|
|
| (38 intermediate revisions by 2 users not shown) |
| Line 15: |
Line 15: |
| *Shiny serosal surface. | | *Shiny serosal surface. |
| **No exudate. | | **No exudate. |
| *Small diameter. | | *Normal diameter. |
| | **6.6 +/- 1.5 mm -- based on CT.<ref name=pmid21344807>{{Cite journal | last1 = Charoensak | first1 = A. | last2 = Pongpornsup | first2 = S. | last3 = Suthikeeree | first3 = W. | title = Wall thickness and outer diameter of the normal appendix in adults using 64 slices multidetector CT. | journal = J Med Assoc Thai | volume = 93 | issue = 12 | pages = 1437-42 | month = Dec | year = 2010 | doi = | PMID = 21344807 }}</ref> |
|
| |
|
| ===Microscopic=== | | ===Microscopic=== |
| Features: | | Features: |
| *+/-Lymphoid hyperplasia. | | *+/-Lymphoid hyperplasia - mucosa or submucosa. |
| | *Normal colorectal-type mucosa. |
| | *Fatty submucosa. |
| | *Benign smooth muscle. |
| | *Serosa. |
|
| |
|
| Negatives: | | Negatives: |
| *No neutrophils in the muscularis propria. | | *No [[neutrophil]]s in the muscularis propria. |
| *No lesion in appendiceal tip. | | *No lesion in appendiceal tip. |
| *No serosal inflammation. | | *No serosal inflammation ([[periappendicitis]]). |
| *No organisms in the appendiceal lumen, e.g. [[Enterobius vermicularis]]. | | *No organisms in the appendiceal lumen, e.g. [[Enterobius vermicularis]]. |
|
| |
|
| ==Negative appendectomy==
| | DDx: |
| ===General===
| | *[[Adenovirus appendicitis]]. |
| *Common.
| | *[[Cryptosporidiosis]]. |
| *Use for quality control among general surgeons.{{fact}} | | *Mild colitis. |
| | |
| ===Gross===
| |
| See ''[[normal vermiform appendix]]''.
| |
| | |
| ===Microscopic===
| |
| See ''[[normal vermiform appendix]]''.
| |
| | |
| Notes:
| |
| *Should be ''[[submitted in total]]''. | |
|
| |
|
| ===Sign out=== | | ===Sign out=== |
| <pre> | | <pre> |
| VERMIFORM APPENDIX, APPENDECTOMY: | | VERMIFORM APPENDIX WITHIN NORMAL LIMITS. |
| - APPENDIX NEGATIVE FOR ACUTE APPENDICITIS AND NEGATIVE FOR ACUTE PERIAPPENDICITIS.
| |
| </pre> | | </pre> |
|
| |
|
| <pre>
| | Note: |
| VERMIFORM APPENDIX, APPENDECTOMY:
| | *This is for a normal appendix within a larger operation. The article ''[[negative appendectomy]]'' deals with a normal appearing appendix that was removed for presumed appendicitis. |
| - APPENDIX WITH LYMPHOID HYPERPLASIA AND FOCAL MUCOSAL EROSIONS.
| |
| - NEGATIVE FOR ACUTE APPENDICITIS.
| |
| - NEGATIVE FOR ACUTE PERIAPPENDICITIS.
| |
| </pre>
| |
|
| |
|
| ====Micro==== | | ==Negative appendectomy== |
| The sections show appendiceal wall with focal mucosa erosions and several intraluminal
| | {{Main|Negative appendectomy}} |
| neutrophil clusters. Lymphoid hyperplasia is present. Fecal material is present within
| | An appendectomy done for presumed [[acute appendicitis]] that is pathologically within normal limits |
| the lumen of the appendix.
| |
| | |
| There are no neutrophils within the muscularis propria. There is no serositis. There is
| |
| no distortion of the crypt architecture. No granulomas are identified. No cryptitis is
| |
| identified.
| |
|
| |
|
| =Inflammatory pathologies= | | =Inflammatory pathologies= |
| ==Acute appendicitis== | | ==Acute appendicitis== |
| ===General===
| | {{Main|Acute appendicitis}} |
| *Bread 'n butter of general surgery.
