Difference between revisions of "P16"
Jump to navigation
Jump to search

| (26 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
{{ Infobox immunostain | |||
[[Image:Endocervical adenocarcinoma in situ - p16 --- high mag.jpg|thumb|right|AIS showing the characteristic p16 staining.]] | | Name = {{PAGENAME}} | ||
| Image = High grade squamous intraepithelial lesion - 2 - p16 -- high mag.jpg | |||
| Width = | |||
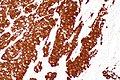
| Caption = [[HSIL]] showing the characteristic p16 staining. (WC/Nephron) | |||
| Abbrev = | |||
| Synonyms = | |||
| Similar = [[HPV]] | |||
| Clones = | |||
| Use = [[HSIL]] versus [[LSIL]], HPV associated SCC versus non-HPV associated SCC | |||
| Subspecial = [[gynecologic pathology]], [[head and neck pathology]] | |||
| Pattern = nuclear and cytoplasmic | |||
| Positive = endometrial tubal metaplasia, [[cervical SCC]], [[HPV-associated head and neck SCC]], [[serous carcinoma of the endometrium]] | |||
| Negative = | |||
| Other = | |||
}} | |||
[[Image:Endocervical adenocarcinoma in situ - p16 --- high mag.jpg|thumb|right|250px|[[Endocervical AIS]] showing the characteristic p16 staining.]] | |||
'''p16''' is a commonly used [[immunostain]]. It can be considered a surrogate marker for [[HPV]] infection. | '''p16''' is a commonly used [[immunostain]]. It can be considered a surrogate marker for [[HPV]] infection. | ||
p16, like most other "p" stains, is a nuclear stain. | p16, like most other "p" stains, is a nuclear stain. The antibody target is a cell cycle protein, cyclin-dependent kinase inhibitor 2A, sometimes denoted p16<sup>INK4a</sup>. | ||
==Pattern== | ==Pattern== | ||
| Line 10: | Line 25: | ||
*Squamous lesions of the [[uterine cervix]] - see [[HSIL]]. | *Squamous lesions of the [[uterine cervix]] - see [[HSIL]]. | ||
*Head and neck squamous cell carcinoma, specifically ''[[human papillomavirus-associated head and neck squamous cell carcinoma]]''. | *Head and neck squamous cell carcinoma, specifically ''[[human papillomavirus-associated head and neck squamous cell carcinoma]]''. | ||
*Increased expression in well-differentiated liposarcoma.<ref>{{Cite journal | last1 = Thway | first1 = K. | last2 = Flora | first2 = R. | last3 = Shah | first3 = C. | last4 = Olmos | first4 = D. | last5 = Fisher | first5 = C. | title = Diagnostic utility of p16, CDK4, and MDM2 as an immunohistochemical panel in distinguishing well-differentiated and dedifferentiated liposarcomas from other adipocytic tumors. | journal = Am J Surg Pathol | volume = 36 | issue = 3 | pages = 462-9 | month = Mar | year = 2012 | doi = 10.1097/PAS.0b013e3182417330 | PMID = 22301498 }}</ref> | |||
*Limited use in melanocytic lesions.<ref>{{Cite journal | last1 = Koh | first1 = SS. | last2 = Cassarino | first2 = DS. | title = Immunohistochemical Expression of p16 in Melanocytic Lesions: An Updated Review and Meta-analysis. | journal = Arch Pathol Lab Med | volume = 142 | issue = 7 | pages = 815-828 | month = Jul | year = 2018 | doi = 10.5858/arpa.2017-0435-RA | PMID = 29939777 }}</ref> | |||
== | ===Head and neck squamous cell carcinoma=== | ||
===Positive=== | p16 testing is useful in: | ||
*[[Squamous cell carcinoma]] - esp. cervical SCC, anal SCC, penile SCC, HPV-associated head and neck SCC. | #[[Lymph node metastases]] with an [[unknown primary]] - positivity suggests an oropharyngeal primary. | ||
