Schwannoma
Schwannoma is a relatively common peripheral nerve sheath tumour.
| Schwannoma | |
|---|---|
| Diagnosis in short | |
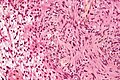
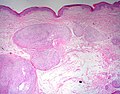
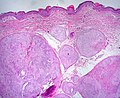
 Schwannoma showing Antoni A and Antoni B areas. HPS stain. | |
|
| |
| LM |
Antoni A areas (cellular, fibrillary, polar, elongated), Antoni B area (pauci-cellular, loose microcystic tissue), Verocay bodies (paucinuclear area surrounded by nuclei), hyaline thickened blood vessels, thick capsule. +/-peripheral lymphoid cuff (esp. GI tract) |
| Subtypes | conventional schwannoma, cellular schwannoma, plexiform schwannoma, melanotic schwannoma |
| LM DDx | meningioma, leiomyoma, GIST, intranodal palisaded myofibroblastoma, MPNST, neurofibroma, biphenotypic sinonasal sarcoma |
| IHC | S-100 +ve, EMA -ve, CD34 +ve |
| Site | soft tissue - peripheral nerve sheath tumours |
|
| |
| Syndromes | neurofibromatosis type 2, Carney complex (psammomatous melanotic schwannoma), schwannomatosis |
|
| |
| Prevalence | common |
| Prognosis | good |
| Clin. DDx | meningioma - esp. at cerebellopontine angle |
At the cerebellopontine (CP) angle, they may be referred to as acoustic neuroma or vestibular schwannoma.
General
- A common neuropathology tumour that occasionally shows-up elsewhere.
- often encapsulated tumour of tissue surrounding a nerve.
- Axons adjacent to the tumour are normal... but may be compressed.
- May be a part of neurofibromatosis type 2.
- Occurs at all ages.
Macro
- Usu. encapsulated.
- Cystic.
- Yellow patches on white surface.
- Variable lipidization.
Microscopic
Features:[1]
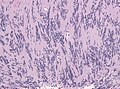
- Antoni A:
- Cellular.
- 'Fibrillary, polar, elongated'.
- Antoni B:
- Pauci-cellular.
- Loose microcystic tissue.
- Verocay bodies - paucinuclear area surrounded by clusters of nuclei - diagnostic feature.
- Hyaline thickened blood vessels.
- Thick capsule.
- In the GI tract: classically have a peripheral lymphoid cuff.[2]
- +/-Hemosiderin deposition within tumour.
- Reticulin stain +ve (around individual cells).
Notes:
- Tumour does not smear well.[3]
- Antoni A: may look somewhat like scattered matchsticks.
- Hybrid Schwannoma / Neurofibroma are overrepresented in hereditary conditions.[4]
DDx:
- Meningioma.
- Intranodal palisaded myofibroblastoma - if surrounded by a rim of lymphoid tissue, i.e. intranodal.
- Leiomyoma.
- Gastrointestinal stromal tumour.
- MPNST - schwannoma with ancient change has no significant mitotic activity.[5]
- Neurofibroma.
- Biphenotypic sinonasal sarcoma - head and neck.
Images

Schwannoma - Antoni A & B - intermed. mag. (WC)
Schwannoma - Antoni A & B - very high mag. (WC)
Antoni-A pattern in cerebelloponine angle schwannoma. (WC/jensflorian)
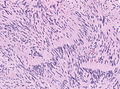
Antoni-A pattern in cerebelloponine angle schwannoma.(WC/jensflorian)
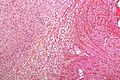
Nerve root schwannoma - intermed. mag. (WC)

S-100 immunostain in schwannoma. (WC/Ed Uthman)