| |
| *Interesting factoid: appendicitis is considered protective against [[ulcerative colitis]].<ref name=pmid19685454>{{Cite journal | last1 = Beaugerie | first1 = L. | last2 = Sokol | first2 = H. | title = Appendicitis, not appendectomy, is protective against ulcerative colitis, both in the general population and first-degree relatives of patients with IBD. | journal = Inflamm Bowel Dis | volume = | issue = | pages = | month = Aug | year = 2009 | doi = 10.1002/ibd.21064 | PMID = 19685454 }}</ref><ref name=pmid19273505>{{Cite journal | last1 = Timmer | first1 = A. | last2 = Obermeier | first2 = F. | title = Reduced risk of ulcerative colitis after appendicectomy. | journal = BMJ | volume = 338 | issue = | pages = b225 | month = | year = 2009 | doi = | PMID = 19273505 }}</ref>
| |
| | |
| Short clinical DDx:
| |
| *GI tract:
| |
| **Symptomatic [[Meckel diverticulum]].
| |
| **Epiploic appendagitis.
| |
| *Gynecologic tract:
| |
| **Ectopic pregnancy.
| |
| **Ruptured ovarian cyst.
| |
| **Ovarian torsion.
| |
| ***Pelvic inflammatory disease.
| |
| | |
| ===Gross===
| |
| Features:
| |
| *Serosal surface dull.
| |
| *May be perforated (best determined on gross).
| |
| *+/-Fibrinous exudate.
| |
| | |
| Note:
| |
| *Normal diameter of appendix (based on CT): 6.6 +/- 1.5 mm.<ref name=pmid21344807>{{Cite journal | last1 = Charoensak | first1 = A. | last2 = Pongpornsup | first2 = S. | last3 = Suthikeeree | first3 = W. | title = Wall thickness and outer diameter of the normal appendix in adults using 64 slices multidetector CT. | journal = J Med Assoc Thai | volume = 93 | issue = 12 | pages = 1437-42 | month = Dec | year = 2010 | doi = | PMID = 21344807 }}</ref>
| |
| **Similar numbers are found in another study.<ref name=pmid17457270>{{Cite journal | last1 = Huwart | first1 = L. | last2 = El Khoury | first2 = M. | last3 = Lesavre | first3 = A. | last4 = Phan | first4 = C. | last5 = Rangheard | first5 = AS. | last6 = Bessoud | first6 = B. | last7 = Menu | first7 = Y. | title = [What is the thickness of the normal appendix on MDCT?]. | journal = J Radiol | volume = 88 | issue = 3 Pt 1 | pages = 385-9 | month = Mar | year = 2007 | doi = | PMID = 17457270 }}</ref>
| |
| | |
| ===Microscopic===
| |
| Features:
| |
| * Neutrophils in the muscularis propria - '''key feature'''.
| |
| * +/- Vascular [[thrombosis]] (and [[necrosis]]) - known as ''gangrenous appendicitis''.<ref>URL: [http://emedicine.medscape.com/article/363818-overview http://emedicine.medscape.com/article/363818-overview]. Accessed on: 21 June 2010.</ref>
| |
| * +/- Findings suggestive of etiology - usu. absent:
| |
| ** +/- Fecalith.
| |
| ** +/- Viral inclusions (extremely rare)
| |
| *** See ''[[adenovirus appendicitis]]''.
| |
| | |
| Note:
| |
| *Eosinophils are very common.<ref name=pmid9444860>{{Cite journal | last1 = Aravindan | first1 = KP. | title = Eosinophils in acute appendicitis: possible significance. | journal = Indian J Pathol Microbiol | volume = 40 | issue = 4 | pages = 491-8 | month = Oct | year = 1997 | doi = | PMID = 9444860 }}</ref>
| |
| **Appendices with eosinophils but no apparent [[neutrophil]]s probably represent the same process.<ref name=pmid20551528>{{Cite journal | last1 = Aravindan | first1 = KP. | last2 = Vijayaraghavan | first2 = D. | last3 = Manipadam | first3 = MT. | title = Acute eosinophilic appendicitis and the significance of eosinophil - Edema lesion. | journal = Indian J Pathol Microbiol | volume = 53 | issue = 2 | pages = 258-61 | month = | year = | doi = 10.4103/0377-4929.64343 | PMID = 20551528 }}</ref>
| |
| | |
| DDx:
| |
| *Mucinous tumour.
