Difference between revisions of "Neuroendocrine neoplasms"
m (→IHC - generic) |
|||
| (20 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
'''Neuroendocrine neoplasms''', also '''neuroendocrine tumours''', are a group of tumours whose behaviour varies from benign to malignant and are found in may different sites. | [[Image:Small intestine neuroendocrine tumour high mag.jpg|thumb|right|200px|Micrograph of a neuroendocrine tumour of the small bowel. [[H&E stain]].]] | ||
'''Neuroendocrine neoplasms''', also '''neuroendocrine tumours''', are a group of tumours whose behaviour varies from benign to malignant and are found in may different sites. ''Neuroendocrine tumour'' is commonly abbreviated '''NET'''. | |||
These tumours arise from epithelium; thus, malignant tumours in this group are referred to as '''neuroendocrine carcinomas'''. | These tumours arise from epithelium; thus, malignant tumours in this group are referred to as '''neuroendocrine carcinomas'''. | ||
| Line 13: | Line 14: | ||
===Pathophysiology=== | ===Pathophysiology=== | ||
*Neuroendocrine tumour -> hormone secretion (5-hydroxytryptamine + others).<ref name=pmid19444261>{{Cite journal | last1 = Druce | first1 = M. | last2 = Rockall | first2 = A. | last3 = Grossman | first3 = AB. | title = Fibrosis and carcinoid syndrome: from causation to future therapy. | journal = Nat Rev Endocrinol | volume = 5 | issue = 5 | pages = 276-83 | month = May | year = 2009 | doi = 10.1038/nrendo.2009.51 | PMID = 19444261 }}</ref> | *Neuroendocrine tumour -> hormone secretion (5-hydroxytryptamine + others).<ref name=pmid19444261>{{Cite journal | last1 = Druce | first1 = M. | last2 = Rockall | first2 = A. | last3 = Grossman | first3 = AB. | title = Fibrosis and carcinoid syndrome: from causation to future therapy. | journal = Nat Rev Endocrinol | volume = 5 | issue = 5 | pages = 276-83 | month = May | year = 2009 | doi = 10.1038/nrendo.2009.51 | PMID = 19444261 }}</ref> | ||
*In GI NETs ''carcinoid syndrome'' usually only arises in the context of liver metastases. | |||
**GI NETs without liver mets do not develop the syndrome due to ''first pass effect'' of the liver. | |||
**Exceptions to the rule -- carcinoid syndrome without liver mets: ovarian NETs, testicular NETs, bronchial NETs.<ref name=pmid1574032>{{Cite journal | last1 = Haq | first1 = AU. | last2 = Yook | first2 = CR. | last3 = Hiremath | first3 = V. | last4 = Kasimis | first4 = BS. | title = Carcinoid syndrome in the absence of liver metastasis: a case report and review of literature. | journal = Med Pediatr Oncol | volume = 20 | issue = 3 | pages = 221-3 | month = | year = 1992 | doi = | PMID = 1574032 }}</ref> | |||
===Clinical=== | ===Clinical=== | ||
| Line 32: | Line 36: | ||
DDx: | DDx: | ||
*[[Paraganglioma]]. | *[[Paraganglioma]]. | ||
*Neoplasm with neuroendocrine differentiation (<30% neuroendocrine component<ref name=pmid26556999>{{Cite journal | last1 = Kleist | first1 = B. | last2 = Poetsch | first2 = M. | title = Neuroendocrine differentiation: The mysterious fellow of colorectal cancer. | journal = World J Gastroenterol | volume = 21 | issue = 41 | pages = 11740-7 | month = Nov | year = 2015 | doi = 10.3748/wjg.v21.i41.11740 | PMID = 26556999 }}</ref>). | |||
