Difference between revisions of "Pituitary gland"
Jensflorian (talk | contribs) (Variants) |
Jensflorian (talk | contribs) (→Pituitary carcinoma: Update) |
||
| (37 intermediate revisions by the same user not shown) | |||
| Line 2: | Line 2: | ||
Divisions:<ref>[http://www.vivo.colostate.edu/hbooks/pathphys/endocrine/hypopit/histo.html http://www.vivo.colostate.edu/hbooks/pathphys/endocrine/hypopit/histo.html]</ref> | Divisions:<ref>[http://www.vivo.colostate.edu/hbooks/pathphys/endocrine/hypopit/histo.html http://www.vivo.colostate.edu/hbooks/pathphys/endocrine/hypopit/histo.html]</ref> | ||
*Anterior pituitary ([[AKA]] adenohypophysis). | *Anterior pituitary ([[AKA]] adenohypophysis, pars distalis). | ||
*Posterior pituitary (AKA neurohypophysis, neural pituitary). | *Posterior pituitary (AKA neurohypophysis, neural pituitary, pars nervosa). | ||
=Function= | =Function= | ||
| Line 16: | Line 16: | ||
Mnemonic: "Go Look For The Adenoma Please" = GH, LH, FSH, TSH, ACTH, PRL. | Mnemonic: "Go Look For The Adenoma Please" = GH, LH, FSH, TSH, ACTH, PRL. | ||
===Intermedia=== | |||
* Originates from the posterior wall of the Rathke’s pouch. | |||
* Hormones: MSH, ACTH precursor. | |||
* Contains colloid cysts. | |||
===Posterior=== | ===Posterior=== | ||
| Line 57: | Line 62: | ||
*Less cellular. | *Less cellular. | ||
**Usually more cellular in perivascular location. | **Usually more cellular in perivascular location. | ||
Image: [http://www.ouhsc.edu/histology/Glass%20slides/38_09.jpg Herring bodies (ouhsc.edu)]. | |||
<gallery> | |||
File:Pituitary gland histology 2014.jpg | Pituitary gland, low magnification (WC/Athikhun.suw) | |||
</gallery> | |||
=DDx for sella turcica lesions= | =DDx for sella turcica lesions= | ||
*[[Pituitary adenoma]]. | *[[Pituitary adenoma|PitNET]]. | ||
*[[Rathke cleft cyst]]. | *[[Rathke cleft cyst]]. | ||
*[[Craniopharyngioma]]. | *[[Craniopharyngioma]]. | ||
| Line 80: | Line 88: | ||
=Specific entities= | =Specific entities= | ||
==Pituitary adenoma== | ==Pituitary neuroendocrine tumor (PitNET)== | ||
Old terminology '''Pituitary adenoma''' is depreceated. | |||
The WHO 2022 Classification of tumours of endocrine organs recoginizes following tumours:<ref>{{cite journal |vauthors=Asa SL, Mete O, Perry A, Osamura RY |title=Overview of the 2022 WHO Classification of Pituitary Tumors |journal=Endocr Pathol |volume=33 |issue=1 |pages=6–26 |date=March 2022 |pmid=35291028 |doi=10.1007/s12022-022-09703-7 |url=}}</ref> | |||
{| class="wikitable sortable" style="margin-left:auto;margin-right:auto" | |||
! PitNET lineage | |||
! PitNET type | |||
! subtypes | |||
! Hormone IHC | |||
! Transcription factor IHC | |||
|- | |||
| PIT1 | |||
| Somatotroph tumor | |||
| Densely and sparsely granulated tumor | |||
| GH, a-subunit+/-, CK+ | |||
| PIT1 | |||
|- | |||
| PIT1 | |||
| Lactotroph tumor | |||
| Densely and sparsely granulated tumor | |||
| PRL, CK-ve or weak | |||
| PIT1, [[Estrogen receptor|ER]] | |||
|- | |||
| PIT1 | |||
| Mammosomatotroph tumor | |||
| | |||
| GH, PRL (usu. less), CK perinuclear +ve | |||
| PIT1, [[Estrogen receptor|ER]] | |||
|- | |||
| PIT1 | |||
| Thyrotroph tumor | |||
| | |||
| TSH, CK-ve or weak | |||
| PIT1, GATA3 | |||
|- | |||
| PIT1 | |||
| Mature plurihormonal PIT1 lineage tumor | |||
| | |||
| GH, PRL, TSH, a-subunit +/-ve, CK perinuclear | |||
| PIT1, [[Estrogen receptor|ER]], GATA3 | |||
|- | |||
| PIT1 | |||
| Immature PIT1 lineage tumor | |||
| | |||
| Only focal GH, PRL, TSH, a-subunit +/-ve, CK variable | |||
| PIT1, [[Estrogen receptor|ER]] +/-ve, GATA3 +/-ve | |||
|- | |||
| PIT1 | |||
| Acidophilic stem cell tumor | |||
| | |||
| PRL, GH (focal/variable), CK fibrous bodies | |||
| PIT1, [[Estrogen receptor|ER]] | |||
|- | |||
| PIT1 | |||
| Mixed somatotroph and lactotroph tumor | |||
| | |||