| |
| *[[Neuroendocrine tumour]].
| |
| *[[Granulomatous appendicitis]].
| |
| *[[Crohn's disease]] of the appendix.
| |
| **Approximately of 40% colectomies for CD (that include an appendix) have involvement of the appendix.<ref name=pmid11956821>{{Cite journal | last1 = Stangl | first1 = PC. | last2 = Herbst | first2 = F. | last3 = Birner | first3 = P. | last4 = Oberhuber | first4 = G. | title = Crohn's disease of the appendix. | journal = Virchows Arch | volume = 440 | issue = 4 | pages = 397-403 | month = Apr | year = 2002 | doi = 10.1007/s004280100532 | PMID = 11956821 }}</ref>
| |
| | |
| Images:
| |
| *[http://commons.wikimedia.org/wiki/File:Appendicitis_-_low_mag.jpg Appendicitis - low mag. (WC)].
| |
| *[http://commons.wikimedia.org/wiki/File:Appendicitis_-_very_high_mag.jpg Appendicitis - very high mag. (WC)].
| |
| | |
| ===Sign out===
| |
| <pre>
| |
| VERMIFORM APPENDIX, APPENDECTOMY:
| |
| - ACUTE APPENDICITIS.
| |
| - ACUTE PERIAPPENDICITIS.
| |
| </pre>
| |
| | |
| <pre>
| |
| VERMIFORM APPENDIX, APPENDECTOMY:
| |
| - GANGRENOUS APPENDICITIS.
| |
| - ACUTE PERIAPPENDICITIS.
| |
| </pre>
| |
| | |
| ====Micro====
| |
| =====Gangrenous appendicitis=====
| |
| The sections shows appendiceal wall with marked acute transmural inflammation and necrotic appendiceal wall with large collections of neutrophils. Several medium-sized blood vessels are thrombosed. A thick layer of neutrophils cover the serosa aspect.
| |
|
| |
|
| ==Adenovirus appendicitis== | | ==Adenovirus appendicitis== |
| ===General===
| | {{Main|Adenovirus appendicitis}} |
| *Rare type of appendicitis in children.
| |
| *Presents as run-of-the-mill acute appendicitis.
| |
| *Caused by ''[[Adenovirus]]''.
| |
| | |
| ===Microscopic===
| |
| Features:<ref name=pmid17990936>{{cite journal |author=Grynspan D, Rabah R |title=Adenoviral appendicitis presenting clinically as acute appendicitis |journal=Pediatr. Dev. Pathol. |volume=11 |issue=2 |pages=138–41 |year=2008 |pmid=17990936 |doi=10.2350/07-06-0299.1 |url=}}</ref>
| |
| *Lymphoid hyperplasia - key feature.
| |
| *+/-Adenovirus inclusions; "smudge cells".
| |
| | |
| Notes:
| |
| *The classic finding of appendicitis (neutrophils infiltrating into the muscularis propria) may be absent.<ref name=pmid17990936/>
| |
| | |
| Image:
| |
| *[http://wiki.medpedia.com/Image:Ab14.jpg?filetimestamp=20091014175858 Smudge cell (medpedia.com)].
| |
| | |
| ===IHC===
| |
| *Adenovirus +ve = '''diagnostic'''.
