Difference between revisions of "Pulmonary alveolar proteinosis"
Jump to navigation
Jump to search
(→Stains) |
(→Stains) |
||
| Line 87: | Line 87: | ||
==Stains== | ==Stains== | ||
*[[PAS stain|PAS]] +ve -- material in airspace (surfactant).<ref name=pmid24424195>{{Cite journal | last1 = Ben-Dov | first1 = I. | last2 = Segel | first2 = MJ. | title = Autoimmune pulmonary alveolar proteinosis: Clinical course and diagnostic criteria. | journal = Autoimmun Rev | volume = | issue = | pages = | month = Jan | year = 2014 | doi = 10.1016/j.autrev.2014.01.046 | PMID = 24424195 }}</ref> | *[[PAS stain|PAS]] +ve -- material in airspace (surfactant).<ref name=pmid24424195>{{Cite journal | last1 = Ben-Dov | first1 = I. | last2 = Segel | first2 = MJ. | title = Autoimmune pulmonary alveolar proteinosis: Clinical course and diagnostic criteria. | journal = Autoimmun Rev | volume = | issue = | pages = | month = Jan | year = 2014 | doi = 10.1016/j.autrev.2014.01.046 | PMID = 24424195 }}</ref><ref>{{Cite journal | last1 = Mikami | first1 = T. | last2 = Yamamoto | first2 = Y. | last3 = Yokoyama | first3 = M. | last4 = Okayasu | first4 = I. | title = Pulmonary alveolar proteinosis: diagnosis using routinely processed smears of bronchoalveolar lavage fluid. | journal = J Clin Pathol | volume = 50 | issue = 12 | pages = 981-4 | month = Dec | year = 1997 | doi = | PMID = 9516877 }}</ref> | ||
*[[PASD stain|PASD]] +ve (red<ref name=pmid16468308>{{Cite journal | last1 = Meng | first1 = ZL. | last2 = Liu | first2 = HR. | last3 = Liang | first3 = ZY. | last4 = Zhang | first4 = SY. | title = [Pathologic feature and diagnosis of pulmonary alveolar proteinosis]. | journal = Zhonghua Bing Li Xue Za Zhi | volume = 34 | issue = 9 | pages = 575-8 | month = Sep | year = 2005 | doi = | PMID = 16468308 }}</ref>). | *[[PASD stain|PASD]] +ve (red<ref name=pmid16468308>{{Cite journal | last1 = Meng | first1 = ZL. | last2 = Liu | first2 = HR. | last3 = Liang | first3 = ZY. | last4 = Zhang | first4 = SY. | title = [Pathologic feature and diagnosis of pulmonary alveolar proteinosis]. | journal = Zhonghua Bing Li Xue Za Zhi | volume = 34 | issue = 9 | pages = 575-8 | month = Sep | year = 2005 | doi = | PMID = 16468308 }}</ref>). | ||
**[[Pulmonary edema]] fluid -ve.<ref>URL: [http://pathhsw5m54.ucsf.edu/overview/fungi1a.html http://pathhsw5m54.ucsf.edu/overview/fungi1a.html]. Accessed on: 3 March 2014.</ref> | **[[Pulmonary edema]] fluid -ve.<ref>URL: [http://pathhsw5m54.ucsf.edu/overview/fungi1a.html http://pathhsw5m54.ucsf.edu/overview/fungi1a.html]. Accessed on: 3 March 2014.</ref> | ||
Revision as of 14:35, 3 March 2014
| Pulmonary alveolar proteinosis | |
|---|---|
| Diagnosis in short | |
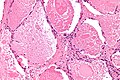
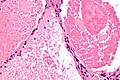
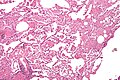
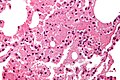
 Pulmonary alveolar proteinosis. H&E stain. | |
|
| |
| LM | "dense bodies" or "chatter" (represent dead macrophages) within acellular eosinophilic material that is in the alveoli |
| LM DDx | pulmonary edema, pneumocystis pneumonia, pulmonary hemorrhage (acute) |
| Stains | PAS +ve |
| IHC | surfactant +ve |
| EM | lamellar bodies |
| Site | lung - see medical lung diseases |
|
| |
| Associated Dx | +/-hematologic malignancy |
| Clinical history | +/-infection, +/-smoking |
| Signs | decreased oxygen saturation |
| Prevalence | uncommon |
| Blood work | anti-GM-CSF antibodies, LDH elevated |
| Radiology | airspace disease, "crazy paving" |
| Prognosis | benign |
Pulmonary alveolar proteinosis, abbreviated PAP, in an uncommon medical lung disease.
General
- Associated with smoking - particularily in men.[1]
Pathophysiology:
- GM-CSF (granulocyte-macrophage colony stimulating factor) signaling in macrophages/lack of GM-CSF.
- GM-CSF is required by alveolar macrophages to clear surfactant.
Classification:[1]
- Congenital:
- Abnormal surfactant.
- GM-CSF receptor defect.
- Secondary:
- Infections.
- Haematologic malignancy.
- Acquired:
- Dusts - interfere with macrophage function.
Clinical:
- Dyspnea & cough - gradual onset.
- Anti-GM-CSF antibodies - usually.[2]
- Serum LDH elevated.[2][3]
- Decreased oxygen saturation.
Radiology
- CXR: airspace disease.
- HRCT: "crazy paving" - see: http://radiographics.rsnajnls.org/cgi/content/figsonly/23/6/1509.
Microscopic
Features:
- Crap in the alveoli:
- "Dense bodies" - dead macrophages ("Chatter" in the alveoli).
- Edema - has pink stuff in the alveoli like PAP but no dense bodies.
DDx - may mimic:[4]
- Pulmonary edema.
- Pneumocystis pneumonia - exudates foamy & vacuolated.
- Pulmonary hemorrhage (acute). (???)
Images
www:
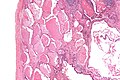
PAP - low mag. (WC)

