Parathyroid glands
The parathyroid glands are an endocrine organ that is important in calcium regulation. They often make an appearance in the context of thyroid surgery.
Error creating thumbnail:
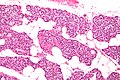
Micrograph of a parathyroid gland. H&E stain.
They produce parathyroid hormone (PTH). PTH acts to increase serum calcium and is important in the regulation of the calcium balance.
Clinical
Hyperparathyroidism
- Definition: increased secretion of parathyroid hormone (PTH).[1]
What PTH does:[1]
- Increase serum calcium.
- Decrease serum phosphate.
Classification
- Primary.
- Secondary.
- Tertiary.
Overview in a table
| Type | PTH | Calcium | Common causes |
|---|---|---|---|
| Primary hyperparathyroidism | high | high | parathyroid adenoma (~85-90% of cases), parathyroid hyperplasia (~10-15% of cases) |
| Secondary hyperparathyroidism | high | low or normal | chronic renal failure, vitamin D deficiency[2] |
| Tertiary hyperparathyroidism | high | high | persistent hyperparathyroidism after renal transplant;[3] arises in the context of secondary hyperparathyroidism[4] |
Genetics
Genes implicated in hyperparathyroidism:[5][6]
- MEN1.
- CASR.
- HRPT2/CDC73.
- CDKN1B.
- RET.
Hypercalcemia DDx
Mnemonic GRIMED:[7]
- Granulomatous disease (tuberculosis, sarcoidosis).
- Renal disease.
- Immobility.
- Malignancy (esp. squamous cell carcinoma, plasmacytoma).
- Endocrine (primary hyperparathyroidism, tertiary hyperparathyroidism, familial hypocalciuric hypercalcemia (FHH)).
- Drugs (thiazides ... others).
Note:
- Hyperparathyroidism and FHH are assoc. with an increased PTH.[8]
- Other causes are assoc. with a decreased PTH.
Primary hyperparathyroidism
Cause:[9]
- Parathyroid adenoma ~90%.
- Parathyroid hyperplasia ~10%.
- Parathyroid carcinoma ~1%.
Familial causes of primary hyperparathyroidism:
- MEN 1.
- MEN 2A.
- Familial hypocalciuric hypercalcemia.
- Autosomal dominant.
- CASR (calcium sensing receptor) gene defect.[10]
Classic manifestations moans, stones, bones, (abdominal) groans, psychiatric overtones.[11][12]
- Moans = bone pain.
- Stones = nephrolithiasis (kidney stones).
- Bones = bone pathology, e.g. osteitis fibrosa cystica.[13]
- Groans = constipation.
- Psychiatric overtones = CNS pathology.
- Can include: lethargy, fatigue, depression, memory loss, psychosis, ataxia, delirium, and coma.
Hypoparathyroidism
- Rare vis-à-vis hyperparathyroidism.
- Classically iatrogenic, i.e. the surgeon removing 'em.[8]
Other causes:[14]
- Autoimmune hypoparathyroidism.
- Autosomal dominat hypoparathyroidism.
- Familial isolated hypoparathyroidism.
- Congenital absence (DiGeorge syndrome).
- Drugs - proton pump inhibitors.[15][16]
Normal parathyroid glands
- The cytology is dealt with in normal parathyroid cytology.
General
- Identification of normal can be tricky.
Gross
- No distinctive features - surgeons thus send 'em to pathologists.
Microscopic
Features:[17]
- Low power:
- May vaguely resemble lymphoid tissue - may have hyperchromatic cytoplasm.
- Does not have follicular centres like a lymph node.
- May form gland-like structure and vaguely resemble the thyroid at low power.
- Cytoplasm may be clear[18] - key feature.
- Surrounded by a thin fibrous capsule.
- May vaguely resemble lymphoid tissue - may have hyperchromatic cytoplasm.
- High power:
- Mixed cell population:[19]
- Chief cells - predominant cell type, small, cytoplasm has variable staining (hyperchromatic-clear-eosinophilic).