| PRL, GH (in separate cells) | |||
| PIT1, [[Estrogen receptor|ER]] (only in lactotroph component) | |||
|- | |||
| TPIT | |||
| Corticotroph tumor | |||
| Densely and sparsely granulated tumors, Crooke cell adenoma | |||
| ACTH,CK+ve | |||
| TPIT | |||
|- | |||
| SF1 | |||
| Gonadotroph tumor | |||
| | |||
| FSH, LH, a-Subunit or none | |||
| SF1, ER, GATA3, CK+/-ve | |||
|- | |||
| None | |||
| Plurihormonal tumor | |||
| | |||
| All combinations possible | |||
| All combinations possible, CK+/-ve | |||
|- | |||
| None | |||
| Null cell adenoma | |||
| | |||
| None (adenohypophyseal?) | |||
| None | |||
|} | |||
Other tumours may be classified as plurhormonal or double adenomas or as adenomas with unusual IHC combination. | |||
===General=== | ===General=== | ||
*Clinical:<ref>{{Ref PBoD8|1100}}</ref> | *Clinical:<ref>{{Ref PBoD8|1100}}</ref> | ||
**Classically: visual field defects (bitemporal hemianopsia). | **Classically: visual field defects (bitemporal hemianopsia). | ||
**Others (increased intracranial pressure): headache, nausea, vomiting. | **Others (increased intracranial pressure): headache, nausea, vomiting. | ||
**Tumor of adults. | |||
Morphologic Classification: | |||
#Microtumor <= 1 cm. | |||
#Macrotumor 1-4 cm. | |||
#Giant tumor > 4cm. | |||
May be classified by what they secrete. | |||
# | #Functional (endocrine hyperfunction). | ||
# | #*Acromegaly/giantism. | ||
#*Hyperprolactinemia. | |||
#*Cushing disease. | |||
#*Hyperthyroidism. | |||
#*Significant elevation of FSH/LH. | |||
#Clinically nonfunctioning. | |||
Notes: | Notes: | ||
''Cushing disease'' is due to pituitary gland hypersecretion of ACTH (due to a pituitary adenoma ''or'' CRH hypersecretion from the hypothalamus).<ref name=Ref_PBoD8_1148>{{Ref PBoD8|1148}}</ref> [[Cushing syndrome]] is hypercortisolism ''not'' due to pituitary gland pathology. | |||
Imaging: | |||
*Sellar enlargement. | |||
*Bone erosion, invasive growth esp. cavernous sinus (35-45%). | |||
*Inhomogenous signal in T1w MRI. | |||
====Familial pituitary adenomas==== | ====Familial pituitary adenomas==== | ||
| Line 121: | Line 231: | ||
*Loss of fibrous stroma. | *Loss of fibrous stroma. | ||
**The cells of a normal (anterior) pituitary are nested. | **The cells of a normal (anterior) pituitary are nested. | ||
*Basophilic cells (corticotrophs). | |||
*Eosinophilic cells(somatotrophs). | |||
*Extensive fibrosis often seen in TSH-producing tumors. | |||
Notes: | Notes: | ||
| Line 146: | Line 259: | ||
Crooke_HE_40x.jpg | Crooke cell adenoma, HE (WC/Marvin101) | Crooke_HE_40x.jpg | Crooke cell adenoma, HE (WC/Marvin101) | ||
File:Crooke Cytokeratins.jpg | Crooke cell adenoma, panCK (WC/Marvin101) | File:Crooke Cytokeratins.jpg | Crooke cell adenoma, panCK (WC/Marvin101) | ||
HE_fibrosis_pituitary_adenoma.jpg | Fibrosis in pituitary adenoma. | |||
</gallery> | </gallery> | ||
| Line 154: | Line 268: | ||
*LH. | *LH. | ||
*FSH. | *FSH. | ||
*TSH | *TSH - [[Hyperthyroidism]] | ||
*GH. | *GH - [[Acromegaly]]. | ||
*Prolactin. | *Prolactin -Galactorrhea, Amenorrhea, Gynecomastia. Golgi staining pattern in sparsely granulated cases. | ||
*ACTH - Cushing | *ACTH - [[Cushing syndrome]]. | ||
*PIT-1: stains somatotrophs, lactotrophs and thyrothrops. | |||
*TPIT: stains corticotrophs. | |||
*SF1: stains gonadotrophs. | |||
*Chromogranin A +ve | |||
*Synaptophysin strongly +ve (except lactotrophs) | |||
*CAM5.2: fibrous bodies in sparsely granulated somatotroph adenoma, Ring-like staining in Crooke cell adenoma. | |||
*MIB-1: Usu less than 3%. | |||
Note: | |||
Null-cell adenoma must be hormone immunonegative and negative for transcription factors. | |||
===Variants=== | ===Variants=== | ||