| |
|
| |
|
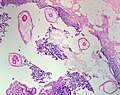
| ==Enterobius vermicularis== | | ==Enterobius vermicularis== |
| Line 156: |
Line 62: |
| *May be found in the appendix. | | *May be found in the appendix. |
| *The incidence is higher in normal appendices than inflamed ones.<ref name=pmid1853157>{{Cite journal | last1 = Wiebe | first1 = BM. | title = Appendicitis and Enterobius vermicularis. | journal = Scand J Gastroenterol | volume = 26 | issue = 3 | pages = 336-8 | month = Mar | year = 1991 | doi = | PMID = 1853157 }}</ref><ref name=pmid7945067/> | | *The incidence is higher in normal appendices than inflamed ones.<ref name=pmid1853157>{{Cite journal | last1 = Wiebe | first1 = BM. | title = Appendicitis and Enterobius vermicularis. | journal = Scand J Gastroenterol | volume = 26 | issue = 3 | pages = 336-8 | month = Mar | year = 1991 | doi = | PMID = 1853157 }}</ref><ref name=pmid7945067/> |
| | *Clinically mimics appendicitis.<ref>{{cite journal |author=Ariyarathenam AV, Nachimuthu S, Tang TY, Courtney ED, Harris SA, Harris AM |title=Enterobius vermicularis infestation of the appendix and management at the time of laparoscopic appendectomy: case series and literature review |journal=Int J Surg |volume=8 |issue=6 |pages=466–9 |year=2010 |pmid=20637320 |doi=10.1016/j.ijsu.2010.06.007 |url=}}</ref> |
|
| |
|
| ===Microscopic=== | | ===Microscopic=== |
| Line 161: |
Line 68: |
| *Usu. the appendiceal wall has no inflammation, i.e. there is no appendicitis.<ref name=pmid1853157/><ref name=pmid7945067>{{Cite journal | last1 = Dahlstrom | first1 = JE. | last2 = Macarthur | first2 = EB. | title = Enterobius vermicularis: a possible cause of symptoms resembling appendicitis. | journal = Aust N Z J Surg | volume = 64 | issue = 10 | pages = 692-4 | month = Oct | year = 1994 | doi = | PMID = 7945067 }}</ref> | | *Usu. the appendiceal wall has no inflammation, i.e. there is no appendicitis.<ref name=pmid1853157/><ref name=pmid7945067>{{Cite journal | last1 = Dahlstrom | first1 = JE. | last2 = Macarthur | first2 = EB. | title = Enterobius vermicularis: a possible cause of symptoms resembling appendicitis. | journal = Aust N Z J Surg | volume = 64 | issue = 10 | pages = 692-4 | month = Oct | year = 1994 | doi = | PMID = 7945067 }}</ref> |
| *''[[Enterobius vermicularis]]'' organisms. | | *''[[Enterobius vermicularis]]'' organisms. |
| | |
| | ====Image==== |
| | <gallery> |
| | Image:Enterobius_-_very_low_mag.jpg | Enterobius - very low mag. (WC/Nephron) |
| | Image:Enterobius_-_high_mag.jpg | Enterobius - high mag. (WC/Nephron) |
| | Image:Pinworms_in_the_Appendix_%281%29.jpg | Pinworm (WC/Uthman) |
| | </gallery> |
|
| |
|
| ==Granulomatous appendicitis== | | ==Granulomatous appendicitis== |
| ===General===
| | {{Main|Granulomatous appendicitis}} |
| Most common cause:
| |
| *Yersinia appendicitis.<ref name=pmid11257626>{{cite journal |author=Lamps LW, Madhusudhan KT, Greenson JK, ''et al.'' |title=The role of Yersinia enterocolitica and Yersinia pseudotuberculosis in granulomatous appendicitis: a histologic and molecular study |journal=Am. J. Surg. Pathol. |volume=25 |issue=4 |pages=508–15 |year=2001 |month=April |pmid=11257626 |doi= |url=}}</ref>
| |
| | |
| DDx:<ref>[http://granuloma.homestead.com/appendicitis.html http://granuloma.homestead.com/appendicitis.html]</ref>
| |
| *Yersinia appendicitis.<ref name=pmid11257626>{{cite journal |author=Lamps LW, Madhusudhan KT, Greenson JK, ''et al.'' |title=The role of Yersinia enterocolitica and Yersinia pseudotuberculosis in granulomatous appendicitis: a histologic and molecular study |journal=Am. J. Surg. Pathol. |volume=25 |issue=4 |pages=508–15 |year=2001 |month=April |pmid=11257626 |doi= |url=}}</ref>
| |
| **Yersinia = gram negative rod (red on [[Gram stain]]).
| |
| **"Safety pin"-like appearance<ref>URL: [http://www.cdc.gov/ncidod/dvbid/plague/p1.htm http://www.cdc.gov/ncidod/dvbid/plague/p1.htm]. Accessed on: 30 June 2011.</ref> - approximately 0.5 micrometers diameter x 2 micrometers length.
| |
| *Other micro-organism ([[TB]], fungus).
| |
| *[[Crohn's disease]].
| |
| *[[Sarcoidosis]].