#Oropharyngeal carcinomas. | |||
Note: | |||
*Like elsewhere, i.e. other anatomical sites, p16 is an imperfect surrogate marker for the presence of ''[[HPV]]''.<ref name=pmid23935769/> | |||
*Non-oropharyngeal sites ([[oral cavity]], [[larynx]], and hypopharynx) are not well-studied; however, it is known that p16 positivity is much less common in there.<ref name=pmid23935769>{{Cite journal | last1 = Stephen | first1 = JK. | last2 = Divine | first2 = G. | last3 = Chen | first3 = KM. | last4 = Chitale | first4 = D. | last5 = Havard | first5 = S. | last6 = Worsham | first6 = MJ. | title = Significance of p16 in Site-specific HPV Positive and HPV Negative Head and Neck Squamous Cell Carcinoma. | journal = Cancer Clin Oncol | volume = 2 | issue = 1 | pages = 51-61 | month = | year = 2013 | doi = 10.5539/cco.v2n1p51 | PMID = 23935769 }}</ref> | |||
====Images==== | |||
<gallery> | |||
Image:Consistent with HPV-associated SCC - p16 -- intermed mag.jpg | c/w HPV-assoc. SCC - p16 - intermed. mag. (WC/Nephron) | |||
Image:Consistent with HPV-associated SCC - p16 -- high mag.jpg | c/w HPV-assoc. SCC - p16 - high mag. (WC/Nephron) | |||
</gallery> | |||
==Positive== | |||
*[[Squamous cell carcinoma]] - esp. [[cervical SCC]], anal SCC, penile SCC, [[HPV-associated head and neck SCC]]. | |||
*High grade [[urothelial carcinoma]] ~86% of cases by PCR.<ref name=pmid25069600>{{Cite journal | last1 = Piaton | first1 = E. | last2 = Casalegno | first2 = JS. | last3 = Advenier | first3 = AS. | last4 = Decaussin-Petrucci | first4 = M. | last5 = Mege-Lechevallier | first5 = F. | last6 = Ruffion | first6 = A. | last7 = Mekki | first7 = Y. | title = p16(INK4a) overexpression is not linked to oncogenic human papillomaviruses in patients with high-grade urothelial cancer cells. | journal = Cancer Cytopathol | volume = 122 | issue = 10 | pages = 760-9 | month = Oct | year = 2014 | doi = 10.1002/cncy.21462 | PMID = 25069600 }}</ref> | *High grade [[urothelial carcinoma]] ~86% of cases by PCR.<ref name=pmid25069600>{{Cite journal | last1 = Piaton | first1 = E. | last2 = Casalegno | first2 = JS. | last3 = Advenier | first3 = AS. | last4 = Decaussin-Petrucci | first4 = M. | last5 = Mege-Lechevallier | first5 = F. | last6 = Ruffion | first6 = A. | last7 = Mekki | first7 = Y. | title = p16(INK4a) overexpression is not linked to oncogenic human papillomaviruses in patients with high-grade urothelial cancer cells. | journal = Cancer Cytopathol | volume = 122 | issue = 10 | pages = 760-9 | month = Oct | year = 2014 | doi = 10.1002/cncy.21462 | PMID = 25069600 }}</ref> | ||
*[[Serous carcinoma of the endometrium]] - should be strong.<ref name=pmid17581420>{{Cite journal | last1 = Chiesa-Vottero | first1 = AG. | last2 = Malpica | first2 = A. | last3 = Deavers | first3 = MT. | last4 = Broaddus | first4 = R. | last5 = Nuovo | first5 = GJ. | last6 = Silva | first6 = EG. | title = Immunohistochemical overexpression of p16 and p53 in uterine serous carcinoma and ovarian high-grade serous carcinoma. | journal = Int J Gynecol Pathol | volume = 26 | issue = 3 | pages = 328-33 | month = Jul | year = 2007 | doi = 10.1097/01.pgp.0000235065.31301.3e | PMID = 17581420 }}</ref> | |||
*[[High-grade squamous intraepithelial lesion]] - full thickness, strong. | |||