*Corticotroph adenomas exhibiting Crooke's hyaline change: agressive course.<ref>{{Cite journal | last1 = George | first1 = DH. | last2 = Scheithauer | first2 = BW. | last3 = Kovacs | first3 = K. | last4 = Horvath | first4 = E. | last5 = Young | first5 = WF. | last6 = Lloyd | first6 = RV. | last7 = Meyer | first7 = FB. | title = Crooke's cell adenoma of the pituitary: an aggressive variant of corticotroph adenoma. | journal = Am J Surg Pathol | volume = 27 | issue = 10 | pages = 1330-6 | month = Oct | year = 2003 | doi = | PMID = 14508394 }}</ref> | *Corticotroph adenomas exhibiting Crooke's hyaline change: agressive course.<ref>{{Cite journal | last1 = George | first1 = DH. | last2 = Scheithauer | first2 = BW. | last3 = Kovacs | first3 = K. | last4 = Horvath | first4 = E. | last5 = Young | first5 = WF. | last6 = Lloyd | first6 = RV. | last7 = Meyer | first7 = FB. | title = Crooke's cell adenoma of the pituitary: an aggressive variant of corticotroph adenoma. | journal = Am J Surg Pathol | volume = 27 | issue = 10 | pages = 1330-6 | month = Oct | year = 2003 | doi = | PMID = 14508394 }}</ref> | ||
*Acidophilic stem cell adenomas: large, locally invasive adenoma with low GH activity. <ref>{{Cite journal | last1 = Horvath | first1 = E. | last2 = Kovacs | first2 = K. | last3 = Singer | first3 = W. | last4 = Smyth | first4 = HS. | last5 = Killinger | first5 = DW. | last6 = Erzin | first6 = C. | last7 = Weiss | first7 = MH. | title = Acidophil stem cell adenoma of the human pituitary: clinicopathologic analysis of 15 cases. | journal = Cancer | volume = 47 | issue = 4 | pages = 761-71 | month = Feb | year = 1981 | doi = | PMID = 6261917 }}</ref> | |||
*Sparsely granulated somatotroph adenomas are more invasive than other variants and respond less to medical treatment. <ref>{{Cite journal | last1 = Kato | first1 = M. | last2 = Inoshita | first2 = N. | last3 = Sugiyama | first3 = T. | last4 = Tani | first4 = Y. | last5 = Shichiri | first5 = M. | last6 = Sano | first6 = T. | last7 = Yamada | first7 = S. | last8 = Hirata | first8 = Y. | title = Differential expression of genes related to drug responsiveness between sparsely and densely granulated somatotroph adenomas. | journal = Endocr J | volume = 59 | issue = 3 | pages = 221-8 | month = | year = 2012 | doi = | PMID = 22200580 }}</ref> | |||
* Lactotroph adenomas in men may show aggressive clinical behavior. <ref>{{Cite journal | last1 = Delgrange | first1 = E. | last2 = Vasiljevic | first2 = A. | last3 = Wierinckx | first3 = A. | last4 = François | first4 = P. | last5 = Jouanneau | first5 = E. | last6 = Raverot | first6 = G. | last7 = Trouillas | first7 = J. | title = Expression of estrogen receptor alpha is associated with prolactin pituitary tumor prognosis and supports the sex-related difference in tumor growth. | journal = Eur J Endocrinol | volume = 172 | issue = 6 | pages = 791-801 | month = Jun | year = 2015 | doi = 10.1530/EJE-14-0990 | PMID = 25792376 }}</ref> | |||
*Immature PIT-1 lineage tumors may show aggresive growth. <ref> {{Cite journal | last1 = Mete | first1 = O. | last2 = Gomez-Hernandez | first2 = K. | last3 = Kucharczyk | first3 = W. | last4 = Ridout | first4 = R. | last5 = Zadeh | first5 = G. | last6 = Gentili | first6 = F. | last7 = Ezzat | first7 = S. | last8 = Asa | first8 = SL. | title = Silent subtype 3 pituitary adenomas are not always silent and represent poorly differentiated monomorphous plurihormonal Pit-1 lineage adenomas. | journal = Mod Pathol | volume = 29 | issue = 2 | pages = 131-42 | month = Feb | year = 2016 | doi = 10.1038/modpathol.2015.151 | PMID = 26743473 }}</ref> | |||
===Molecular=== | |||
*GNAS mutations frequently in densely granulated somatotroph tumors. | |||
==Pituitary blastoma== | |||
* New entity introduced in 2017<ref>{{Cite journal | last1 = Lopes | first1 = MBS. | title = The 2017 World Health Organization classification of tumors of the pituitary gland: a summary. | journal = Acta Neuropathol | volume = 134 | issue = 4 | pages = 521-535 | month = Oct | year = 2017 | doi = 10.1007/s00401-017-1769-8 | PMID = 28821944 }}</ref> | |||