| |
| *Foreign body reaction.
| |
| *Interval (delayed) appendectomy.
| |
| **Approximately 60% of delayed appendectomies have granulomas.<ref name=pmid12883248>{{Cite journal | last1 = Guo | first1 = G. | last2 = Greenson | first2 = JK. | title = Histopathology of interval (delayed) appendectomy specimens: strong association with granulomatous and xanthogranulomatous appendicitis. | journal = Am J Surg Pathol | volume = 27 | issue = 8 | pages = 1147-51 | month = Aug | year = 2003 | doi = | PMID = 12883248 }}</ref>
| |
| | |
| ===Microscopic===
| |
| Features:
| |
| *[[Granulomas]].
| |
| *+/-"Safety pin"-like organisms (Yersinia).
| |
| | |
| Image(s):
| |
| *[http://www.cdc.gov/ncidod/dvbid/plague/p1.htm Yersinia (CDC)].
| |
|
| |
|
| ==Inflammatory bowel disease== | | ==Inflammatory bowel disease== |
| Line 201: |
Line 94: |
| *Acute inflammation of the serosa. | | *Acute inflammation of the serosa. |
| **[[Neutrophil]]s in the serosa. | | **[[Neutrophil]]s in the serosa. |
| | |
| | DDx: |
| | *[[Acute appendicitis]]. |
|
| |
|
| =Tumours of the appendix= | | =Tumours of the appendix= |
| Line 207: |
Line 103: |
|
| |
|
| ==Mucinous tumours of the appendix== | | ==Mucinous tumours of the appendix== |
| :''Benign appendiceal [[mucocele]]'' and ''appendiceal mucocele'' redirect here.
| | {{Main|Mucinous tumours of the appendix}} |
| ===General===
| | This grouping includes ''mucinous cystadenoma'' and ''mucinous cystadenocarcinoma''. |
| *There are many classifications and they are controversial.<ref name=pmid21970481>{{Cite journal | last1 = Panarelli | first1 = NC. | last2 = Yantiss | first2 = RK. | title = Mucinous neoplasms of the appendix and peritoneum. | journal = Arch Pathol Lab Med | volume = 135 | issue = 10 | pages = 1261-8 | month = Oct | year = 2011 | doi = 10.5858/arpa.2011-0034-RA | PMID = 21970481 }}</ref>
| |
| **The controversy centres on whether to call all mucinous tumours outside of the appendix ''adenocarcinoma'' - regardless of whether they have atypia & show invasion.
| |
| *''Panarelli and Yantiss'' created a nice summary table - that compare the classifications - see: [http://www.archivesofpathology.org/action/showFullPopup?id=i1543-2165-135-10-1261-t01&doi=10.5858%2Farpa.2011-0034-RA comparison of classifications (archivesofpathology.org)].<ref name=pmid21970481/>
| |
| *In women - an ovarian primary must be excluded.
| |
| **Concurrent ''bilateral'' ovarian tumours suggests the tumour originated from the appendix and spread to the ovaries.
| |
| *[[Onlinepathology]] prefers the classification of Misdraji,<ref name=pmid12883241>{{cite journal |author=Misdraji J, Yantiss RK, Graeme-Cook FM, Balis UJ, Young RH |title=Appendiceal mucinous neoplasms: a clinicopathologic analysis of 107 cases |journal=Am. J. Surg. Pathol. |volume=27 |issue=8 |pages=1089–103 |year=2003 |month=August |pmid=12883241 |doi= |url=http://meta.wkhealth.com/pt/pt-core/template-journal/lwwgateway/media/landingpage.htm?issn=0147-5185&volume=27&issue=8&spage=1089}}</ref> as it is the least complicated
| |
| | |
| ====Misdraji classification====
| |
| *Benign - ''low grade mucinous tumour''.
| |
| *Borderline - ''mucinous tumour of uncertain malignant potential'' or ''borderline mucinous tumour''.
| |
| *Malignant - ''mucinous adenocarcinoma''.