**A subset of LSIL stains with p16; however, it is ''not'' full thickness - see ''[[HSIL]]'' article. | |||
*[[Small cell carcinoma of the lung]] - most cases (95 of 101 cases in one series<ref name=pmid29566943>{{cite journal |authors=Švajdler M, Mezencev R, Ondič O, Šašková B, Mukenšnábl P, Michal M |title=P16 is a useful supplemental diagnostic marker of pulmonary small cell carcinoma in small biopsies and cytology specimens |journal=Ann Diagn Pathol |volume=33 |issue= |pages=23–29 |date=April 2018 |pmid=29566943 |doi=10.1016/j.anndiagpath.2017.11.008 |url=}}</ref>). | |||
Note: | |||
*Positive staining (in the head and neck pathology context) is defined as (strong block) positive staining in >75% (or >50%) of lesional cells.<ref name=pmid28621317>{{cite journal |authors=Shelton J, Purgina BM, Cipriani NA, Dupont WD, Plummer D, Lewis JS |title=p16 immunohistochemistry in oropharyngeal squamous cell carcinoma: a comparison of antibody clones using patient outcomes and high-risk human papillomavirus RNA status |journal=Mod Pathol |volume=30 |issue=9 |pages=1194–1203 |date=September 2017 |pmid=28621317 |doi=10.1038/modpathol.2017.31 |url=}}</ref> | |||
**Staining varies somewhat by the p16 clone used. | |||
===Benign=== | |||
*p16 endometrial tubal metaplasia.<ref name=pmid17429140>{{Cite journal | last1 = Horree | first1 = N. | last2 = Heintz | first2 = AP. | last3 = Sie-Go | first3 = DM. | last4 = van Diest | first4 = PJ. | title = p16 is consistently expressed in endometrial tubal metaplasia. | journal = Cell Oncol | volume = 29 | issue = 1 | pages = 37-45 | month = | year = 2007 | doi = | PMID = 17429140 }}</ref> | |||
====Focal staining==== | |||
*[[Endometriosis]] - focal/weak staining may be seen.<ref name=pmid26095917>{{Cite journal | last1 = Stewart | first1 = CJ. | last2 = Bharat | first2 = C. | title = Clinicopathological and immunohistological features of polypoid endometriosis. | journal = Histopathology | volume = 68 | issue = 3 | pages = 398-404 | month = Feb | year = 2016 | doi = 10.1111/his.12755 | PMID = 26095917 }}</ref><ref name=pmid16462152>{{Cite journal | last1 = O'Neill | first1 = CJ. | last2 = McCluggage | first2 = WG. | title = p16 expression in the female genital tract and its value in diagnosis. | journal = Adv Anat Pathol | volume = 13 | issue = 1 | pages = 8-15 | month = Jan | year = 2006 | doi = 10.1097/01.pap.0000201828.92719.f3 | PMID = 16462152 }}</ref> | |||
==Negative== | |||
*Breast carcinoma. | <!-- *Breast carcinoma. --> | ||
*[[Prostate carcinoma]]. | <!-- *[[Prostate carcinoma]]. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3267667/ --> | ||
*[[Lung squamous cell carcinoma]] | *[[Lung squamous cell carcinoma]]<ref name=pmid20823766>{{Cite journal | last1 = Pereira | first1 = TC. | last2 = Share | first2 = SM. | last3 = Magalhães | first3 = AV. | last4 = Silverman | first4 = JF. | title = Can we tell the site of origin of metastatic squamous cell carcinoma? An immunohistochemical tissue microarray study of 194 cases. | journal = Appl Immunohistochem Mol Morphol | volume = 19 | issue = 1 | pages = 10-4 | month = Jan | year = 2011 | doi = 10.1097/PAI.0b013e3181ecaf1c | PMID = 20823766 }}</ref> - 21% positive (7/33).<ref name=pmid19369633>{{Cite journal | last1 = Wang | first1 = CW. | last2 = Wu | first2 = TI. | last3 = Yu | first3 = CT. | last4 = Wu | first4 = YC. | last5 = Teng | first5 = YH. | last6 = Chin | first6 = SY. | last7 = Lai | first7 = CH. | last8 = Chen | first8 = TC. | title = Usefulness of p16 for differentiating primary pulmonary squamous cell carcinoma from cervical squamous cell carcinoma metastatic to the lung. | journal = Am J Clin Pathol | volume = 131 | issue = 5 | pages = 715-22 | month = May | year = 2009 | doi = 10.1309/AJCPTPBC6V5KUITM | PMID = 19369633 }}</ref> | ||