Images | ==Images== | ||
<gallery> | |||
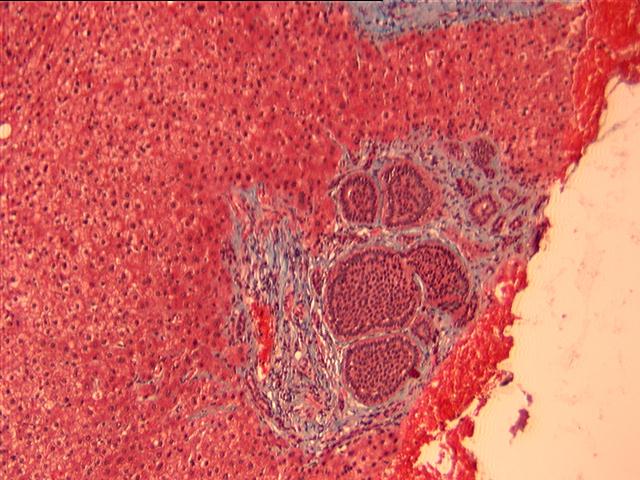
Image:Small_intestine_neuroendocrine_tumour_low_mag.jpg | Neuroendocrine tumour - low mag. (WC/Nephron) | |||
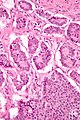
Image:Small_intestine_neuroendocrine_tumour_intermed_mag.jpg | Neuroendocrine tumour - intermed. mag. (WC/Nephron) | |||
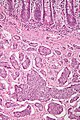
Image:Small_intestine_neuroendocrine_tumour_high_mag.jpg | Neuroendocrine tumour - high mag. (WC/Nephron) | |||
</gallery> | |||
www: | |||
*[http://path.upmc.edu/cases/case7/images/micro3.jpg NET met to liver (upmc.edu)].<ref>URL: [http://path.upmc.edu/cases/case7.html http://path.upmc.edu/cases/case7.html}. Accessed on: 17 December 2011.</ref> | |||
=IHC - generic= | =IHC - generic= | ||
Key stains:<ref name=pmid17204019>{{Cite journal | last1 = Williams | first1 = GT. | title = Endocrine tumours of the gastrointestinal tract-selected topics. | journal = Histopathology | volume = 50 | issue = 1 | pages = 30-41 | month = Jan | year = 2007 | doi = 10.1111/j.1365-2559.2006.02570.x | PMID = 17204019 }}</ref> | |||
*Chromogranin A +ve. | *Chromogranin A +ve. | ||
**Considered the most specific neuroendocrine stain.<ref name=pmid20182342>{{Cite journal | last1 = McCluggage | first1 = WG. | last2 = Kennedy | first2 = K. | last3 = Busam | first3 = KJ. | title = An immunohistochemical study of cervical neuroendocrine carcinomas: Neoplasms that are commonly TTF1 positive and which may express CK20 and P63. | journal = Am J Surg Pathol | volume = 34 | issue = 4 | pages = 525-32 | month = Apr | year = 2010 | doi = 10.1097/PAS.0b013e3181d1d457 | PMID = 20182342 }}</ref> | |||
*Synaptophysin +ve. | *Synaptophysin +ve. | ||
Others: | Others: | ||
*NSE +ve. | *NSE +ve. | ||
*CD56 +ve. | *[[CD56]] +ve. | ||
*Ki-67 - useful for grading. | *[[Ki-67]] - useful for grading. | ||
*PGP9.5.<ref name=pmid20182342/> | |||
*[[CDX2]] -ve/+ve. | |||
**+ve suggests ileum, appendix or colon origin.<ref name=pmid22180832>{{Cite journal | last1 = Saad | first1 = RS. | last2 = Ghorab | first2 = Z. | last3 = Khalifa | first3 = MA. | last4 = Xu | first4 = M. | title = CDX2 as a marker for intestinal differentiation: Its utility and limitations. | journal = World J Gastrointest Surg | volume = 3 | issue = 11 | pages = 159-66 | month = Nov | year = 2011 | doi = 10.4240/wjgs.v3.i11.159 | PMID = 22180832 }}</ref> | |||
*Serotonin -ve/+ve. | |||
**+ve suggests jejuno-ileal origin.{{fact}} | |||
Hormone products: | |||
*Glucagon +ve/-ve. | |||
*Gastrin +ve/-ve. | |||
*Somatostatin +ve/-ve. | |||
=Site specific= | =Site specific= | ||
==Lung== | ==Lung== | ||
{{Main|Lung_tumours#Neuroendocrine_tumours}} | {{Main|Lung_tumours#Neuroendocrine_tumours}} | ||
==Genitourinary pathology== | |||
{{Main|Small cell carcinoma of the prostate gland}} | |||
{{Main|Small cell carcinoma of the urinary bladder}} | |||