.jpg)
www:
- Antoni A (pathguy.com).
- Antoni A & Antoni B side-by-side (ajnr.org).
- Cystic schwannoma - several images (upmc.edu).
Schwannoma subtypes
There are four:[6]
- Conventional schwannoma.
- Cellular schwannoma.
- Plexiform schwannoma.
- Melanotic schwannoma.
Conventional schwannoma
- Most common.
Cellular schwannoma
- May mimic MPNST.
- Usu. <4 mitoses in 10 HPF (see HPFitis).
- Absence of Verocay bodies.
- Usu paravertebral location.
Images:
Plexiform schwannoma
- May mimic MPNST if cellular - esp. in childhood.
Images:
Plexiform schwannoma - low mag. (WC)
Plexiform schwannoma - high mag. (WC)


Melanotic schwannoma
- May be confused with melanoma.
- Psammomatous form (psammomatous melanotic schwannoma) associated with a heritable disorder (Carney complex).
Note:
- Carney complex:[6]
- Cutaneous lentigines.
- Myxomas (skin (subcutaneous), subcutanous, heart).
- Endocrine neoplasms.
Images:
Psammomatous melanotic schwannoma - high mag. (WC)

IHC
Features:[7]
- S-100 +ve.
- Glut1 +ve.
- CD34 +ve.
- Cytokeratins ~70% +ve.[8]
- SOX10 +ve.[9]
- -ve in synovial sarcoma, rhabdomyosarcoma, chondrosarcoma.
- EMA -ve. (???)
- Usually +ve (~75% of the time) in meningiomas.[10]
Others:
Molecular
Overview: [13]
- Most common: NF2 (in Vestibular Schwannoma up to84%).
- less common: ARID1A, ARID1B, DDR, TSC1, TSC2, CDC27 and USP8.
- SH3PXD2A-HTRA1 fusions (10%).
Molecular subgroups:[16]
- Group 1: vestibular (has significant higher rate of 22q loss).
- Group 2: spinal.
Sign out
Lesion, Right Ulnar Nerve, Excision:
- Schwannoma.
Block letters
LESION, LEFT ANTERIOR TIBIA, EXCISION: - SCHWANNOMA. - NEGATIVE FOR MALIGNANCY.
Micro
The sections show a soft tissue spindle cell lesion, with cellular fibrillary areas (Antoni A) and pauci-cellular microcystic areas (Antoni B). There are also pauci-nuclear areas surrounded by clusters of nuclei (Verocay bodies). Thick hyaline blood vessels are present within the lesion. There is no apparent nuclear atypia. Mitotic activity is not readily apparent. No nerve is seen adjacent to the lesion. The lesion is partially encapsulated by fibrous tissue. Focally, ink is seen on the lesional cells.
See also
References
- ↑ Wippold FJ, Lubner M, Perrin RJ, Lämmle M, Perry A (October 2007). "Neuropathology for the neuroradiologist: Antoni A and Antoni B tissue patterns". AJNR Am J Neuroradiol 28 (9): 1633–8. doi:10.3174/ajnr.A0682. PMID 17893219. http://www.ajnr.org/cgi/reprint/28/9/1633.
- ↑ Levy AD, Quiles AM, Miettinen M, Sobin LH (March 2005). "Gastrointestinal schwannomas: CT features with clinicopathologic correlation". AJR Am J Roentgenol 184 (3): 797–802. PMID 15728600. http://www.ajronline.org/cgi/content/full/184/3/797.
- ↑ MUN. 24 November 2010.
- ↑ Harder, A.; Wesemann, M.; Hagel, C.; Schittenhelm, J.; Fischer, S.; Tatagiba, M.; Nagel, C.; Jeibmann, A. et al. (May 2012). "Hybrid neurofibroma/schwannoma is overrepresented among schwannomatosis and neurofibromatosis patients.". Am J Surg Pathol 36 (5): 702-9. doi:10.1097/PAS.0b013e31824d3155. PMID 22446939.
