs.2005.12.057 | PMID = 16678584 }}</ref> | |||
===Images=== | |||
<gallery> | |||
Image: Non-small cell lung carcinoma -- low mag.jpg | NSCLC - low mag. (WC) | |||
Image: Non-small cell lung carcinoma -- intermed mag.jpg | NSCLC - intermed mag. (WC) | |||
Image: Non-small cell lung carcinoma -- high mag.jpg | NSCLC - high mag. (WC) | |||
Image: Non-small cell lung carcinoma -- very high mag.jpg | NSCLC - very high mag. (WC) | |||
Image: Non-small cell lung carcinoma - alt -- very high mag.jpg | NSCLC - very high mag. (WC) | |||
</gallery> | |||
==IHC== | |||
Features: | |||
*Lack of staining with [[neuroendocrine markers]] (chromogranin A -ve, synaptophysin -ve, CD56 -ve). | |||
*Keratins +ve. | |||
Note: | |||
*If immunostains favour adenocarcinoma or squamous cell carcinoma, the case should be sign as ''favour adenocarcinoma'' or ''favour squamous cell carcinoma'', see ''Sloan-Kettering algorithm'' below and ''Sign out'' section. | |||
===Adenocarcinoma versus squamous carcinoma=== | |||
Memorial Sloan-Kettering algorithm - Rekhtman ''et al.'':<ref name=pmid21623384>{{Cite journal | last1 = Rekhtman | first1 = N. | last2 = Ang | first2 = DC. | last3 = Sima | first3 = CS. | last4 = Travis | first4 = WD. | last5 = Moreira | first5 = AL. | title = Immunohistochemical algorithm for differentiation of lung adenocarcinoma and squamous cell carcinoma based on large series of whole-tissue sections with validation in small specimens. | journal = Mod Pathol | volume = 24 | issue = 10 | pages = 1348-59 | month = Oct | year = 2011 | doi = 10.1038/modpathol.2011.92 | PMID = 21623384 }}</ref> | |||
{| class="wikitable sortable" | |||
! TTF-1\p63 | |||
! p63 -ve (0% of cells) | |||
! p63 +ve <50% of cells | |||
! p63 +ve >=50% of cells | |||
|- | |||
| TTF-1 +ve >=50% of cells | |||
| [[adenocarcinoma of the lung|Adenocarcinoma]] | |||
| Adenocarcinoma | |||
| Adenocarcinoma | |||
|- | |||
| TTF-1 +ve <50% of cells | |||
| Adenocarcinoma | |||
| Adenocarcinoma | |||
| [[Lung SCC|Squamous carcinoma]] | |||
|- | |||
| TTF-1 -ve (0% of cells) | |||
| Adenocarcinoma | |||
| CK5/6 to determine | |||
| Squamous carcinoma | |||
|} | |||
==Sign out== | |||
International consensus terminology - Travis ''et al''.:<ref name=pmid22970842>{{Cite journal | last1 = Travis | first1 = WD. | last2 = Brambilla | first2 = E. | last3 = Noguchi | first3 = M. | last4 = Nicholson | first4 = AG. | last5 = Geisinger | first5 = K. | last6 = Yatabe | first6 = Y. | last7 = Ishikawa | first7 = Y. | last8 = Wistuba | first8 = I. | last9 = Flieder | first9 = DB. | title = Diagnosis of lung cancer in small biopsies and cytology: implications of the 2011 International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification. | journal = Arch Pathol Lab Med | volume = 137 | issue = 5 | pages = 668-84 | month = May | year = 2013 | doi = 10.5858/arpa.2012-0263-RA | PMID = 22970842 }}</ref> | |||
{| class="wikitable sortable" | |||
! Diagnosis | |||
! Stains | |||
|- | |||
| Non-small cell carcinoma, favour adenocarcinoma | |||
| [[TTF-1]] or napsin +ve | |||
|- | |||
| Non-small cell carcinoma, favour squamous cell carcinoma | |||
| [[p40]] or [[p63]] +ve | |||
|- | |||
| Non-small cell carcinoma-not otherwise specified | |||
| -ve NE stains, -ve SCC stains, -ve adenoca stains | |||
|} | |||
===Not otherwise specified=== | |||
<pre> | |||
Lung, Left Lower Lobe, Core Biopsy: | |||
- NON-SMALL CELL CARCINOMA-NOT OTHERWISE SPECIFIED, see comment. | |||
COMMENT: | |||
The tumour stains as follows: | |||
POSITIVE: EMA, AE1/AE3. | |||
NEGATIVE: TTF-1, chromogranin A, synaptophysin, CD56, CD45, CK5/6, p63. | |||
The morphology would be compatible with small cell carcinoma or basaloid | |||
squamous cell carcinoma. | |||
The neuroendocrine markers (chromogranin A, synaptophysin, CD56) and the squamous | |||