==Gastrointestinal tract== | ==Gastrointestinal tract== | ||
| Line 74: | Line 95: | ||
===Stomach=== | ===Stomach=== | ||
{{Main|Gastric neuroendocrine tumour}} | |||
{| | |||
===Duodenum=== | ===Duodenum=== | ||
{{Main| | {{Main|Duodenal neuroendocrine tumour}} | ||
===Pancreatic=== | ===Pancreatic=== | ||
{{Main|Pancreatic neuroendocrine tumour}} | {{Main|Pancreatic neuroendocrine tumour}} | ||
===Vermiform appendix=== | |||
{{Main|Appendiceal neuroendocrine tumour}} | |||
=See also= | =See also= | ||
*[[Basics]]. | *[[Basics]]. | ||
*[[Goblet cell carcinoid]]. | *[[Goblet cell carcinoid]]. | ||
*[[Mixed neuroendocrine-nonneuroendocrine neoplasm]] (MiNEN). | |||
=References= | =References= | ||
Latest revision as of 19:55, 5 December 2023

Neuroendocrine neoplasms, also neuroendocrine tumours, are a group of tumours whose behaviour varies from benign to malignant and are found in may different sites. Neuroendocrine tumour is commonly abbreviated NET.
These tumours arise from epithelium; thus, malignant tumours in this group are referred to as neuroendocrine carcinomas.
Use of the term carcinoid
Use of the term carcinoid is discouraged (in pathology reports), in the context of gastrointestinal pathology.[1][2][3]
The term is still used for neuroendocrine tumours of the lung - see carcinoid tumours.
Carcinoid syndrome
Pathophysiology
- Neuroendocrine tumour -> hormone secretion (5-hydroxytryptamine + others).[4]
- In GI NETs carcinoid syndrome usually only arises in the context of liver metastases.
- GI NETs without liver mets do not develop the syndrome due to first pass effect of the liver.
- Exceptions to the rule -- carcinoid syndrome without liver mets: ovarian NETs, testicular NETs, bronchial NETs.[5]
Clinical
Features:[4]
- Diarrhea, flushing and wheezing.
Pathologic findings
Classic pathologic finding:[4]
- Fibrosis of cardiac valves (tricuspid and pulmonary).
- Result TIPS = tricuspid insufficiency pulmonary stenosis.
Microscopic - generic
Features:
- Nests of cells - with fibrous stroma in between.
- May have a trabecular architecture.
- Stippled chromatin AKA salt-and-pepper chromatin, coarse chromatin.
- Classically subepithelial/mural.
DDx:
- Paraganglioma.
- Neoplasm with neuroendocrine differentiation (<30% neuroendocrine component[6]).
Images

Neuroendocrine tumour - low mag. (WC/Nephron)
Neuroendocrine tumour - intermed. mag. (WC/Nephron)
Neuroendocrine tumour - high mag. (WC/Nephron)


www:
{kind=link}
IHC - generic
Key stains:[8]
- Chromogranin A +ve.
- Considered the most specific neuroendocrine stain.[9]
- Synaptophysin +ve.
Others:
- NSE +ve.
- CD56 +ve.
- Ki-67 - useful for grading.
- PGP9.5.[9]
- CDX2 -ve/+ve.
- +ve suggests ileum, appendix or colon origin.[10]
- Serotonin -ve/+ve.
- +ve suggests jejuno-ileal origin.[citation needed]
Hormone products:
- Glucagon +ve/-ve.
- Gastrin +ve/-ve.
- Somatostatin +ve/-ve.
Site specific
Lung
Genitourinary pathology
Gastrointestinal tract
WHO classification for digestive NET
Subtypes:[11]
- Neuroendocrine tumour G1.