* Epithelial glands with rosette-like formations resembling immature Rathke epithelium. | |||
* Synaptophysin +ve, usu. ACTH+ve | |||
* DICER1 mutations<ref>{{Cite journal | last1 = de Kock | first1 = L. | last2 = Sabbaghian | first2 = N. | last3 = Plourde | first3 = F. | last4 = Srivastava | first4 = A. | last5 = Weber | first5 = E. | last6 = Bouron-Dal Soglio | first6 = D. | last7 = Hamel | first7 = N. | last8 = Choi | first8 = JH. | last9 = Park | first9 = SH. | title = Pituitary blastoma: a pathognomonic feature of germ-line DICER1 mutations. | journal = Acta Neuropathol | volume = 128 | issue = 1 | pages = 111-22 | month = Jul | year = 2014 | doi = 10.1007/s00401-014-1285-z | PMID = 24839956 }}</ref> | |||
==Pituitary carcinoma== | |||
* Depreceated in the WHO2022 classification. | |||
* It is acknowledged that PitNETs can be invasive or spread to other sites. | |||
==Rathke cleft cyst== | ==Rathke cleft cyst== | ||
| Line 195: | Line 336: | ||
{{Main|Craniopharyngioma}} | {{Main|Craniopharyngioma}} | ||
== | ==Gangliocytoma== | ||
* Neuronal cells in abundant neuropil. | |||
* S-100, Synaptophysin +ve. | |||
* Isolated sellar cases are very rare. | |||
Image: [[https://twitter.com/sty_md/status/664676241111252992]] | |||
==Mixed Gangliocytoma-adenoma== | |||
AKA: ganglioneuroma, pituitary adenoma with neuronal choristoma (PANCH) | |||
*Neuronal cells mixed with pituitary adenoma cells. | |||
* Approx. 0.25% of all pituitary adenomas. | |||
* Association with somatotroph adenomas (acromegaly). | |||
==Pituicytoma== | |||
{{Main|Pituicytoma}} | {{Main|Pituicytoma}} | ||
| Line 225: | Line 379: | ||
*Rare. | *Rare. | ||
*Autoantigens are unknown. | *Autoantigens are unknown. | ||
*May occur in pregnancy. | |||
*May be misdiagnosed as a nonsecreting adenoma. | *May be misdiagnosed as a nonsecreting adenoma. | ||
| Line 230: | Line 385: | ||
Features:<ref name=pmid18388197>{{cite journal |author=Tzou SC, Lupi I, Landek M, ''et al.'' |title=Autoimmune hypophysitis of SJL mice: clinical insights from a new animal model |journal=Endocrinology |volume=149 |issue=7 |pages=3461–9 |year=2008 |month=July |pmid=18388197 |pmc=2453094 |doi=10.1210/en.2007-1692 |url=}}</ref> | Features:<ref name=pmid18388197>{{cite journal |author=Tzou SC, Lupi I, Landek M, ''et al.'' |title=Autoimmune hypophysitis of SJL mice: clinical insights from a new animal model |journal=Endocrinology |volume=149 |issue=7 |pages=3461–9 |year=2008 |month=July |pmid=18388197 |pmc=2453094 |doi=10.1210/en.2007-1692 |url=}}</ref> | ||
*Lymphocytic infiltration. | *Lymphocytic infiltration. | ||
<gallery> | |||
File:Lymphocytic_hypophysitis_CD3.jpg | Lymphocytic hypophysitis, CD3 IHC. (WC/jensflorian) | |||
</gallery> | |||
=See also= | =See also= | ||
Latest revision as of 11:30, 30 September 2022
The pituitary gland is known as the master gland.
Divisions:[1]
- Anterior pituitary (AKA adenohypophysis, pars distalis).
- Posterior pituitary (AKA neurohypophysis, neural pituitary, pars nervosa).
Function
Anterior
Hormones:[2]
- Growth hormone (GH).
- Luteinizing hormone (LH)
- Follicle-stimulating hormone (FSH)
- Thyroid stimulating hormone (TSH)
- Adrenocorticotropic hormone (ACTH)
- Prolactin (PRL)
Mnemonic: "Go Look For The Adenoma Please" = GH, LH, FSH, TSH, ACTH, PRL.
Intermedia
- Originates from the posterior wall of the Rathke’s pouch.
- Hormones: MSH, ACTH precursor.
- Contains colloid cysts.
Posterior
Hormones:[2]
- Oxytocin.
- Antidiuretic hormone (ADH).
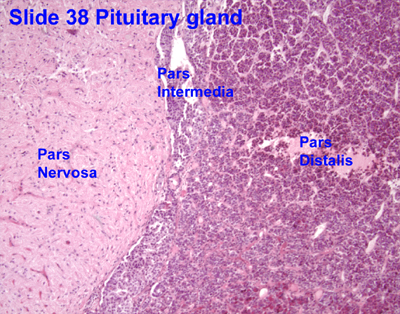
Anatomy and histology
Anatomy
Basic anatomy (simplified):[3]
- Anterior:
- Pars distalis.
- Pars intermedia.
- Posterior:
- Pars nervosa.
