Difference between revisions of "Vasculitides"
(→See also: +umbilical cord) |
(+images) |
||
| Line 190: | Line 190: | ||
**It may difficult to find small blood vessels in affected portions of lung. | **It may difficult to find small blood vessels in affected portions of lung. | ||
Images | ====Images==== | ||
www: | |||
*[http://www.flickr.com/photos/pulmonary_pathology/3734403695/ Wegener's granulomatosis (flickr.com)]. | |||
*[http://path.upmc.edu/cases/case269.html Wegener's granulomatosis - several crappy images (upmc.edu)]. | |||
*[http://path.upmc.edu/cases/case660.html Wegener's granulomatosis - more crappy images (upmc.edu)]. | |||
*[http://path.upmc.edu/cases/case675.html WG - more images (upmc.edu)]. | |||
<gallery> | |||
Image:Wegener%27s_granulomatosis_-b-_intermed_mag.jpg |WG - intermed. mag. (WC) | |||
Image:Wegener%27s_granulomatosis_-b-_very_high_mag.jpg |WG - fibrinoid necrosis - very high mag. (WC) | |||
</gallery> | |||
==Churg-Strauss syndrome== | ==Churg-Strauss syndrome== | ||
*Abbreviated ''CSS''. | *Abbreviated ''CSS''. | ||
| Line 220: | Line 220: | ||
*Abundant eosinophils. | *Abundant eosinophils. | ||
*[[Granuloma]]s. | *[[Granuloma]]s. | ||
DDx: | DDx: | ||
*Eosinophilic vasculitis associated with a [[connective tissue disease]].<ref name=pmid8708015>{{Cite journal | last1 = Chen | first1 = KR. | last2 = Su | first2 = WP. | last3 = Pittelkow | first3 = MR. | last4 = Conn | first4 = DL. | last5 = George | first5 = T. | last6 = Leiferman | first6 = KM. | title = Eosinophilic vasculitis in connective tissue disease. | journal = J Am Acad Dermatol | volume = 35 | issue = 2 Pt 1 | pages = 173-82 | month = Aug | year = 1996 | doi = | PMID = 8708015 }}</ref> | *Eosinophilic vasculitis associated with a [[connective tissue disease]].<ref name=pmid8708015>{{Cite journal | last1 = Chen | first1 = KR. | last2 = Su | first2 = WP. | last3 = Pittelkow | first3 = MR. | last4 = Conn | first4 = DL. | last5 = George | first5 = T. | last6 = Leiferman | first6 = KM. | title = Eosinophilic vasculitis in connective tissue disease. | journal = J Am Acad Dermatol | volume = 35 | issue = 2 Pt 1 | pages = 173-82 | month = Aug | year = 1996 | doi = | PMID = 8708015 }}</ref> | ||
====Images==== | |||
<gallery> | |||
Image:Churg-Strauss_syndrome_-_high_mag.jpg |CSS - high mag. (WC) | |||
Image:Churg-Strauss_syndrome_-_very_high_mag.jpg |CSS - very high mag. (WC) | |||
</gallery> | |||
=Medium vessel vasculitides= | =Medium vessel vasculitides= | ||
The follow section has information specific to the individual types of medium vessel vasculitis. | The follow section has information specific to the individual types of medium vessel vasculitis. | ||
Revision as of 05:36, 10 December 2014
This article deals with the vasculitides (singular vasculitis). Vascular disease that is not vasculitides is covered in the article vascular disease.
The histology of normal vessels is dealt with in normal blood vessels.
Overview
Most common[1]
- Polyarteritis nodosa (PAN).
- Microscopic polyangiitis.
- Wegener's granulomatosis.
- Predominantly cutaneous vasculitis.
- Giant cell arteritis (GCA).
Grouping by size
Small vessel vasculitides
Definition
Small vessel vasculitis = vasculitis of vessels smaller than arteries; affects arterioles, venules, and capillaries.[2]
- What is an arteriole?