==References== | ==References== | ||
Latest revision as of 15:59, 25 November 2021
| P16 | |
|---|---|
| Immunostain in short | |
 HSIL showing the characteristic p16 staining. (WC/Nephron) | |
| Similar stains | HPV |
| Use | HSIL versus LSIL, HPV associated SCC versus non-HPV associated SCC |
| Subspeciality | gynecologic pathology, head and neck pathology |
| Normal staining pattern | nuclear and cytoplasmic |
| Positive | endometrial tubal metaplasia, cervical SCC, HPV-associated head and neck SCC, serous carcinoma of the endometrium |

Endocervical AIS showing the characteristic p16 staining.
p16 is a commonly used immunostain. It can be considered a surrogate marker for HPV infection. p16, like most other "p" stains, is a nuclear stain. The antibody target is a cell cycle protein, cyclin-dependent kinase inhibitor 2A, sometimes denoted p16INK4a.
Pattern
- Nuclear stain +/- cytoplasmic staining.
Use
- Squamous lesions of the uterine cervix - see HSIL.
- Head and neck squamous cell carcinoma, specifically human papillomavirus-associated head and neck squamous cell carcinoma.
- Increased expression in well-differentiated liposarcoma.[1]
- Limited use in melanocytic lesions.[2]
Head and neck squamous cell carcinoma
p16 testing is useful in:
- Lymph node metastases with an unknown primary - positivity suggests an oropharyngeal primary.
- Oropharyngeal carcinomas.
Note:
- Like elsewhere, i.e. other anatomical sites, p16 is an imperfect surrogate marker for the presence of HPV.[3]
- Non-oropharyngeal sites (oral cavity, larynx, and hypopharynx) are not well-studied; however, it is known that p16 positivity is much less common in there.[3]
Images
c/w HPV-assoc. SCC - p16 - intermed. mag. (WC/Nephron)
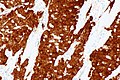
c/w HPV-assoc. SCC - p16 - high mag. (WC/Nephron)


Positive
- Squamous cell carcinoma - esp. cervical SCC, anal SCC, penile SCC, HPV-associated head and neck SCC.
- High grade urothelial carcinoma ~86% of cases by PCR.[4]
- Serous carcinoma of the endometrium - should be strong.[5]
- High-grade squamous intraepithelial lesion - full thickness, strong.
- A subset of LSIL stains with p16; however, it is not full thickness - see HSIL article.
- Small cell carcinoma of the lung - most cases (95 of 101 cases in one series[6]).
Note:
- Positive staining (in the head and neck pathology context) is defined as (strong block) positive staining in >75% (or >50%) of lesional cells.[7]
- Staining varies somewhat by the p16 clone used.
Benign
- p16 endometrial tubal metaplasia.[8]
Focal staining
- Endometriosis - focal/weak staining may be seen.[9][10]
Negative
- Lung squamous cell carcinoma[11] - 21% positive (7/33).[12]
References
- ↑ Thway, K.; Flora, R.; Shah, C.; Olmos, D.; Fisher, C. (Mar 2012). "Diagnostic utility of p16, CDK4, and MDM2 as an immunohistochemical panel in distinguishing well-differentiated and dedifferentiated liposarcomas from other adipocytic tumors.". Am J Surg Pathol 36 (3): 462-9. doi:10.1097/PAS.0b013e3182417330. PMID 22301498.