- Oxyphil cells (acid staining cells[20]) - abundant cytoplasm.
- Adipocytes - dependent on age, body habitus, PT hormone, size of gland.[21]
- Increased with age, may be used to help differentiate from thyroid - key feature.
- Mixed cell population:[19]
Images
Parathyroid gland - intermed. mag. (WC)
Parathyroid gland - cropped - high mag. (WC)
Parathyroid gland - high mag. (WC)

www:
Parathyroid cell types
| Name | Staining (cytoplasm) | Quantity of cells | Cytoplasm (quantity) | Function | Image |
|---|---|---|---|---|---|
| (parathyroid) chief cells | intense hyperchromatic to eosinophilic (see note) | abundant | moderate | manufacture parathyroid hormone (PTH) |
|
| oxyphil cells | moderate/light hyperchromatic to eosinophilic | rare | abundant | ? | File:Parathyroid adenoma - oxyphil cells -- high mag.jpg Oxyphil cells (WC) |

{kind=link}
Notes:
- Cytoplasmic staining varies considerably on H&E preparations - it may vary from hyperchromatic[22] to clear to eosinophilic.[23]
- Chief cells tend to stain more intensely than oxyphil cells.
Thyroid versus parathyroid
- Parathyroid cytoplasm:
- Hyperchromatic.
Notes:
- Thyroid often has birefringent (calcium oxalate) crystals (60 of 80 cases) whereas parathyroid less often does (2 or 20 cases).[24]
- Thyroid usually follicular - though parathyroid occasionally is pseudofollicular.
Parathyroid versus lymphoid tissue
- Parathyroid:
- No germinal centres.
- Gland-like/follicular-like arrangement may be present but usually much smaller than normal thyroid follicles.
- May be confused with thyroid microfollicules.
- Occasional cell with rim of clear cytoplasm (oxyphil?).
- Nuclei are different:
- Slightly larger than in lymphocytes (1.2-1.5x the size)
- Stippled chromatin (unlike lymphocytes).
Images:
{kind=link}
IHC
- GATA3 +ve (>98%[26]).
- PTH -ve/+ve (~33%[26]).
- Chromogranin A +ve (~80%[26]).
- AE1/AE3 +ve.[citation needed]
Specific entities
Parathyroid hyperplasia
Main article: Parathyroid hyperplasia
Parathyroid adenoma
Main article: Parathyroid adenoma
Parathyroid carcinoma
Main article: Parathyroid carcinoma
See also
References
- ↑ 1.0 1.1 URL: http://emedicine.medscape.com/article/127351-overview. Accessed on: 24 January 2013.
- ↑ URL: http://emedicine.medscape.com/article/127351-overview#aw2aab6b5. Accessed on: 24 January 2013.
- ↑ URL: http://emedicine.medscape.com/article/127351-overview#aw2aab6b6. Accessed on: 24 January 2013.
- ↑ Duan, K.; Gomez Hernandez, K.; Mete, O. (Oct 2015). "Clinicopathological correlates of hyperparathyroidism.". J Clin Pathol 68 (10): 771-87. doi:10.1136/jclinpath-2015-203186. PMID 26163537.
- ↑ Starker, LF.; Akerström, T.; Long, WD.; Delgado-Verdugo, A.; Donovan, P.; Udelsman, R.; Lifton, RP.; Carling, T. (Apr 2012). "Frequent germ-line mutations of the MEN1, CASR, and HRPT2/CDC73 genes in young patients with clinically non-familial primary hyperparathyroidism.". Horm Cancer 3 (1-2): 44-51. doi:10.1007/s12672-011-0100-8. PMID 22187299.
- ↑ Hendy, GN.; Cole, DE. (2013). "Genetic defects associated with familial and sporadic hyperparathyroidism.". Front Horm Res 41: 149-65. doi:10.1159/000345675. PMID 23652676.
- ↑ Shiau, Carolyn; Toren, Andrew (2006). Toronto Notes 2006: Comprehensive Medical Reference (Review for MCCQE 1 and USMLE Step 2) (22nd edition (2006) ed.). Toronto Notes for Medical Students, Inc.. pp. Emerg.. ISBN 978-0968592861.