- There is no histologic definition according to Sternberg's Histology for Pathologists; however, a diameter of <100 micrometers is suggested as a definition.[3]
Types
- Predominantly cutaneous vasculitis.
- Henoch-Schoenlein purpura.
- Essential cryoglobulinemic vasculitis.
- ANCA-associated:
- Wegener's granulomatosis (c-ANCA > p-ANCA).
- Churg-Strauss syndrome (50% ANCA +ve).
- Microscopic polyangiitis (usually p-ANCA).
Notes:
- ANCA = anti-neutrophil cytoplasmic antibodies.
- The terminology has changed as more knowledge has been gained:
- MPO-ANCA = p-ANCA.
- PR3-ANCA = c-ANCA.
- The terminology has changed as more knowledge has been gained:
Medium vessel vasculitides[4]
- Polyarteritis nodosa (PAN).
- Kawasaki disease.
Large vessel vasculitides[4]
- Giant cell arteritis (AKA temporal arteritis).
- Takayasu's arteritis.
Grouping by hypersensitivity
Cell-mediated hypersensitivity:[5]
- Giant cell arteritis.
- Takayasu arteritis.
- Churg-Strauss disease.
- Wegener’s granulomatosis.
Note:
- All have granulomas.
Immune complex mediated hypersensitivity:[5]
- Polyarteritis nodosa.
- Microscopic polyangiitis.[citation needed]
- Leukocytoclastic vasculitis.[citation needed]
- Henoch-Schonlein purpura.
Pathologist's role in the diagnosis of vasculitis
General
- Pathologists often cannot, based on morphology alone, arrive at the definitive diagnosis.
- The presentation & distribution are more characteristic than the pathology.[6][7]
Microscopic
Features - both #1 and #2 are required:[8]
- Inflammatory cells within the blood vessel wall.
- Vessel injury:
- +/-RBC extravasation - common.
Notes:
- Involvement is usually patchy.
- If there is an inkling of vasculitis... it should prompt deeper cuts.
Features to consider
- Presence of granulomas.
- Type inflammatory cells, i.e. eosinophils, mononuclear cells.
- Size of vessels involved.
- Extent of involvement.
- Acuity (acute vs. subacute vs. chronic vs. acute on chronic).
- Chronic = thick fibrotic appearing vessels with a small lumen.
Vasculitis versus neuropathy
| Domain | Vasculitis | Neuropathy |
|---|---|---|
| Clinical | pain, diffuse/ patchy distribution |
focal/isolated |
| Pathological (inflammatory cells) |
epineurium | endoneurium |
Small vessel vasculitides
The follow section has information specific to the individual types of small vessel vasculitis.
Small vessel leukocytoclastic vasculitis
- AKA leukocytoclastic vasculitis, abbreviated LCV.
General
- Most common cutaneous vasculitis.[10]
Clinical:
- Palpable purpura, usu. lower extremity.
Microscopic
Features:[10]
- Small upper dermis vessels with:
- Neutrophils.
- Fragmentation of neutrophils (leukocytoclasia).
- Vessel damage: fibrin deposition (bright pink acellular stuff).
- Neutrophils.
Has a very broad DDx:[10]
- Infectious:
- Bacterial.
- Viral.
- Fungal.
- Vasculitic disorders:
- ANCA mediated vasculitides:
- Henoch–Schönlein purpura.[11]
- Urticarial vasculitis.
- Other:
- Connective tissue disease, e.g. mixed connective tissue disease, SLE, rheumatoid arthritis.
- Cryoglobulinemia - may be due to multiple myeloma, hepatitis C; have intravascular thrombi.
- Paraneoplastic.
- Drugs.
Image:
Stains
- PAS - look for fungus.
Microscopic polyangiitis
General
- Classically MPO-ANCA (p-ANCA) +ve.
Microscopic
Features - small-sized vessels with:
- Inflammatory cells (neutrophils, lymphocytes) within the tunica media.
- Fibroid necrosis: dead vessel wall - pink anucleate stuff, nuclear debris (black specks of nuclear material).
- No granulomas.
Images:
Wegener granulomatosis
- Abbreviated WG.