markers (p63, CK5/6) are negative; thus, the tumour is not further classified. | |||
</pre> | |||
===Favour squamous=== | |||
<pre> | |||
Lung, Left Upper Lobe, Core Biopsy: | |||
- NON-SMALL CELL CARCINOMA, favour squamous cell carcinoma, see comment. | |||
Comment: | |||
The tumour stains as follows: | |||
POSITIVE: AE1/AE3, CK5/6, CK7. | |||
NEGATIVE: TTF-1, napsin A, p63, CDX2, CK20, S-100. | |||
EGFR/ALK testing has been ordered. | |||
The immunostains favour squamous cell carcinoma. | |||
</pre> | |||
==See also== | |||
*[[Lung tumours]]. | |||
*[[SUV]]. | |||
*[[Sarcomatoid carcinoma of the lung]]. | |||
==References== | |||
{{Reflist|1}} | |||
[[Category:Pulmonary pathology]] | [[Category:Pulmonary pathology]] | ||
[[Category:Diagnosis]] | |||
Latest revision as of 17:01, 18 June 2017
| Non-small cell lung carcinoma | |
|---|---|
| Diagnosis in short | |
 Non-small cell lung carcinoma. H&E stain. | |
|
| |
| Synonyms | large cell carcinoma (term discouraged in the context of biopsies & FNAs) |
| Subtypes | NSCC favour adenocarcinoma, NSCC favour squamous cell carcinoma, NSCC-not otherwise specified |
| LM DDx | lung adenocarcinoma, lung squamous carcinoma, lung small cell carcinoma, poorly differentiated metastatic carcinoma, other poorly differentiated neoplasms |
| IHC | pankeratin +ve, CD56 -ve, chromogranin A -ve, synaptophysin -ve, TTF-1 +ve/-ve, p63 +ve/-ve |
| Staging | lung cancer staging |
| Site | lung - see lung tumours |
|
| |
| Clinical history | no history of malignancy or no suspicion of recurrence |
| Symptoms | +/-hemopytsis, +/-dyspnea |
| Prevalence | uncommon |
| Radiology | not suggestive of metastatic disease |
| Prognosis | usually poor |
| Clin. DDx | other lung tumours |
| Treatment | surgery if feasible |
Non-small cell lung carcinoma, abbreviated NSCLC, is a malignant epithelial neoplasm of the lung that is not small cell carcinoma of the lung.
It is umbrella term that includes squamous cell carcinoma of lung, adenocarcinoma of the lung and adenosquamous carcinoma of the lung.[1]
It is also known as large cell carcinoma; however, usage of large cell carcinoma is discouraged in the context of lung biopsies and lung cytopathology specimens.[2]
In the clinical context, it is often referred to as non-small cell lung cancer; this ignores the fact that not all non-small cell lung cancer fits into the carcinoma category.
Poorly differentiated carcinoma of the lung, non-small cell carcinoma and poorly differentiated lung carcinoma redirect to this article.
General
- Non-small cell lung carcinoma can be considered a waffle diagnosis and as such its use should be limited.
- It is preferable to be more specific if this is possible, i.e. call adenocarcinoma or squamous cell carcinoma.
- Historically, it was sufficient to differentiate between small cell and non-small cell carcinomas, as the treatment for all non-small cell lung carcinomas was the same.
- Small cell carcinoma is typically considered non-surgical disease; thus, non-small cell carcinoma or poorly differentiated carcinoma, as a diagnosis, is less likely to exclude surgery as an option.
Clinical:
- Radiologic findings should not be suggestive of a metastasis.
- No history of malignancy or no suspicion of recurrence.
- +/-Hemopytsis.
- +/-Dyspnea.
Microscopic
Features:
- Typically large cells with abundant cytoplasm.
- +/-Nucleoli.
- No stippled chromatin.
DDx:
- Squamous cell carcinoma of the lung.
- Adenocarcinoma of the lung.
- Small cell carcinoma of the lung.
- Large cell variant of small cell carcinoma of the lung.
- Lung metastasis - imaging suggestive of a metastasis or a history of malignancy.
- Malignant melanoma.
- Other poorly differentiated neoplasms
Grading
- NSCC-NOS, NSCC favour adenocarcinoma, NSCC favour SCC are grade 4.