Embryological origin:[3]
- Anterior - Rathke's pouch (roof of mouth).
- Posterior - diencephalon (ventral aspect).
Images:
Histology
Anterior
- Acidophils (40% of cells) = red or orange.
- GH, PRL.
- Basophils (10% of cells) = basophilic (light blue).
- TSH, LH, FSH, ACTH.
- Chromophobes (50% of cells) = amphophilic (purplish/grey).
Notes:
- The cellular product (i.e. hormone produced) is not strictly correlated with the cell type.[4]
- The cells can be typed using IHC; somatotrophs (GH), lactotrophs (PRL), corticotrophs (ACTH), thyrotrophs (TSH), gonadotrophs (FSH, LH).[5]
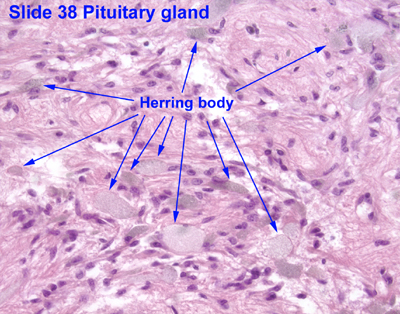
Posterior
Features:[4]
- Herring bodies - key feature.
- Eosinophilic axonal dilations filled with lysosomes and neurosecretory granules.
- Less cellular.
- Usually more cellular in perivascular location.
Image: Herring bodies (ouhsc.edu).

Pituitary gland, low magnification (WC/Athikhun.suw)

DDx for sella turcica lesions
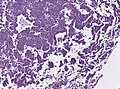
Pituitary necrosis
- Rare.
Causes of pituitary necrosis
- Sheehan syndrome - secondary to blood loss in childbirth.[6]
- Syphilis (fetal-maternal transmission).[7]
- Mollaret's meningitis - very rare.[8] (???)
- Spontaneous necrosis of pituitary tumours - case reports.[9]
Images:
Specific entities
Pituitary neuroendocrine tumor (PitNET)
Old terminology Pituitary adenoma is depreceated. The WHO 2022 Classification of tumours of endocrine organs recoginizes following tumours:[10]
| PitNET lineage | PitNET type | subtypes | Hormone IHC | Transcription factor IHC |
|---|---|---|---|---|
| PIT1 | Somatotroph tumor | Densely and sparsely granulated tumor | GH, a-subunit+/-, CK+ | PIT1 |
| PIT1 | Lactotroph tumor | Densely and sparsely granulated tumor | PRL, CK-ve or weak | PIT1, ER |
| PIT1 | Mammosomatotroph tumor | GH, PRL (usu. less), CK perinuclear +ve | PIT1, ER | |
| PIT1 | Thyrotroph tumor | TSH, CK-ve or weak | PIT1, GATA3 | |
| PIT1 | Mature plurihormonal PIT1 lineage tumor | GH, PRL, TSH, a-subunit +/-ve, CK perinuclear | PIT1, ER, GATA3 | |
| PIT1 | Immature PIT1 lineage tumor | Only focal GH, PRL, TSH, a-subunit +/-ve, CK variable | PIT1, ER +/-ve, GATA3 +/-ve | |
| PIT1 | Acidophilic stem cell tumor | PRL, GH (focal/variable), CK fibrous bodies | PIT1, ER | |
| PIT1 | Mixed somatotroph and lactotroph tumor | PRL, GH (in separate cells) | PIT1, ER (only in lactotroph component) | |
| TPIT | Corticotroph tumor | Densely and sparsely granulated tumors, Crooke cell adenoma | ACTH,CK+ve | TPIT |
| SF1 | Gonadotroph tumor | FSH, LH, a-Subunit or none | SF1, ER, GATA3, CK+/-ve | |
| None | Plurihormonal tumor | All combinations possible | All combinations possible, CK+/-ve | |
| None | Null cell adenoma | None (adenohypophyseal?) | None |
Other tumours may be classified as plurhormonal or double adenomas or as adenomas with unusual IHC combination.
General
- Clinical:[11]
- Classically: visual field defects (bitemporal hemianopsia).
- Others (increased intracranial pressure): headache, nausea, vomiting.
- Tumor of adults.
Morphologic Classification:
- Microtumor <= 1 cm.
- Macrotumor 1-4 cm.
- Giant tumor > 4cm.
May be classified by what they secrete.
- Functional (endocrine hyperfunction).
- Acromegaly/giantism.
- Hyperprolactinemia.
- Cushing disease.
- Hyperthyroidism.
- Significant elevation of FSH/LH.
- Clinically nonfunctioning.
Notes:
Cushing disease is due to pituitary gland hypersecretion of ACTH (due to a pituitary adenoma or CRH hypersecretion from the hypothalamus).[12] Cushing syndrome is hypercortisolism not due to pituitary gland pathology.
Imaging:
- Sellar enlargement.
- Bone erosion, invasive growth esp. cavernous sinus (35-45%).
- Inhomogenous signal in T1w MRI.