- AKA granulomatosis with polyangiitis.
General
- Autoimmune.
Clinical
- Epistasis.
- Renal failure - present as nephritic syndrome.
- Renal biopsy: crescentic glomerulonephritis (AKA rapidly progressive glomerulonephritis).
- Pulmonary hemorrhage.
Serology:
- c-ANCA +ve.[12]
Notes:
- Pulmonary hemorrhage syndromes:[13]
- Goodpasture syndrome.
- Idiopathic pulmonary hemosiderosis.
- Vasculitis-assoc. hemorrhage (hypersensitivity angiitis, Wegener granulomatosis).
- Systemic lupus erythematosus.
Microscopic
Features:
- Small vessel vasculitis:
- Inflammatory cells within the vessel wall.
- Granulomas - typically poorly formed.[14]
- Multinucleated giant cells - common. (???)
- Granulomas - typically poorly formed.[14]
- Vessel wall injury.
- Inflammatory cells within the vessel wall.
Notes:
- In the lung, the granulomas tend to be centrilobular, as the artery travels with the airway and is centrilobular.
- It may difficult to find small blood vessels in affected portions of lung.
Images
www:
- Wegener's granulomatosis (flickr.com).
- Wegener's granulomatosis - several crappy images (upmc.edu).
- Wegener's granulomatosis - more crappy images (upmc.edu).
- WG - more images (upmc.edu).
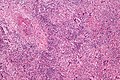
WG - intermed. mag. (WC)
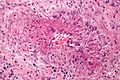
WG - fibrinoid necrosis - very high mag. (WC)


Churg-Strauss syndrome
General
Defining features - memory device GAFE:
- Granulomata.
- Asthma.
- Fever.
- Eosinophilia.
Notes:
- Similar to Wegener's granulomatosis (classically c-ANCA +ve) and microscopic polyangiitis.[16]
Microscopic
Features:
- Small vessel vasculitis.
- Abundant eosinophils.
- Granulomas.
DDx:
- Eosinophilic vasculitis associated with a connective tissue disease.[17]
Images
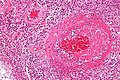
CSS - high mag. (WC)
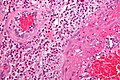
CSS - very high mag. (WC)


Medium vessel vasculitides
The follow section has information specific to the individual types of medium vessel vasculitis.
Kawasaki disease
General
- Medium vessel disease.
- Classically afflicts the coronary arteries of children - usu. less than 5 years old.
- May lead to coronary artery aneurysms.[18]
Clinical features - mnemonic Warm CREAM:[19]
- Warm = fever.
- Conjunctivitis, non-exudative.
- Rash, polymorphous.
- Erythema or edema of hands and feet.
- Adenopathy, usu. cervical and unilateral.
- Mucosal manifestations - strawberry tongue, cracked lips.
Treatment:
- High dose IV aspirin.
Microscopic
Features:
- Medium-sized vessels with intramural inflammatory cells.
- Vessel destruction, e.g. fibrinoid necrosis (very pink anucleate arterial wall).
Polyarteritis nodosa
- Abbreviated PAN.
General
- Involves small and medium sized vessels.
- Often - renal vessels, mesenteric vessels.[20]
- Strong association with hepatitis B (see medical liver diseases); ~1/3 of patients with PAN have HBV.
Serology:
- ANCA is usually negative.
Microscopic
Features - medium-sized vessels with:
- Inflammatory cells (neutrophils, lymphocytes) within the tunica media.
- Fibroid necrosis: dead vessel wall - pink anucleate stuff, nuclear debris (black specks of nuclear material).
- Usu. focal (wall) involvement; classically leads to berry microaneurysms - ergo the name polyarteritis nodosa.
Image:
Large vessel vasculitides
The follow section has information specific to the individual types of large vessel vasculitis.
Giant cell arteritis
- Temporal artery redirects here.
- Abbreviated GCA.
- AKA temporal arteritis.
General
- Classically afflicts the temporal artery.
Clinical features:
- Classic finding: jaw claudication, in a patient older than 50 years.