- ↑ Koh, SS.; Cassarino, DS. (Jul 2018). "Immunohistochemical Expression of p16 in Melanocytic Lesions: An Updated Review and Meta-analysis.". Arch Pathol Lab Med 142 (7): 815-828. doi:10.5858/arpa.2017-0435-RA. PMID 29939777.
- ↑ 3.0 3.1 Stephen, JK.; Divine, G.; Chen, KM.; Chitale, D.; Havard, S.; Worsham, MJ. (2013). "Significance of p16 in Site-specific HPV Positive and HPV Negative Head and Neck Squamous Cell Carcinoma.". Cancer Clin Oncol 2 (1): 51-61. doi:10.5539/cco.v2n1p51. PMID 23935769.
- ↑ Piaton, E.; Casalegno, JS.; Advenier, AS.; Decaussin-Petrucci, M.; Mege-Lechevallier, F.; Ruffion, A.; Mekki, Y. (Oct 2014). "p16(INK4a) overexpression is not linked to oncogenic human papillomaviruses in patients with high-grade urothelial cancer cells.". Cancer Cytopathol 122 (10): 760-9. doi:10.1002/cncy.21462. PMID 25069600.
- ↑ Chiesa-Vottero, AG.; Malpica, A.; Deavers, MT.; Broaddus, R.; Nuovo, GJ.; Silva, EG. (Jul 2007). "Immunohistochemical overexpression of p16 and p53 in uterine serous carcinoma and ovarian high-grade serous carcinoma.". Int J Gynecol Pathol 26 (3): 328-33. doi:10.1097/01.pgp.0000235065.31301.3e. PMID 17581420.
- ↑ Švajdler M, Mezencev R, Ondič O, Šašková B, Mukenšnábl P, Michal M (April 2018). "P16 is a useful supplemental diagnostic marker of pulmonary small cell carcinoma in small biopsies and cytology specimens". Ann Diagn Pathol 33: 23–29. doi:10.1016/j.anndiagpath.2017.11.008. PMID 29566943.
- ↑ Shelton J, Purgina BM, Cipriani NA, Dupont WD, Plummer D, Lewis JS (September 2017). "p16 immunohistochemistry in oropharyngeal squamous cell carcinoma: a comparison of antibody clones using patient outcomes and high-risk human papillomavirus RNA status". Mod Pathol 30 (9): 1194–1203. doi:10.1038/modpathol.2017.31. PMID 28621317.
- ↑ Horree, N.; Heintz, AP.; Sie-Go, DM.; van Diest, PJ. (2007). "p16 is consistently expressed in endometrial tubal metaplasia.". Cell Oncol 29 (1): 37-45. PMID 17429140.
- ↑ Stewart, CJ.; Bharat, C. (Feb 2016). "Clinicopathological and immunohistological features of polypoid endometriosis.". Histopathology 68 (3): 398-404. doi:10.1111/his.12755. PMID 26095917.
- ↑ O'Neill, CJ.; McCluggage, WG. (Jan 2006). "p16 expression in the female genital tract and its value in diagnosis.". Adv Anat Pathol 13 (1): 8-15. doi:10.1097/01.pap.0000201828.92719.f3. PMID 16462152.
- ↑ Pereira, TC.; Share, SM.; Magalhães, AV.; Silverman, JF. (Jan 2011). "Can we tell the site of origin of metastatic squamous cell carcinoma? An immunohistochemical tissue microarray study of 194 cases.". Appl Immunohistochem Mol Morphol 19 (1): 10-4. doi:10.1097/PAI.0b013e3181ecaf1c. PMID 20823766.
- ↑ Wang, CW.; Wu, TI.; Yu, CT.; Wu, YC.; Teng, YH.; Chin, SY.; Lai, CH.; Chen, TC. (May 2009). "Usefulness of p16 for differentiating primary pulmonary squamous cell carcinoma from cervical squamous cell carcinoma metastatic to the lung.". Am J Clin Pathol 131 (5): 715-22. doi:10.1309/AJCPTPBC6V5KUITM. PMID 19369633.