Note:
- In a large series of patients, there is no statistical difference in survival been grade 3 and grade 4.[3]
Images
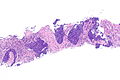
NSCLC - low mag. (WC)
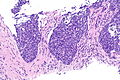
NSCLC - intermed mag. (WC)
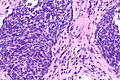
NSCLC - high mag. (WC)
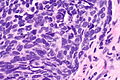
NSCLC - very high mag. (WC)
NSCLC - very high mag. (WC)




IHC
Features:
- Lack of staining with neuroendocrine markers (chromogranin A -ve, synaptophysin -ve, CD56 -ve).
- Keratins +ve.
Note:
- If immunostains favour adenocarcinoma or squamous cell carcinoma, the case should be sign as favour adenocarcinoma or favour squamous cell carcinoma, see Sloan-Kettering algorithm below and Sign out section.
Adenocarcinoma versus squamous carcinoma
Memorial Sloan-Kettering algorithm - Rekhtman et al.:[4]
| TTF-1\p63 | p63 -ve (0% of cells) | p63 +ve <50% of cells | p63 +ve >=50% of cells |
|---|---|---|---|
| TTF-1 +ve >=50% of cells | Adenocarcinoma | Adenocarcinoma | Adenocarcinoma |
| TTF-1 +ve <50% of cells | Adenocarcinoma | Adenocarcinoma | Squamous carcinoma |
| TTF-1 -ve (0% of cells) | Adenocarcinoma | CK5/6 to determine | Squamous carcinoma |
Sign out
International consensus terminology - Travis et al.:[2]
| Diagnosis | Stains |
|---|---|
| Non-small cell carcinoma, favour adenocarcinoma | TTF-1 or napsin +ve |
| Non-small cell carcinoma, favour squamous cell carcinoma | p40 or p63 +ve |
| Non-small cell carcinoma-not otherwise specified | -ve NE stains, -ve SCC stains, -ve adenoca stains |
Not otherwise specified
Lung, Left Lower Lobe, Core Biopsy: - NON-SMALL CELL CARCINOMA-NOT OTHERWISE SPECIFIED, see comment. COMMENT: The tumour stains as follows: POSITIVE: EMA, AE1/AE3. NEGATIVE: TTF-1, chromogranin A, synaptophysin, CD56, CD45, CK5/6, p63. The morphology would be compatible with small cell carcinoma or basaloid squamous cell carcinoma. The neuroendocrine markers (chromogranin A, synaptophysin, CD56) and the squamous markers (p63, CK5/6) are negative; thus, the tumour is not further classified.
Favour squamous
Lung, Left Upper Lobe, Core Biopsy: - NON-SMALL CELL CARCINOMA, favour squamous cell carcinoma, see comment. Comment: The tumour stains as follows: POSITIVE: AE1/AE3, CK5/6, CK7. NEGATIVE: TTF-1, napsin A, p63, CDX2, CK20, S-100. EGFR/ALK testing has been ordered. The immunostains favour squamous cell carcinoma.
See also
References
- ↑ Song, Z.; Lin, B.; Shao, L.; Zhang, Y. (Sep 2013). "Therapeutic efficacy of gefitinib and erlotinib in patients with advanced lung adenosquamous carcinoma.". J Chin Med Assoc 76 (9): 481-5. doi:10.1016/j.jcma.2013.05.007. PMID 23769878.
- ↑ 2.0 2.1 Travis, WD.; Brambilla, E.; Noguchi, M.; Nicholson, AG.; Geisinger, K.; Yatabe, Y.; Ishikawa, Y.; Wistuba, I. et al. (May 2013). "Diagnosis of lung cancer in small biopsies and cytology: implications of the 2011 International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification.". Arch Pathol Lab Med 137 (5): 668-84. doi:10.5858/arpa.2012-0263-RA. PMID 22970842.
- ↑ Sun, Z.; Aubry, MC.; Deschamps, C.; Marks, RS.; Okuno, SH.; Williams, BA.; Sugimura, H.; Pankratz, VS. et al. (May 2006). "Histologic grade is an independent prognostic factor for survival in non-small cell lung cancer: an analysis of 5018 hospital- and 712 population-based cases.". J Thorac Cardiovasc Surg 131 (5): 1014-20. doi:10.1016/j.jtcvs.2005.12.057. PMID 16678584.
- ↑ Rekhtman, N.; Ang, DC.; Sima, CS.; Travis, WD.; Moreira, AL. (Oct 2011). "Immunohistochemical algorithm for differentiation of lung adenocarcinoma and squamous cell carcinoma based on large series of whole-tissue sections with validation in small specimens.". Mod Pathol 24 (10): 1348-59. doi:10.1038/modpathol.2011.92. PMID 21623384.