Sjögren syndrome
Sjögren syndrome, also Sjögren disease, is an uncommon disease that rheumatologists see. Sjögren is also spelled Sjoegren and Sjogren.
The syndrome may be part of another connective tissue disorder, e.g. rheumatoid arthritis, in which case it is called secondary Sjögren syndrome.[1]
General
Clinical - classically:
- Women in 50s.
- Dry mouth (xerostomia).
- Dry eyes (xerophthalmia).
Diagnostic criteria
European criteria of 2002:[2]
| Criteria | Details | Type |
|---|---|---|
| Oral symptoms | any: (1) dry mouth > 3 months, (2) require fluids for swallowing, (3) swollen salivary glands (adults) | history |
| Oral signs | any: (1) low salivary flow test positive, (2) salivary scintigraphy positive (3) (parotid) sialography positive | clinical test |
| Ocular symptoms | any: (1) dry eye > 3 months, (2) need artifical tears >3x/day, (3) sand or gravel in the eyes sensation | history |
| Ocular signs | any: (1) Schirmer's test positive, (2) ocular dye test positive | clinical test |
| Autoantibodies | anti-SSA/Ro and/or anti-SSB/La | serology |
| Histology | labial minor salivary gland biopsy focus score >= 1.0/ 4 mm*mm; definition: multiple lymphocytic foci with >50 lymphocytes adjacent to mucinous acini, evaluated in 4 mm*mm of glandular tissue | pathology |
The diagnosis is made if either:[2]
- Four of six criteria required, must include either autoantibodies or histology.
- Three of the four objective (non-history) criteria are met.
Notes:
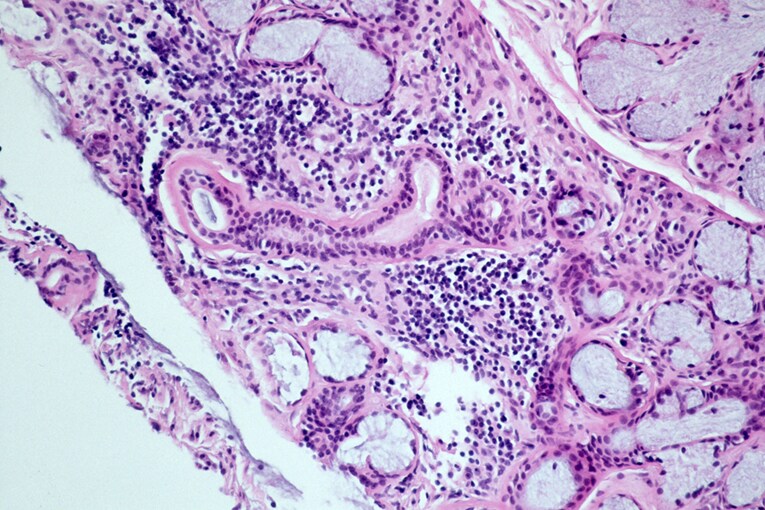
Microscopic
Features (salivary gland):[3]
- "Significant lymphocytic infiltrate" adjacent to viable salivary gland (or lacrimal gland) acini - key feature.
- "Significant" lymphocytic infiltrate": cluster of >= 50 lymphocytes - important.
- Lymphocytes may be perivascular or periductular.[4][5]
- Plasma cells should not exceed 10% of the inflammatory infiltrate.[4]
- May have "benign lymphoepithelial lesions"[6] - intraepithelial lymphocytes.
- "Significant" lymphocytic infiltrate": cluster of >= 50 lymphocytes - important.
- +/-Fibrosis.
DDx:
- MALT lymphoma.
- Chronic sialadenitis - mixed inflammatory infiltrate.
Note:
- Diagnosis is based on clinicopathologic correlation; the histology alone is insufficient.
Images:
Focus score
Features:[4]
- This is nothing more than a count of significant lymphocytic foci per 4 mm*mm.
- Significant: >= 50 lymphocytes, adjacent to salivary gland acini.