| |
| | |
| Five year survival (in a series of 107 cases) as per Misdraji classification:<ref name=pmid12883241/>
| |
| {| class="wikitable sortable"
| |
| !Tumour
| |
| !Five year survival
| |
| |-
| |
| |LAMN
| |
| |100%
| |
| |-
| |
| |LAMN extra-appendiceal spread
| |
| |86%
| |
| |-
| |
| |MACA
| |
| |44%
| |
| |-
| |
| |}
| |
| *LAMN = low-grade appendiceal mucinous neoplasm.
| |
| *LAMN extra-appendiceal = low-grade appendiceal mucinous neoplasm with extra-appendiceal spread.
| |
| *MACA = mucinous adenocarcinoma of the appendix.
| |
| | |
| ====World Health Organization classification====
| |
| WHO classification:
| |
| *Adenoma with low-grade dysplasia.
| |
| *Adenoma with high-grade dysplasia.
| |
| *Low-grade invasive mucinous adenocarcinoma
| |
| **Confined to the appendiceal wall.
| |
| **Outside of the appendix.
| |
| *High-grade invasive mucinous adenocarcinoma.
| |
| | |
| ====Comparison between Misdraji and WHO classification====
| |
| Adapted from ''Panarelli and Yantiss'':<ref name=pmid21970481>{{Cite journal | last1 = Panarelli | first1 = NC. | last2 = Yantiss | first2 = RK. | title = Mucinous neoplasms of the appendix and peritoneum. | journal = Arch Pathol Lab Med | volume = 135 | issue = 10 | pages = 1261-8 | month = Oct | year = 2011 | doi = 10.5858/arpa.2011-0034-RA | PMID = 21970481 }}</ref>
| |
| {| class="wikitable sortable"
| |
| ! Stage
| |
| ! Cytologic dysplasia
| |
| ! Misdraji
| |
| ! World Health Organization
| |
| |-
| |
| | Confined to the mucosa
| |
| | low-grade
| |
| | low-grade appendiceal mucinous neoplasm (LAMN)
| |
| | mucinous adenoma, negative for high-grade dysplasia
| |
| |-
| |
| | Confined to the mucosa
| |
| | high-grade
| |
| | non-invasive mucinous cystadenocarcinoma of the appendix
| |
| | mucinous adenoma with high-grade dysplasia
| |
| |-
| |
| | At least into the submucosa, confined to the appendix
| |
| | low-grade
| |
| | low-grade appendiceal mucinous neoplasm (LAMN)
| |
| | invasive mucinous adenocarcinoma, low-grade
| |
| |-
| |
| | At least into the submucosa, confined to the appendix
| |
| | high-grade
| |
| | mucinous adenocarcinoma of the appendix (MACA)
| |
| | invasive mucinous adenocarcinoma, high-grade
| |
| |-
| |
| | Extra-appendiceal spread
| |
| | low-grade
| |
| | low-grade appendiceal mucinous neoplasm (LAMN)
| |
| | invasive mucinous adenocarcinoma, low-grade
| |
| |-
| |
| | Extra-appendiceal spread
| |
| | high-grade
| |
| | mucinous adenocarcinoma of the appendix (MACA)
| |
| | invasive mucinous adenocarcinoma, high-grade
| |
| |}
| |
| | |
| ===Microscopic===
| |
| ====Low-grade appendiceal mucinous neoplasm====
| |
| *[[AKA]] ''benign mucinous tumour of the appendix''.
| |
| | |
| Microscopic:
| |
| *Single layer of epithelium with ''tufts''.
| |
| **Vaguely resemble ''serrations'', i.e. the ''saw-tooth'' pattern in hyperplastic polyps of the colon.
| |
| *Mucin contained (inside appendix only).
| |
| *No marked nuclear atypia.
| |
| | |
| Note:
| |
| *May be deceptively bland appearing from a cytologic perspective.
| |
| | |
| Images:
| |
| *[http://www.nature.com/modpathol/journal/v17/n12/fig_tab/3800212f1.html LAMN - low mag. (nature.com)].<ref name=pmid15354187/>
| |
| *[http://www.nature.com/modpathol/journal/v17/n12/fig_tab/3800212f3.html LAMN - high mag. (nature.com)].<ref name=pmid15354187>{{Cite journal | last1 = Misdraji | first1 = J. | last2 = Burgart | first2 = LJ. | last3 = Lauwers | first3 = GY. | title = Defective mismatch repair in the pathogenesis of low-grade appendiceal mucinous neoplasms and adenocarcinomas. | journal = Mod Pathol | volume = 17 | issue = 12 | pages = 1447-54 | month = Dec | year = 2004 | doi = 10.1038/modpathol.3800212 | PMID = 15354187 }}</ref>
| |
| *[http://pathlabmed.typepad.com/surgical_pathology_and_la/2012/02/digital-case-simple-mucocele-of-the-appendix.html Appendiceal mucocele (pathlabmed.typepad.com)].
