Pneumonia
Pneumonia is inflammation of the lung, which includes infectious and non-infectious etiologies.
It is a subset of the medical lung diseases. This article primarily deals with the infectious pneumonias. Idiopathic interstitial pneumonias are discussed very briefly; they are dealt with in detail in the diffuse lung diseases article.
Infectious pnemonia
Anatomical classification of pneumonia
- Generally, not used by clinicians.
- Use of the terms without qualification is discouraged... as they do not make explicit the etiology.
Bronchopneumonia
- Multiple foci of (acute) inflammation involving the bronchi.
- This is the most common form of (infectious) pneumonia.
Lobar pneumonia
- Pneumonia that involves a whole lobe.
- Rarely seen in areas where antibiotic treatments are widely available.
Acute infectious pneumonia
General
- This is seen by pathologists, in autopsy, from time-to-time.
Most common cause:
- Streptococcus pneumoniae.[1]
The top three community acquired (acute) pneumonia:[2]
- Streptococcuc pneumonia.
- Haemophilus influenzae.
- Moraxella catarrhalis.
Other community acquired pneumonia:[1]
- S. aureus.
- Legionaella pneumophila.
- Klebsiella pneumoniae.
- Pseudomonas.
Hospital-acquired pneumonia:[1]
- Gram-negative rods.
- Staphylococcus aureus.
Radiologic correlate
- Air space disease.
Gross pathology
- Consolidation (the lung parenchyma is firm) - best appreciated by running a finger over the cut surface of the lung with a small-to-moderate amount of pressure.
Bronchopneumonia:
- Classically yellow-white centered on the bronchi.[3]
Lobar pneumnia is classically described in four stages:[4][5]
- Congestion - day 1-2.
- Red hepatization - day 2-4.
- Gray hepatization - day 4-6.
- Resolution - day 6+.
Note:
- The stages of lobar pneumonia is considered more-or-less historical. In the age of antibiotics, lobar pneumonia is uncommon.
Microscopic
Features:
- Alveoli packed with PMNs.
- +/-Clusters of bacteria - small dots or rods.
- +/-Abscess formation.
- Lung abscess = destruction of parenchyma + PMNs.[6]
Image:
{kind=link}
Stains
- Gram stain -- to type the bacteria.
Chronic infectious pneumonia
General
Common microorganisms:[1]
- Nocardia.
- Actinomyces.
- Mycobacterium tuberculosis.
- Atypical mycobacterium, e.g. Mycobacterium avium-intracellulare.
- Histoplasma capsulatum.
- Coccidioides immitis.
- Blastomyces dermatitidis.
Note:
- All of the later ones are granulomatous.
