Difference between revisions of "Vermiform appendix"
| Line 99: | Line 99: | ||
=====Alternate===== | =====Alternate===== | ||
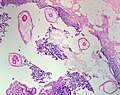
The section show appendiceal wall without increased numbers of neutrophils. The | The section show appendiceal wall without increased numbers of neutrophils. The | ||
appendiceal lumen has | appendiceal lumen has cellular debris and inflammatory cells. The mucosa has prominent lymphoid tissue | ||
with germinal centre formation. | with germinal centre formation. | ||
Revision as of 19:47, 17 November 2015
The vermiform appendix, usually just appendix, is a little thingy that is attached to the cecum. Taking it out is the bread 'n butter of general surgery.
The appendix is a vestigial structure that is thought to have arisen from a larger cecum. Larger cecae are often seen in herbivores and thought to facilitate better digestion of plant matter.[1]
Normal
Normal vermiform appendix
General
- Seen in:
- Right hemicolectomies.
- Surgeries for ovarian mucinous tumours.
Gross
- Shiny serosal surface.
- No exudate.
- Normal diameter.
- 6.6 +/- 1.5 mm -- based on CT.[2]
Microscopic
Features:
- +/-Lymphoid hyperplasia - mucosa or submucosa.
- Normal colorectal-type mucosa.
- Fatty submucosa.
- Benign smooth muscle.
- Serosa.
Negatives:
- No neutrophils in the muscularis propria.
- No lesion in appendiceal tip.
- No serosal inflammation (periappendicitis).
- No organisms in the appendiceal lumen, e.g. Enterobius vermicularis.
DDx:
- Adenovirus appendicitis.
- Cryptosporidiosis.
- Mild colitis.
Sign out
VERMIFORM APPENDIX WITHIN NORMAL LIMITS.
Negative appendectomy
General
- Common.
- Use for quality control among general surgeons.[citation needed]
Gross
See normal vermiform appendix.
Microscopic
See normal vermiform appendix.
Notes:
- Should be submitted in total.
DDx:
- Acute appendicitis.
- Adenovirus appendicitis.
- Appendiceal neuroendocrine tumour.
- Non-appendiceal pathology - see DDx of acute appendicitis.
- Isolated periappendicitis.
- Crypt cell carcinoma - AKA goblet cell carcinoid.
Sign out
Vermiform Appendix, Appendectomy: - Appendix within normal limits. - One benign lymph node. - NEGATIVE for acute appendicitis and NEGATIVE for periappendicitis. Comment: The specimen was submitted in total.
Block letters
VERMIFORM APPENDIX, APPENDECTOMY: - APPENDIX NEGATIVE FOR ACUTE APPENDICITIS AND NEGATIVE FOR ACUTE PERIAPPENDICITIS.
VERMIFORM APPENDIX, APPENDECTOMY: - APPENDIX WITH LYMPHOID HYPERPLASIA AND FOCAL MUCOSAL EROSIONS. - NEGATIVE FOR ACUTE APPENDICITIS. - NEGATIVE FOR ACUTE PERIAPPENDICITIS.
Micro
The sections show appendiceal wall with focal mucosa erosions and several intraluminal neutrophil clusters. Lymphoid hyperplasia is present. Fecal material is present within the lumen of the appendix.
There are no neutrophils within the muscularis propria. There is no serositis. There is no distortion of the crypt architecture. No granulomas are identified. No cryptitis is identified.
Alternate
The section show appendiceal wall without increased numbers of neutrophils. The appendiceal lumen has cellular debris and inflammatory cells. The mucosa has prominent lymphoid tissue with germinal centre formation.
No intraluminal pathologic micro-organisms are seen. There is no serositis. There is no distortion of the crypt architecture. No granulomas are identified. No cryptitis is identified.
Inflammatory pathologies
Acute appendicitis
Adenovirus appendicitis
Enterobius vermicularis
- AKA pinworm.
General
- May be found in the appendix.
- The incidence is higher in normal appendices than inflamed ones.[3][4]
- Clinically mimics appendicitis.[5]
Microscopic
Features:
- Usu. the appendiceal wall has no inflammation, i.e. there is no appendicitis.[3][4]
- Enterobius vermicularis organisms.
Image

Enterobius - very low mag. (WC/Nephron)

Enterobius - high mag. (WC/Nephron)
Pinworm (WC/Uthman)


.jpg)
Granulomatous appendicitis
Inflammatory bowel disease
Periappendicitis
General
Definition: inflammation of tissues around the (vermiform) appendix.[6]
- May be seen in association of appendicitis or alone.
Microscopic
Features:
- Acute inflammation of the serosa.
- Neutrophils in the serosa.
DDx:
Tumours of the appendix
Adenocarcinoma
- Like colorectal adenocarcinoma - see colorectal tumours.
Mucinous tumours of the appendix
This grouping includes mucinous cystadenoma and mucinous cystadenocarcinoma.
Goblet cell carcinoid
Neuroendocrine tumour of the appendix
- Previously known as appendiceal carcinoid.
- AKA appendiceal neuroendocrine tumour, abbreviated appendiceal NET.
See also
References
- ↑ Dawkins, R. (2009). The Greatest Show on Earth: The Evidence for Evolution (1st ed.). Free Press. pp. 115. ISBN 978-1416594789.
- ↑ Charoensak, A.; Pongpornsup, S.; Suthikeeree, W. (Dec 2010). "Wall thickness and outer diameter of the normal appendix in adults using 64 slices multidetector CT.". J Med Assoc Thai 93 (12): 1437-42. PMID 21344807.
- ↑ 3.0 3.1 Wiebe, BM. (Mar 1991). "Appendicitis and Enterobius vermicularis.". Scand J Gastroenterol 26 (3): 336-8. PMID 1853157.
- ↑ 4.0 4.1 Dahlstrom, JE.; Macarthur, EB. (Oct 1994). "Enterobius vermicularis: a possible cause of symptoms resembling appendicitis.". Aust N Z J Surg 64 (10): 692-4. PMID 7945067.
- ↑ Ariyarathenam AV, Nachimuthu S, Tang TY, Courtney ED, Harris SA, Harris AM (2010). "Enterobius vermicularis infestation of the appendix and management at the time of laparoscopic appendectomy: case series and literature review". Int J Surg 8 (6): 466–9. doi:10.1016/j.ijsu.2010.06.007. PMID 20637320.
- ↑ URL: http://www.medilexicon.com/medicaldictionary.php?t=66889. Accessed on: 1 June 2011.
- ↑ Fink, AS.; Kosakowski, CA.; Hiatt, JR.; Cochran, AJ. (Jun 1990). "Periappendicitis is a significant clinical finding.". Am J Surg 159 (6): 564-8. PMID 2349982.
- ↑ O'Neil, MB.; Moore, DB. (Sep 1977). "Periappendicitis: Clinical reality or pathologic curiosity?". Am J Surg 134 (3): 356-7. PMID 900337.