- A focus score of one or more is considered significant.[2]
Calculating the focus score (fs):
- Count the significant foci (n).
- Estimate that area in mm2 (a).

{kind=link}
{kind=link}
{kind=link}
Grading
In the past lesions were graded with the Chisholm-Mason classification.[6][8] The Chisholm-Mason classification is based on assessing 4 mm2 area of salivary gland tissue and depends on the abundance and aggregation of lymphocytes.
It is compares to Daniels-Whitcher grading as follows:
| Lymphocytes | Daniels-Whitcher grade |
Chisholm-Mason grade |
|---|---|---|
| slight infiltrate | mild | 1 |
| moderate infiltrate or less than one focus † | intermediate | 2 |
| one focus † | severe | 3 |
| more than one focus † | severe | 4 |
† Focus = an aggregrate of 50 lymphocytes or more.
Sign out
LOWER LIP, BIOPSY: - MINOR SALIVARY GLAND WITH FOCAL LYMPHOCYTIC SIALADENITIS, SEE COMMENT. - SQUAMOUS MUCOSA WITH PARAKERATOSIS, MILD. - NO SIGNIFICANT FIBROSIS. COMMENT: Glandular area: 8 mm*mm. Interstitial fat: not apparent. Plasma cells: not apparent. Fibrosis: none apparent (0% of salivary gland area). Ductular dilation: not apparent. Gross foci: 4. Focus score (foci/4 mm*mm): 2. The histologic findings are compatible with those seen in Sjoegren's disease (focus score >= 1). This result needs to be combined with the clinical and serologic criteria used to diagnose Sjoegren's disease.
See also
References
- ↑ Celenligil, H.; Kansu, E.; Ruacan, S.; Eratalay, K.; Irkeç, M. (1990). "Characterization of peripheral blood and salivary gland lymphocytes in secondary Sjögren's syndrome.". Ann Dent 49 (2): 18-22. PMID 1703737.
- ↑ 2.0 2.1 2.2 Vitali, C.; Bombardieri, S.; Jonsson, R.; Moutsopoulos, HM.; Alexander, EL.; Carsons, SE.; Daniels, TE.; Fox, PC. et al. (Jun 2002). "Classification criteria for Sjögren's syndrome: a revised version of the European criteria proposed by the American-European Consensus Group.". Ann Rheum Dis 61 (6): 554-8. PMC 1754137. PMID 12006334. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1754137/.
- ↑ 3.0 3.1 "Information from your family doctor. Sjögren syndrome.". Am Fam Physician 79 (6): 472. Mar 2009. PMID 19323360.
- ↑ 4.0 4.1 4.2 4.3 Vivino, FB.; Gala, I.; Hermann, GA. (May 2002). "Change in final diagnosis on second evaluation of labial minor salivary gland biopsies.". J Rheumatol 29 (5): 938-44. PMID 12022353.
- ↑ Daniels, TE.; Whitcher, JP. (Jun 1994). "Association of patterns of labial salivary gland inflammation with keratoconjunctivitis sicca. Analysis of 618 patients with suspected Sjögren's syndrome.". Arthritis Rheum 37 (6): 869-77. PMID 8003059.
- ↑ 6.0 6.1 Ramos-Casals, M.; Font, J. (Nov 2005). "Primary Sjögren's syndrome: current and emergent aetiopathogenic concepts.". Rheumatology (Oxford) 44 (11): 1354-67. doi:10.1093/rheumatology/keh714. PMID 15956090. http://rheumatology.oxfordjournals.org/content/44/11/1354.long.
- ↑ URL: http://emedicine.medscape.com/article/332125-workup#aw2aab6b5b6aa. Accessed on: 24 July 2012.
- ↑ Chisholm, DM.; Mason, DK. (Sep 1968). "Labial salivary gland biopsy in Sjögren's disease.". J Clin Pathol 21 (5): 656-60. PMC 473887. PMID 5697370. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC473887/?tool=pubmed.