Familial pituitary adenomas
A pituitary adenoma may be part of a familial syndrome:[13][14]
| Syndrome | Gene | Notes |
|---|---|---|
| Multiple endocrine neoplasia I | MEN1 | characterized by the 3 Ps: pituitary adenoma, parathyroid adenoma, pancreatic neuroendocrine tumour |
| MEN-1-like syndrome | CDKN1B[15] | also known as Multiple endocrine neoplasia IV [15] |
| Carney syndrome | PRKAR1A | other findings (mnemonic NAME): nevi, atrial myxoma, myxoid neurofibroma, ephelides (freckles) |
| Isolated pituitary adenoma[16] | AIP | classically GH-producing adenoma - leads to acromegaly |
Microscopic
Features:[17]
- Loss of fibrous stroma.
- The cells of a normal (anterior) pituitary are nested.
- Basophilic cells (corticotrophs).
- Eosinophilic cells(somatotrophs).
- Extensive fibrosis often seen in TSH-producing tumors.
Notes:
- Smears very well.[18]
Images

Pituitary adenoma - non-functioning. (WC/KGH)
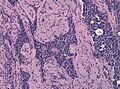
Extensive interstitial and perivascular fibrosis in a pituitary adenoma (WC/jensflorian)
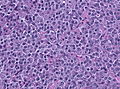
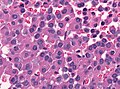
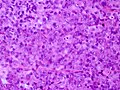
Pituitary adenoma - PRL producing, HE. Note the basophilic appearance of the cells (WC/jensflorian)
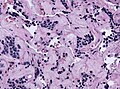
Pituitary adenoma - PRL producing, HE. Extensive regressive changes after after dopamine agonist treatment (WC/jensflorian)
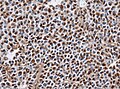
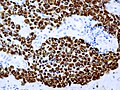
Pituitary adenoma - PRL producing, Prolactin IHC (WC/jensflorian)
Pituitary adenoma - HGH producing, HE. The cells have a slightly eosinophilic appearance (WC/jensflorian)
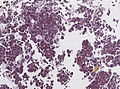
Sparsely granulated adenoma - HGH producing. Note the numerous fibrous bodies in HE stain (WC/jensflorian)
Sparsely granulated adenoma - HGH producing. CK8 IHC highlighting fibrous bodies (WC/jensflorian)
Pituitary adenoma - TSH producing. HE stain showing pleomorphism (WC/jensflorian)
Pituitary adenoma - TSH producing. TSH IHC can be heterogeneous (WC/jensflorian)
Pituitary adenoma - GH producing. (WC/KGH)
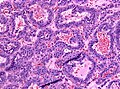
Pituitary adenoma , HE. This gonadotropin producing adenoma has a papillary architecture (WC/jensflorian)
Pituitary adenoma, IHC for FSH (WC/jensflorian)

Pituitary adenoma, IHC for LH (WC/jensflorian)
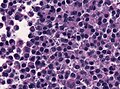
Pituitary adenoma , ACTH producing. PAS-O-G stain showing basophilic adenoma cells (WC/jensflorian)

Pituitary adenoma , ACTH producing. Strong ACTH IHC in this basophilic adenoma (WC/jensflorian)
Pituitary adenoma with vascular pseudorosettes, nonfunctioning (WC/jensflorian)
Crooke cell adenoma, HE (WC/Marvin101)
Crooke cell adenoma, panCK (WC/Marvin101)
Fibrosis in pituitary adenoma.
.jpg)









_GH_production.jpg)








Stains
- Reticulin - loss of reticulin between tumour cells.
IHC
- LH.
- FSH.
- TSH - Hyperthyroidism
- GH - Acromegaly.
- Prolactin -Galactorrhea, Amenorrhea, Gynecomastia. Golgi staining pattern in sparsely granulated cases.
- ACTH - Cushing syndrome.
- PIT-1: stains somatotrophs, lactotrophs and thyrothrops.
- TPIT: stains corticotrophs.
- SF1: stains gonadotrophs.
- Chromogranin A +ve
- Synaptophysin strongly +ve (except lactotrophs)
- CAM5.2: fibrous bodies in sparsely granulated somatotroph adenoma, Ring-like staining in Crooke cell adenoma.
- MIB-1: Usu less than 3%.
Note: Null-cell adenoma must be hormone immunonegative and negative for transcription factors.
Variants
- Corticotroph adenomas exhibiting Crooke's hyaline change: agressive course.[19]
- Acidophilic stem cell adenomas: large, locally invasive adenoma with low GH activity. [20]
- Sparsely granulated somatotroph adenomas are more invasive than other variants and respond less to medical treatment. [21]
- Lactotroph adenomas in men may show aggressive clinical behavior. [22]
- Immature PIT-1 lineage tumors may show aggresive growth. [23]
Molecular
- GNAS mutations frequently in densely granulated somatotroph tumors.