Microscopic
Features:
- Inflammation.
- +/-Granulomas.
Aspiration pneumonia
General
- Usually seen in the context of a toxin and/or pathology that affects the swallowing and cough reflexes.[7]
- The microorganisms involved are usually different than in other causes of acute pneumonia.
Note:
- A special type of aspiration pneumonia is lipoid pneumonia. It is dealt with in the lipoid pneumonia article.
Gross
- More common in the right lung.
- Right main stem bronchus is more vertical.
Microscopic
Features:
- +/-Foreign body giant cells.
- Microorganisms.
Images:
{kind=link}
{kind=link}
{kind=link}
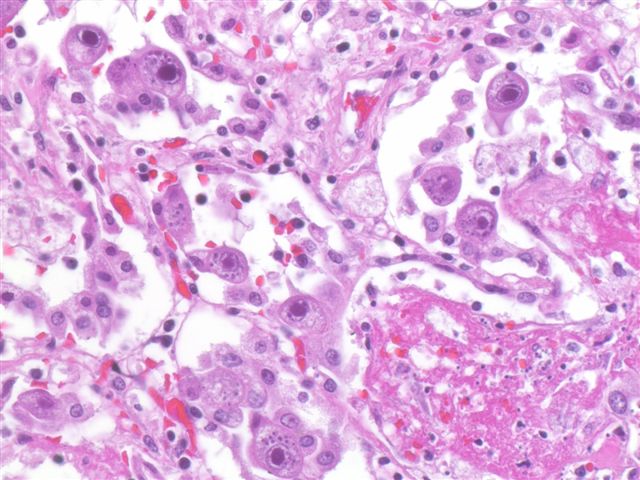
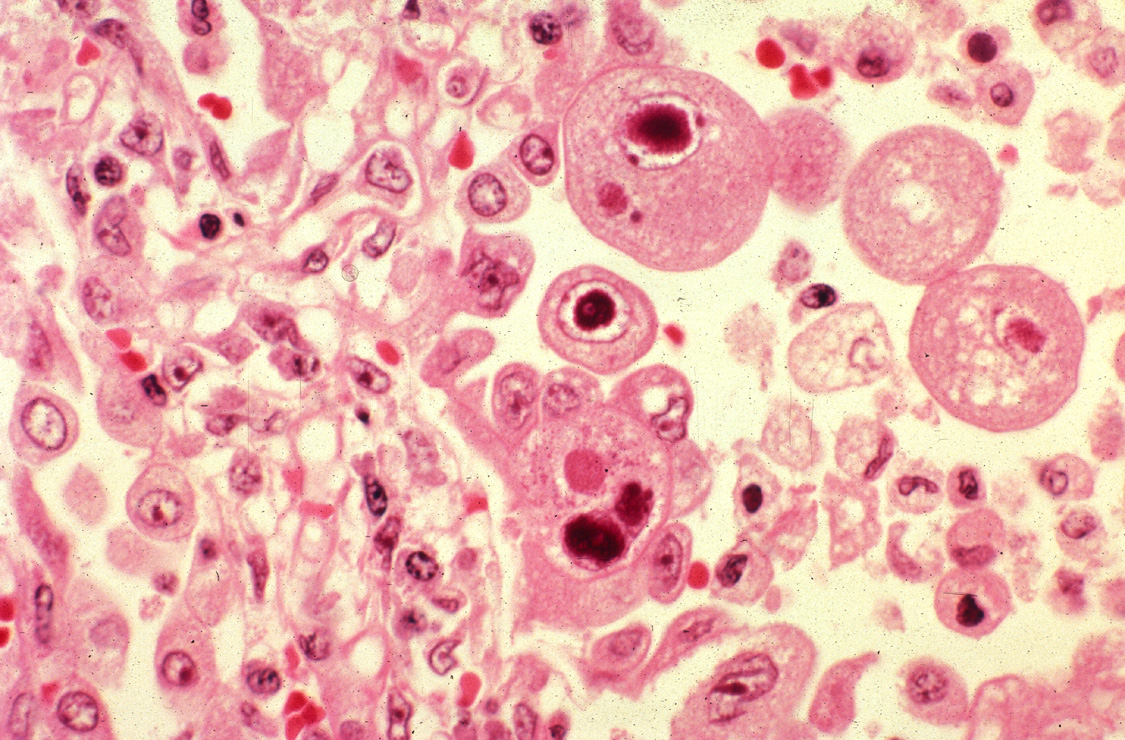
Cytomegalovirus pneumonia
Main article: Cytomegalovirus
General
- Immunodeficiency.
- Critical illness.[8]
Microscopic
Features:
- CMV nuclear changes:
- Large red nucleus with a pale halo.
- Eosinophilic granular cytoplasmic inclusions.
Images:
{kind=link}
{kind=link}
IHC
- CMV +ve -- cytoplasmic inclusions, large nucleus.
Diffuse lung diseases
Main article: Diffuse lung disease
- AKA idiopathic interstitial pneumonia.
Histologic pattern:
See also
References
- ↑ 1.0 1.1 1.2 1.3 Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 711. ISBN 978-1416031215.
- ↑ Nicolau, D. (Sep 2002). "Clinical and economic implications of antimicrobial resistance for the management of community-acquired respiratory tract infections.". J Antimicrob Chemother 50 Suppl S1: 61-70. PMID 12239229.
- ↑ Rose, Alan G. (2008). Atlas of Gross Pathology with Histologic Correlation (1st ed.). Cambridge University Press. pp. 93. ISBN 978-0521868792.
- ↑ Rose, Alan G. (2008). Atlas of Gross Pathology with Histologic Correlation (1st ed.). Cambridge University Press. pp. 92. ISBN 978-0521868792.
- ↑ URL: http://www.histopathology-india.net/Lobar_Pneumonia.htm. Accessed on: 27 February 2012.
- ↑ Rose, Alan G. (2008). Atlas of Gross Pathology with Histologic Correlation (1st ed.). Cambridge University Press. pp. 95. ISBN 978-0521868792.
- ↑ Ohrui, T. (Sep 2005). "Preventive strategies for aspiration pneumonia in elderly disabled persons.". Tohoku J Exp Med 207 (1): 3-12. PMID 16082150.
- ↑ Limaye, AP.; Boeckh, M. (Nov 2010). "CMV in critically ill patients: pathogen or bystander?". Rev Med Virol 20 (6): 372-9. doi:10.1002/rmv.664. PMID 20931610.
- ↑ URL: http://www.pathologyoutlines.com/topic/lungnontumorCMV.html. Accessed on: 23 January 2012.