PAP - intermed. mag. (WC)
PAP - high mag. (WC)
PAP - very high mag. (WC)



PAP - intermed. mag. (WC)
PAP - very high mag. (WC)


{kind=link}
Images of DDx:
Stains
- PAS +ve -- material in airspace (surfactant).[6][7]
- PASD +ve (red[8]).
- Pulmonary edema fluid -ve.[9]
IHC
- Surfactant +ve.[10]
EM
- Lamellar bodies.[11]
Note:
- Lamellar bodies are also seen in secreting adenocarcinoma, obstructive pneumonitis.
Sign out
LUNG, RIGHT UPPER LOBE (ABNORMAL AREA ON CT), WEDGE RESECTION: - PULMONARY ALVEOLAR PROTEINOSIS, SEE COMMENT. - NO SIGNIFICANT INTERSTITIAL FIBROSIS. - NO SIGNIFICANT INFLAMMATION. - NEGATIVE FOR MALIGNANCY.
Micro
Sections show lung with eosinophilic material in the airspaces. Focally, small (~20 micrometres), more dense appearing, bodies are also in the airspace. The alveolar walls are within normal limits. No significant inflammation is identified. No microorganisms are seen with routine stains. There is no pulmonary hemorrhage.
See also
References
- ↑ 1.0 1.1 Trapnell BC, Whitsett JA, Nakata K (December 2003). "Pulmonary alveolar proteinosis". N. Engl. J. Med. 349 (26): 2527-39. doi:10.1056/NEJMra023226. PMID 14695413. http://content.nejm.org/cgi/content/extract/349/26/2527.
- ↑ 2.0 2.1 Lin, FC.; Chang, GD.; Chern, MS.; Chen, YC.; Chang, SC. (Jun 2006). "Clinical significance of anti-GM-CSF antibodies in idiopathic pulmonary alveolar proteinosis.". Thorax 61 (6): 528-34. doi:10.1136/thx.2005.054171. PMID 16517574.
- ↑ Bhattacharyya, D.; Barthwal, MS.; Katoch, CD.; Rohatgi, MG.; Hasnain, S.; Rai, SP.; Arora, A. (Jan 2013). "Primary alveolar proteinosis - A report of two cases.". Med J Armed Forces India 69 (1): 90-3. doi:10.1016/j.mjafi.2012.02.016. PMID 24532945.
- ↑ Leslie, Kevin O.; Wick, Mark R. (2004). Practical Pulmonary Pathology: A Diagnostic Approach (1st ed.). Churchill Livingstone. pp. 248. ISBN 978-0443066313.
- ↑ Leslie KO (May 2009). "My approach to interstitial lung disease using clinical, radiological and histopathological patterns". J. Clin. Pathol. 62 (5): 387–401. doi:10.1136/jcp.2008.059782. PMC 2668105. PMID 19398592. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2668105/.
- ↑ Ben-Dov, I.; Segel, MJ. (Jan 2014). "Autoimmune pulmonary alveolar proteinosis: Clinical course and diagnostic criteria.". Autoimmun Rev. doi:10.1016/j.autrev.2014.01.046. PMID 24424195.
- ↑ Mikami, T.; Yamamoto, Y.; Yokoyama, M.; Okayasu, I. (Dec 1997). "Pulmonary alveolar proteinosis: diagnosis using routinely processed smears of bronchoalveolar lavage fluid.". J Clin Pathol 50 (12): 981-4. PMID 9516877.
- ↑ Meng, ZL.; Liu, HR.; Liang, ZY.; Zhang, SY. (Sep 2005). "[Pathologic feature and diagnosis of pulmonary alveolar proteinosis].". Zhonghua Bing Li Xue Za Zhi 34 (9): 575-8. PMID 16468308.
- ↑ URL: http://pathhsw5m54.ucsf.edu/overview/fungi1a.html. Accessed on: 3 March 2014.
- ↑ Albores, J.; Seki, A.; Fishbein, MC.; Abtin, F.; Lynch, JP.; Wang, T.; Weigt, SS. (Jun 2013). "A rare occurrence of pulmonary alveolar proteinosis after lung transplantation.". Semin Respir Crit Care Med 34 (3): 431-8. doi:10.1055/s-0033-1348472. PMID 23821516.
- ↑ Luo, BF.; Li, HP.; Yi, XH.; Tao, JW.; Lü, HJ.; Fang, X.; Zhang, ZM.; Zhang, L. et al. (Dec 2012). "[The ultrastructural features of sputum deposition and its value in the diagnosis of pulmonary alveolar proteinosis].". Zhonghua Jie He He Hu Xi Za Zhi 35 (12): 887-91. PMID 23328177.