Pituitary blastoma
- New entity introduced in 2017[24]
- Epithelial glands with rosette-like formations resembling immature Rathke epithelium.
- Synaptophysin +ve, usu. ACTH+ve
- DICER1 mutations[25]
Pituitary carcinoma
- Depreceated in the WHO2022 classification.
- It is acknowledged that PitNETs can be invasive or spread to other sites.
Rathke cleft cyst
General
- Benign counterpart of craniopharyngioma.
- Arises from intermediate lobe of pituitary gland (pars intermedia of pituitary gland).
Radiology:
- Typically no calcifications.[26]
Radiologic DDx:[26]
- Arachnoid cyst.
- Craniopharyngioma.
- Cysticercosis.
- Pituitary adenoma.
- Epidermoid of brain.
Microscopic
Features:
- Lined by a layer of cuboidal or columnar epithelial with cilia.
- +/-Goblet cells.[27]
- +/-Squamous metaplasia ~ may be several layers thick.
- May be confused with papillary craniopharyngioma.[28]
- Cholesterol clefts may be seen in association with rupture.[29]
DDx:
Images:
Craniopharyngioma
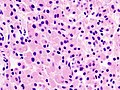
Gangliocytoma
- Neuronal cells in abundant neuropil.
- S-100, Synaptophysin +ve.
- Isolated sellar cases are very rare.
Image: [[1]]
Mixed Gangliocytoma-adenoma
AKA: ganglioneuroma, pituitary adenoma with neuronal choristoma (PANCH)
- Neuronal cells mixed with pituitary adenoma cells.
- Approx. 0.25% of all pituitary adenomas.
- Association with somatotroph adenomas (acromegaly).
Pituicytoma
Spindle cell oncocytoma
- Origin: Neurohypophysis or infundibulum.
- Benign clinical course - WHO grade I.
- Elongated bipolar, spindle cells.
- Fascicular or storiform growth patterns.
- EMA: patchy, S-100+/-ve, GFAP+/-ve, TTF1+ve.
- It is thought that Spindle cell oncocytomas and Granular cell tumors of the neurohypophysis are variants of Pituicyoma.[30]
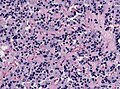
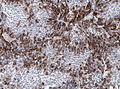
Granular cell tumor of the sellar region
- Origin: Neurohypophysis or infundibulum.
- Benign clinical course - WHO grade I.
- Well circumscribed.
- Polygonal cells with abundant granular cytoplasm.
- CD68+ve, S-100+/-ve, GFAP+/-ve, TTF1+ve.
Granular cell tumor of the sellar region (HE).

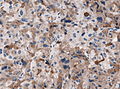
Autoimmune hypophysitis
General
Features:[31]
- Rare.
- Autoantigens are unknown.
- May occur in pregnancy.
- May be misdiagnosed as a nonsecreting adenoma.
Microscopic
Features:[31]
- Lymphocytic infiltration.
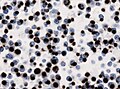
Lymphocytic hypophysitis, CD3 IHC. (WC/jensflorian)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
See also
References
- ↑ http://www.vivo.colostate.edu/hbooks/pathphys/endocrine/hypopit/histo.html
- ↑ 2.0 2.1 http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/P/Pituitary.html
- ↑ 3.0 3.1 URL: http://www.vivo.colostate.edu/hbooks/pathphys/endocrine/hypopit/histo_pit.html. Accessed on: 31 October 2010.
- ↑ 4.0 4.1 Perry, Arie; Brat, Daniel J. (2010). Practical Surgical Neuropathology: A Diagnostic Approach: A Volume in the Pattern Recognition series (1st ed.). Churchill Livingstone. pp. 26. ISBN 978-0443069826.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1098-9. ISBN 978-1416031215.
- ↑ URL: http://www.mayoclinic.com/health/sheehans-syndrome/DS00889. Accessed on: 16 November 2010.
- ↑ URL: http://pediatrics.aappublications.org/cgi/content/full/104/1/e4. Accessed on: 16 November 2010.
- ↑ Dancer CM, Woods ML, Henderson RD, Robertson T, Mungomery M, Allworth A (July 2008). "Mollaret's meningitis and pituitary failure associated with a Rathke's cleft cyst". Intern Med J 38 (7): 609–11. doi:10.1111/j.1445-5994.2008.01709.x. PMID 18715308.
- ↑ Sachdev Y, Evered DC, Hall R (April 1976). "Spontaneous pituitary necrosis". Br Med J 1 (6015): 942. PMC 1639254. PMID 1268492. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1639254/pdf/brmedj00512-0028a.pdf.
- ↑ "Overview of the 2022 WHO Classification of Pituitary Tumors". Endocr Pathol 33 (1): 6–26. March 2022. doi:10.1007/s12022-022-09703-7. PMID 35291028.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1100. ISBN 978-1416031215.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1148. ISBN 978-1416031215.