| |
| | |
| ====Low-grade appendiceal mucinous neoplasm with extra-appendiceal spread====
| |
| *[[AKA]] ''mucinous borderline tumour of the appendix''.
| |
| | |
| Microscopic:
| |
| *Same as LAMN but mucin outside of the appendix.
| |
| *Cells in mucin, i.e. cellular mucin.
| |
| | |
| ====Mucinous adenocarcinoma of the appendix====
| |
| *[[AKA]] ''malignant mucinous tumour of the appendix''.
| |
| | |
| Microscopic:
| |
| *Marked nuclear pleomorphism.
| |
| *Invasion into the appendiceal wall.
| |
| | |
| ===Sign out===
| |
| ====LAMN====
| |
| <pre>
| |
| VERMIFORM APPENDIX, APPENDECTOMY:
| |
| - LOW-GRADE APPENDICEAL MUCINOUS NEOPLASM.
| |
| - ACUTE APPENDICITIS.
| |
| - ACUTE PERIAPPENDICITIS.
| |
| </pre>
| |
| | |
| <pre>
| |
| VERMIFORM APPENDIX AND CECUM, APPENDECTOMY WITH CECAL CUFF:
| |
| - LOW-GRADE APPENDICEAL MUCINOUS NEOPLASM (MUCINOUS CYSTADENOMA).
| |
| - MARGINS NEGATIVE FOR MUCINOUS NEOPLASM.
| |
| | |
| COMMENT:
| |
| No extra-appendiceal mucin is identified. There is no invasion into the appendiceal wall.
| |
| </pre>
| |
| | |
| ==Goblet cell carcinoid==
| |
| *[[AKA]] ''crypt cell carcinoma''.<ref name=pmid18042066>{{cite journal |author=van Eeden S, Offerhaus GJ, Hart AA, ''et al.'' |title=Goblet cell carcinoid of the appendix: a specific type of carcinoma |journal=Histopathology |volume=51 |issue=6 |pages=763–73 |year=2007 |month=December |pmid=18042066 |doi=10.1111/j.1365-2559.2007.02883.x |url=}}</ref>
| |
| *[[AKA]] ''[[neuroendocrine tumour]] with goblet cell differentiation''.
| |
| ===General===
| |
| *Rare appendiceal tumour that typically has an aggressive course vis-a-vis other appendiceal carcinoids.<ref name=pmid18042066>{{cite journal |author=van Eeden S, Offerhaus GJ, Hart AA, ''et al.'' |title=Goblet cell carcinoid of the appendix: a specific type of carcinoma |journal=Histopathology |volume=51 |issue=6 |pages=763–73 |year=2007 |month=December |pmid=18042066 |doi=10.1111/j.1365-2559.2007.02883.x |url=}}</ref>
| |
| *Mixed (biphasic) tumour with endocrine and exocrine features.
| |
| | |
| ===Microscopic===
| |
| Features:<ref name=pmid15967038>{{cite journal |author=Pahlavan PS, Kanthan R |title=Goblet cell carcinoid of the appendix |journal=World J Surg Oncol |volume=3 |issue= |pages=36 |year=2005 |month=June |pmid=15967038 |pmc=1182398 |doi=10.1186/1477-7819-3-36 |url=http://wjso.com/content/3/1/36}}</ref>
| |
| *Mixed neuroendocrine-nonneuroendocrine tumour;<ref name=pmid17684764>{{cite journal |author=Volante M, Righi L, Asioli S, Bussolati G, Papotti M |title=Goblet cell carcinoids and other mixed neuroendocrine/nonneuroendocrine neoplasms |journal=Virchows Arch. |volume=451 Suppl 1 |issue= |pages=S61–9 |year=2007 |month=August |pmid=17684764 |doi=10.1007/s00428-007-0447-y |url=}}</ref> features of both ''carcinoid'' and ''adenocarcinoma.<ref name=pmid15967038>PMID 15967038.</ref>
| |
| **Archictecture: cells arranged in nests or clusters without a lumen.