- ↑ Chan, PT.; Tripathi, S.; Low, SE.; Robinson, LQ. (2007). "Case report--ancient schwannoma of the scrotum.". BMC Urol 7: 1. doi:10.1186/1471-2490-7-1. PMID 17244372.
- ↑ 6.0 6.1 Kurtkaya-Yapicier O, Scheithauer B, Woodruff JM (July 2003). "The pathobiologic spectrum of Schwannomas". Histol. Histopathol. 18 (3): 925–34. PMID 12792904.
- ↑ Hirose T, Tani T, Shimada T, Ishizawa K, Shimada S, Sano T (April 2003). "Immunohistochemical demonstration of EMA/Glut1-positive perineurial cells and CD34-positive fibroblastic cells in peripheral nerve sheath tumors". Mod. Pathol. 16 (4): 293–8. doi:10.1097/01.MP.0000062654.83617.B7. PMID 12692193. http://www.nature.com/modpathol/journal/v16/n4/full/3880761a.html.
- ↑ Fanburg-Smith, JC.; Majidi, M.; Miettinen, M. (Jan 2006). "Keratin expression in schwannoma; a study of 115 retroperitoneal and 22 peripheral schwannomas.". Mod Pathol 19 (1): 115-21. doi:10.1038/modpathol.3800489. PMID 16357842.
- ↑ Nonaka D, Chiriboga L, Rubin BP (September 2008). "Sox10: a pan-schwannian and melanocytic marker". Am. J. Surg. Pathol. 32 (9): 1291–8. doi:10.1097/PAS.0b013e3181658c14. PMID 18636017.
- ↑ Rushing, EJ.; Bouffard, JP.; McCall, S.; Olsen, C.; Mena, H.; Sandberg, GD.; Thompson, LD. (Jun 2009). "Primary extracranial meningiomas: an analysis of 146 cases.". Head Neck Pathol 3 (2): 116-30. doi:10.1007/s12105-009-0118-1. PMID 19644540.
- ↑ Hasegawa, M.; Muramatsu, N.; Tohma, Y.; Fukaya, K.; Fujisawa, H.; Hayashi, Y.; Tachibana, O.; Kida, S. et al. (Jan 2002). "Expression of E-cadherin-catenin complex in human benign schwannomas.". Histol Histopathol 17 (1): 39-44. PMID 11813884.
- ↑ Carlson, JW.; Fletcher, CD. (Oct 2007). "Immunohistochemistry for beta-catenin in the differential diagnosis of spindle cell lesions: analysis of a series and review of the literature.". Histopathology 51 (4): 509-14. doi:10.1111/j.1365-2559.2007.02794.x. PMID 17711447.
- ↑ Agnihotri, S.; Jalali, S.; Wilson, MR.; Danesh, A.; Li, M.; Klironomos, G.; Krieger, JR.; Mansouri, A. et al. (11 2016). "The genomic landscape of schwannoma.". Nat Genet 48 (11): 1339-1348. doi:10.1038/ng.3688. PMID 27723760.
- ↑ Caltabiano, R.; Magro, G.; Polizzi, A.; Praticò, AD.; Ortensi, A.; D'Orazi, V.; Panunzi, A.; Milone, P. et al. (Jun 2017). "A mosaic pattern of INI1/SMARCB1 protein expression distinguishes Schwannomatosis and NF2-associated peripheral schwannomas from solitary peripheral schwannomas and NF2-associated vestibular schwannomas.". Childs Nerv Syst 33 (6): 933-940. doi:10.1007/s00381-017-3340-2. PMID 28365909.
- ↑ Evans, DG.; Bowers, NL.; Tobi, S.; Hartley, C.; Wallace, AJ.; King, AT.; Lloyd, SKW.; Rutherford, SA. et al. (Jun 2018). "Schwannomatosis: a genetic and epidemiological study.". J Neurol Neurosurg Psychiatry. doi:10.1136/jnnp-2018-318538. PMID 29909380.
- ↑ Agnihotri, S.; Jalali, S.; Wilson, MR.; Danesh, A.; Li, M.; Klironomos, G.; Krieger, JR.; Mansouri, A. et al. (11 2016). "The genomic landscape of schwannoma.". Nat Genet 48 (11): 1339-1348. doi:10.1038/ng.3688. PMID 27723760.