- ↑ Elston, MS.; McDonald, KL.; Clifton-Bligh, RJ.; Robinson, BG. (Aug 2009). "Familial pituitary tumor syndromes.". Nat Rev Endocrinol 5 (8): 453-61. doi:10.1038/nrendo.2009.126. PMID 19564887.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 554. ISBN 978-1416054542.
- ↑ 15.0 15.1 Online 'Mendelian Inheritance in Man' (OMIM) 600778
- ↑ Korbonits, M.; Storr, H.; Kumar, AV. (May 2012). "Familial pituitary adenomas - Who should be tested for AIP mutations?". Clin Endocrinol (Oxf). doi:10.1111/j.1365-2265.2012.04445.x. PMID 22612670.
- ↑ Perry, Arie; Brat, Daniel J. (2010). Practical Surgical Neuropathology: A Diagnostic Approach: A Volume in the Pattern Recognition series (1st ed.). Churchill Livingstone. pp. 36. ISBN 978-0443069826.
- ↑ MUN. 24 November 2010.
- ↑ George, DH.; Scheithauer, BW.; Kovacs, K.; Horvath, E.; Young, WF.; Lloyd, RV.; Meyer, FB. (Oct 2003). "Crooke's cell adenoma of the pituitary: an aggressive variant of corticotroph adenoma.". Am J Surg Pathol 27 (10): 1330-6. PMID 14508394.
- ↑ Horvath, E.; Kovacs, K.; Singer, W.; Smyth, HS.; Killinger, DW.; Erzin, C.; Weiss, MH. (Feb 1981). "Acidophil stem cell adenoma of the human pituitary: clinicopathologic analysis of 15 cases.". Cancer 47 (4): 761-71. PMID 6261917.
- ↑ Kato, M.; Inoshita, N.; Sugiyama, T.; Tani, Y.; Shichiri, M.; Sano, T.; Yamada, S.; Hirata, Y. (2012). "Differential expression of genes related to drug responsiveness between sparsely and densely granulated somatotroph adenomas.". Endocr J 59 (3): 221-8. PMID 22200580.
- ↑ Delgrange, E.; Vasiljevic, A.; Wierinckx, A.; François, P.; Jouanneau, E.; Raverot, G.; Trouillas, J. (Jun 2015). "Expression of estrogen receptor alpha is associated with prolactin pituitary tumor prognosis and supports the sex-related difference in tumor growth.". Eur J Endocrinol 172 (6): 791-801. doi:10.1530/EJE-14-0990. PMID 25792376.
- ↑ Mete, O.; Gomez-Hernandez, K.; Kucharczyk, W.; Ridout, R.; Zadeh, G.; Gentili, F.; Ezzat, S.; Asa, SL. (Feb 2016). "Silent subtype 3 pituitary adenomas are not always silent and represent poorly differentiated monomorphous plurihormonal Pit-1 lineage adenomas.". Mod Pathol 29 (2): 131-42. doi:10.1038/modpathol.2015.151. PMID 26743473.
- ↑ Lopes, MBS. (Oct 2017). "The 2017 World Health Organization classification of tumors of the pituitary gland: a summary.". Acta Neuropathol 134 (4): 521-535. doi:10.1007/s00401-017-1769-8. PMID 28821944.
- ↑ de Kock, L.; Sabbaghian, N.; Plourde, F.; Srivastava, A.; Weber, E.; Bouron-Dal Soglio, D.; Hamel, N.; Choi, JH. et al. (Jul 2014). "Pituitary blastoma: a pathognomonic feature of germ-line DICER1 mutations.". Acta Neuropathol 128 (1): 111-22. doi:10.1007/s00401-014-1285-z. PMID 24839956.
- ↑ 26.0 26.1 URL: http://emedicine.medscape.com/article/343629-overview. Accessed on: 14 November 2010.
- ↑ URL: http://www.endotext.org/neuroendo/neuroendo3/neuroendo3.html. Accessed on: 27 May 2010.
- ↑ Perry, Arie; Brat, Daniel J. (2010). Practical Surgical Neuropathology: A Diagnostic Approach: A Volume in the Pattern Recognition series (1st ed.). Churchill Livingstone. pp. 408. ISBN 978-0443069826.
- ↑ URL: http://path.upmc.edu/cases/case177/dx.html. Accessed on: 8 January 2012.
- ↑ Mete, O.; Lopes, MB.; Asa, SL. (Nov 2013). "Spindle cell oncocytomas and granular cell tumors of the pituitary are variants of pituicytoma.". Am J Surg Pathol 37 (11): 1694-9. doi:10.1097/PAS.0b013e31829723e7. PMID 23887161.
- ↑ 31.0 31.1 Tzou SC, Lupi I, Landek M, et al. (July 2008). "Autoimmune hypophysitis of SJL mice: clinical insights from a new animal model". Endocrinology 149 (7): 3461–9. doi:10.1210/en.2007-1692. PMC 2453094. PMID 18388197. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2453094/.
External links
- Neuropathology - neuropathologyweb.org.
- Endocrine histology (anhb.uwa.edu.au).