- Other findings: headache, vision loss or diplopia, scalp tenderness, polymyalgia, weight loss, chills, fever.
Work-up:
- CRP, ESR, temporal artery biopsy.
- ESR normal (>50 years old): <20 mm/hr males, <30 mm/hr females.[22]
Treatment:
- Treat right away with high dose steroids.
- Biopsy is confirmatory.
Microscopic
Features:
- Artery with intramural inflammatory cells.
- Classically granulomatous inflammation.
- Granulomas not required for the diagnosis!
- Classically granulomatous inflammation.
- Destruction of arterial wall, e.g. fibrinoid necrosis (pink anucleate arterial wall).
Image(s):
{kind=link}
Sign out
Negative
TEMPORAL ARTERY, LEFT, BIOPSY: - MEDIUM SIZE ARTERY WITHOUT PATHOLOGIC DIAGNOSIS, SEE COMMENT. COMMENT: A negative biopsy does not rule out the possibility of giant cell (temporal) arteritis, as this may be a focal disorder. The clinical management is dependent upon the clinical impression.
Takayasu arteritis
General
Features:[23]
- Disease of medium/large arteries.
- Classically involves the aortic arch - leading to decreased pulses in the upper limbs.
- Typically in patients <40 yrs old.
- Usually Asian.
Pathogenesis:
- Cell-mediated hypersensitivity.[24][25][citation needed]
Gross
Features:[23]
- Classically involves the aortic arch.
Microscopic
Features:[23]
- Adventitial mononuclear infiltrate with perivascular cuffing of the vasa vasorum.
- Mononuclear inflammation in media.
- Granulomas, giant cells.
- +/-Patchy necrosis of media.
Other
Aortitis
General
- Uncommon.
Gross
Features:
- Tree bark-like appearance.
Notes:
- Several blocks should be submitted.
Image:
{kind=link}
Microscopic
Features:
- Inflammatory cells.
Subclassification:
- Granulomatous.
- Lymphoplasmacytic pattern.
- Mixed inflammatory.
- Suppurative.
LAMP-2 vasculitis
- Associated with pauci-immune necrotizing and crescentic glomerulonephritis.[27]
- Grouped with the ANCA-associated vasculitides.[28]
See also
- Cardiovascular pathology.
- Vascular disease - covers atherosclerosis, medial cystic degeneration.
- Inflammatory skin disorders.
- Umbilical cord vasculitis.
References
- ↑ Yeung, J.C.; Leonard, Blair J. N. (2005). The Toronto Notes 2005 - Review for the MCCQE and Comprehensive Medical Reference (2005 ed.). The Toronto Notes Inc. for Medical Students Inc.. pp. RH3. ISBN 978-0968592854.
- ↑ Jennette JC, Falk RJ (November 1997). "Small-vessel vasculitis". N. Engl. J. Med. 337 (21): 1512–23. doi:10.1056/NEJM199711203372106. PMID 9366584. http://www.nejm.org/doi/full/10.1056/NEJM199711203372106.
- ↑ Sternberg, Stephen S. (1997). Histology for Pathologists (2nd ed.). Lippincott Williams & Wilkins. pp. 769. ISBN 978-0397517183.
- ↑ 4.0 4.1 Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 512. ISBN 978-1416031215.
- ↑ 5.0 5.1 URL: http://dermind.tripod.com/vasculitis.htm. Accessed on: 30 April 2012.
- ↑ URL: http://www.pathology.ubc.ca/path425/PrincipleofPathophysiology/CirculatoryDisorders/SystemicVasculitisDrBWalker.doc. Accessed on: 26 November 2010.
- ↑ URL: http://www.icapture.ubc.ca/who/who_bios_david_walker.shtml. Accessed on: 26 November 2010.
- ↑ Dillon, MJ.; Eleftheriou, D.; Brogan, PA. (Sep 2010). "Medium-size-vessel vasculitis.". Pediatr Nephrol 25 (9): 1641-52. doi:10.1007/s00467-009-1336-1. PMC 2908435. PMID 19946711. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2908435/.