- Neuroendocrine tumour G2.
- Neuroendocrine carcinoma, small cell type.
- Neuroendocrine carcinoma, large cell type.
- Mixed adenoneuroendocrine carcinoma.
Grading
Grading of NETs:[12]
- Grade 1 (G1): < 2 mitoses/2 mm^2 or < 3% Ki-67.
- Grade 2 (G2): > 2 mitoses/2 mm^2 or > 3% Ki-67 and < 20 mitoses/2 mm^2 or < 20% Ki-67.
- Grade 3 (G3): > 20 mitoses/2 mm^2 or > 20% Ki-67.
Notes:
- Neuroendocrine carcinomas are G3 by definition.
Stomach
Duodenum
Pancreatic
Vermiform appendix
See also
References
- ↑ Chetty, R. (Apr 2008). "Requiem for the term 'carcinoid tumour' in the gastrointestinal tract?". Can J Gastroenterol 22 (4): 357-8. PMID 18414708.
- ↑ Klöppel, G.; Perren, A.; Heitz, PU. (Apr 2004). "The gastroenteropancreatic neuroendocrine cell system and its tumors: the WHO classification.". Ann N Y Acad Sci 1014: 13-27. PMID 15153416.
- ↑ Klöppel G (July 2003). "[Neuroendocrine tumors of the gastrointestinal tract]" (in German). Pathologe 24 (4): 287–96. doi:10.1007/s00292-003-0636-7. PMID 14513276.
- ↑ 4.0 4.1 4.2 Druce, M.; Rockall, A.; Grossman, AB. (May 2009). "Fibrosis and carcinoid syndrome: from causation to future therapy.". Nat Rev Endocrinol 5 (5): 276-83. doi:10.1038/nrendo.2009.51. PMID 19444261.
- ↑ Haq, AU.; Yook, CR.; Hiremath, V.; Kasimis, BS. (1992). "Carcinoid syndrome in the absence of liver metastasis: a case report and review of literature.". Med Pediatr Oncol 20 (3): 221-3. PMID 1574032.
- ↑ Kleist, B.; Poetsch, M. (Nov 2015). "Neuroendocrine differentiation: The mysterious fellow of colorectal cancer.". World J Gastroenterol 21 (41): 11740-7. doi:10.3748/wjg.v21.i41.11740. PMID 26556999.
- ↑ URL: [http://path.upmc.edu/cases/case7.html http://path.upmc.edu/cases/case7.html}. Accessed on: 17 December 2011.
- ↑ Williams, GT. (Jan 2007). "Endocrine tumours of the gastrointestinal tract-selected topics.". Histopathology 50 (1): 30-41. doi:10.1111/j.1365-2559.2006.02570.x. PMID 17204019.
- ↑ 9.0 9.1 McCluggage, WG.; Kennedy, K.; Busam, KJ. (Apr 2010). "An immunohistochemical study of cervical neuroendocrine carcinomas: Neoplasms that are commonly TTF1 positive and which may express CK20 and P63.". Am J Surg Pathol 34 (4): 525-32. doi:10.1097/PAS.0b013e3181d1d457. PMID 20182342.
- ↑ Saad, RS.; Ghorab, Z.; Khalifa, MA.; Xu, M. (Nov 2011). "CDX2 as a marker for intestinal differentiation: Its utility and limitations.". World J Gastrointest Surg 3 (11): 159-66. doi:10.4240/wjgs.v3.i11.159. PMID 22180832.
- ↑ Scoazec, JY.; Couvelard, A. (Apr 2011). "[The new WHO classification of digestive neuroendocrine tumors].". Ann Pathol 31 (2): 88-92. doi:10.1016/j.annpat.2011.01.001. PMID 21601112.
- ↑ Volante, M.; Righi, L.; Berruti, A.; Rindi, G.; Papotti, M. (Apr 2011). "The pathological diagnosis of neuroendocrine tumors: common questions and tentative answers.". Virchows Arch 458 (4): 393-402. doi:10.1007/s00428-011-1060-7. PMID 21344263.