- ↑ 8.0 8.1 Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1129. ISBN 978-1416031215.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1127. ISBN 978-1416031215.
- ↑ Online 'Mendelian Inheritance in Man' (OMIM) 601199
- ↑ Lienert, D.; Rege, S. (Feb 2008). "Moans, stones, groans, bones and psychiatric overtones: lithium-induced hyperparathyroidism.". Aust N Z J Psychiatry 42 (2): 171-3. PMID 18350681.
- ↑ URL: http://www.usmleforum.com/files/forum/2010/1/505388.php. Accessed on: 4 December 2011.
- ↑ França, TC.; Griz, L.; Pinho, J.; Diniz, ET.; Andrade, LD.; Lucena, CS.; Beserra, SR.; Asano, NM. et al. (Apr 2011). "Bisphosphonates can reduce bone hunger after parathyroidectomy in patients with primary hyperparathyroidism and osteitis fibrosa cystica.". Rev Bras Reumatol 51 (2): 131-7. PMID 21584419.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1130. ISBN 978-1416031215.
- ↑ Deroux, A.; Khouri, C.; Chabre, O.; Bouillet, L.; Casez, O. (Oct 2014). "Severe acute neurological symptoms related to proton pump inhibitors induced hypomagnesemia responsible for profound hypoparathyroidism with hypocalcemia.". Clin Res Hepatol Gastroenterol 38 (5): e103-5. doi:10.1016/j.clinre.2014.03.005. PMID 24736034.
- ↑ Toh, JW.; Ong, E.; Wilson, R. (Aug 2014). "Hypomagnesaemia associated with long-term use of proton pump inhibitors.". Gastroenterol Rep (Oxf). doi:10.1093/gastro/gou054. PMID 25138239.
- ↑ http://www.medicalhistology.us/twiki/pub/Main/ChapterFourteenSlides/b56b_parathyroid_40x_he_labeled.jpg
- ↑ http://pathology.mc.duke.edu/research/Histo_course/parathyroid2.jpg
- ↑ http://www.bu.edu/histology/p/15002loa.htm
- ↑ http://dictionary.reference.com/search?q=oxyphil%20cell
- ↑ Iwasaki, A.; Shan, L.; Kawano, I.; Nakamura, M.; Utsuno, H.; Kobayashi, A.; Kuma, K.; Kakudo, K. (Jul 1995). "Quantitative analysis of stromal fat content of human parathyroid glands associated with thyroid diseases using computer image analysis.". Pathol Int 45 (7): 483-6. PMID 7551007.
- ↑ http://www.deltagen.com/target/histologyatlas/atlas_files/endocrine/parathyroid_and_thyroid_glands_20x.jpg
- ↑ http://instruction.cvhs.okstate.edu/Histology/HistologyReference/hrendo.htm
- ↑ Wong KS, Lewis JS, Gottipati S, Chernock RD (September 2014). "Utility of birefringent crystal identification by polarized light microscopy in distinguishing thyroid from parathyroid tissue on intraoperative frozen sections". Am J Surg Pathol 38 (9): 1212–9. doi:10.1097/PAS.0000000000000204. PMID 24618617.
- ↑ Johnson, SJ.; Sheffield, EA.; McNicol, AM. (Apr 2005). "Best practice no 183. Examination of parathyroid gland specimens.". J Clin Pathol 58 (4): 338-42. doi:10.1136/jcp.2002.002550. PMC 1770637. PMID 15790694. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1770637/.
- ↑ 26.0 26.1 26.2 Takada, N.; Hirokawa, M.; Suzuki, A.; Higuchi, M.; Kuma, S.; Miyauchi, A. (Jul 2016). "Diagnostic value of GATA-3 in cytological identification of parathyroid tissues.". Endocr J 63 (7): 621-6. doi:10.1507/endocrj.EJ15-0700. PMID 27097544.
{kind=link}
{kind=link}