- ↑ URL: http://dictionary.weather.net/dictionary/amorphous. Accessed on: 26 November 2010.
- ↑ 10.0 10.1 10.2 Brinster, NK. (Nov 2008). "Dermatopathology for the surgical pathologist: a pattern-based approach to the diagnosis of inflammatory skin disorders (part II).". Adv Anat Pathol 15 (6): 350-69. doi:10.1097/PAP.0b013e31818b1ac6. PMID 18948765.
- ↑ Kraft, DM.; Mckee, D.; Scott, C. (Aug 1998). "Henoch-Schönlein purpura: a review.". Am Fam Physician 58 (2): 405-8, 411. PMID 9713395.
- ↑ Yeung, J.C.; Leonard, Blair J. N. (2005). The Toronto Notes 2005 - Review for the MCCQE and Comprehensive Medical Reference (2005 ed.). The Toronto Notes Inc. for Medical Students Inc.. pp. RH6. ISBN 978-0968592854.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 745. ISBN 0-7216-0187-1.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 747. ISBN 0-7216-0187-1.
- ↑ http://emedicine.medscape.com/article/333492-overview
- ↑ URL: http://emedicine.medscape.com/article/334024-overview. Accessed on: 22 January 2011.
- ↑ Chen, KR.; Su, WP.; Pittelkow, MR.; Conn, DL.; George, T.; Leiferman, KM. (Aug 1996). "Eosinophilic vasculitis in connective tissue disease.". J Am Acad Dermatol 35 (2 Pt 1): 173-82. PMID 8708015.
- ↑ Taubert, KA.; Shulman, ST. (Jun 1999). "Kawasaki disease.". Am Fam Physician 59 (11): 3093-102, 3107-8. PMID 10392592.
- ↑ URL: http://www.medicalmnemonics.com/cgi-bin/return_browse.cfm?&system=Other%2FMiscellaneous&discipline=Pathology&browse=1. Accessed on: 14 January 2012.
- ↑ Klatt, Edward C. (2006). Robbins and Cotran Atlas of Pathology (1st ed.). Saunders. pp. 14. ISBN 978-1416002741.
- ↑ Matsumoto, T.; Homma, S.; Okada, M.; Kuwabara, N.; Kira, S.; Hoshi, T.; Uekusa, T.; Saiki, S. (Jul 1993). "The lung in polyarteritis nodosa: a pathologic study of 10 cases.". Hum Pathol 24 (7): 717-24. PMID 8100552.
- ↑ URL: http://www.nlm.nih.gov/medlineplus/ency/article/003638.htm. Accessed on: 17 August 2012.
- ↑ 23.0 23.1 23.2 Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 538. ISBN 0-7216-0187-1.
- ↑ Arnaud, L.; Haroche, J.; Mathian, A.; Gorochov, G.; Amoura, Z. (Nov 2011). "Pathogenesis of Takayasu's arteritis: a 2011 update.". Autoimmun Rev 11 (1): 61-7. doi:10.1016/j.autrev.2011.08.001. PMID 21855656.
- ↑ URL: http://dermind.tripod.com/vasculitis.htm. Accessed on: 30 April 2012.
- ↑ Vaideeswar, P.. "Syphilitic aortitis: rearing of the ugly head.". Indian J Pathol Microbiol 53 (4): 624-7. doi:10.4103/0377-4929.72002. PMID 21045381.
- ↑ Bosch X, Mirapeix E (May 2009). "Vasculitis syndromes: LAMP-2 illuminates pathogenesis of ANCA glomerulonephritis". Nat Rev Nephrol 5 (5): 247–9. doi:10.1038/nrneph.2009.51. PMID 19384321. http://www.nature.com/ki/journal/v76/n1/abs/ki2009123a.html.
- ↑ Chen M, Kallenberg CG (2009). "New advances in the pathogenesis of ANCA-associated vasculitides". Clin. Exp. Rheumatol. 27 (1 Suppl 52): S108–14. PMID 19646356.