| |
| **Location: deep to the intestinal crypts (crypts of Lieberkühn); usually do not involve the mucosa.
| |
| **Cytoplasm distended with mucin.
| |
| **DNA: crescentic nucleus (similar to in signet-ring cells).
| |
| ***+/-Multinucleation.
| |
| ***+/-High mitotic rate.
| |
| ***Usually minimal nuclear atypia.
| |
| | |
| Images:
| |
| *[http://commons.wikimedia.org/wiki/File:Goblet_cell_carcinoid_-2-_very_high_mag.jpg GCC - very high mag. (WC)].
| |
| *[http://commons.wikimedia.org/wiki/File:Goblet_cell_carcinoid_-_very_low_mag.jpg GCC - very low mag. (WC)].
| |
| | |
| ===Stains===
| |
| *Mucin stains +ve:
| |
| **Mucicarmine, perodic acid-Schiff diastase (PAS-D), alician blue.
| |
| | |
| ====IHC====
| |
| *Classic neuroendocrine markers:
| |
| **Synaptophysin +ve.
| |
| **Chromogranin +ve.
| |
| *S100 +ve.
| |
| *NSE +ve.
| |
| *Serotonin +ve.
| |
| | |
| Keratins:
| |
| *Usually CK20 +ve > CK7 +ve.
| |
| | |
| *CEA +ve (membrane).
| |
|
| |
|
| Notes:
| | ==Goblet cell adenocarcinoma== |
| *Nice review of stains in Pahlavan and Kanthan.<ref name=pmid15967038>{{cite journal |author=Pahlavan PS, Kanthan R |title=Goblet cell carcinoid of the appendix |journal=World J Surg Oncol |volume=3 |issue= |pages=36 |year=2005 |month=June |pmid=15967038 |pmc=1182398 |doi=10.1186/1477-7819-3-36 |url=http://wjso.com/content/3/1/36}}</ref>
| | {{Main|Goblet cell adenocarcinoma}} |
| | *Previously known as ''goblet cell carcinoid''. |
|
| |
|
| ==Neuroendocrine tumour of the appendix== | | ==Neuroendocrine tumour of the appendix== |
| {{Main|Neuroendocrine tumour}}
| |
| *Previously known as ''appendiceal carcinoid''. | | *Previously known as ''appendiceal carcinoid''. |
| *[[AKA]] ''appendiceal neuroendocrine tumour'', abbreviated ''appendiceal NET''. | | *[[AKA]] ''appendiceal neuroendocrine tumour'', abbreviated ''appendiceal NET''. |
| ===General===
| | {{Main|Neuroendocrine tumour of the appendix}} |
| *Most common tumour of the appendix.<ref name=PCPBoD8_435>{{Ref PCPBoD8|435}}</ref>
| |
| | |
| Size matters in ''appendiceal NETs'':<ref name=pmid12569593>{{Cite journal | last1 = Modlin | first1 = IM. | last2 = Lye | first2 = KD. | last3 = Kidd | first3 = M. | title = A 5-decade analysis of 13,715 carcinoid tumors. | journal = Cancer | volume = 97 | issue = 4 | pages = 934-59 | month = Feb | year = 2003 | doi = 10.1002/cncr.11105 | PMID = 12569593 }}</ref>
| |
| *<1.0 cm - do not metastasize.
| |
| *1.0-2.0 cm - rarely metastasize.
| |
| | |
| ===Microscopic===
| |
| Features:
| |
| *See ''[[neuroendocrine tumours]]''.
| |
| | |
| ===IHC===
| |
| Features:
| |
| *Chromogranin A -ve/+ve.
| |
| *Synaptophysin +ve.
| |
| | |
| See: ''[[neuroendocrine tumours]]''.
| |
|
| |
|
| =See also= | | =See also= |
| Line 410: |
Line 123: |
|
| |
|
| [[Category:Gastrointestinal pathology]] | | [[Category:Gastrointestinal pathology]] |
| | [[Category:Vermiform appendix]] |




.jpg)