Pilocytic astrocytoma
Jump to navigation
Jump to search
The printable version is no longer supported and may have rendering errors. Please update your browser bookmarks and please use the default browser print function instead.
| Pilocytic astrocytoma | |
|---|---|
| Diagnosis in short | |
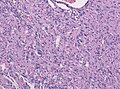
 Pilocytic astrocytoma. Smear. H&E stain. | |
| LM DDx | piloid gliosis, oligodendroglioma, glioblastoma |
| Stains | PAS-D +ve (eosinophilic granular bodies) |
| IHC | GFAP +ve |
| Gross | usually cerebellar +/-cystic |
| Site | brain - usu. cerebellum |
|
| |
| Prevalence | common - esp. in children |
| Prognosis | good (WHO Grade I) |
Pilocytic astrocytoma, abbreviated PA, is a low-grade astrocytoma. It the most common glioma in children.
General
- Low-grade astrocytoma - WHO Grade I by definition, but rare anaplastic forms have been described.
- Classically in the cerebellum in children; most common glioma in children.[1]
- The optic glioma is associated with neurofibromatosis 1.
- Rare variants include Pilomyxoid astrocytoma and Anaplastic pilocytic astrocytoma.
Imaging
- Well-defined, T2-hyperintense.
- Strong CM enhancement.
- May contain cysts.
- Associated with midline structures.
Gross
Features:[1]
- Usually well-circumscribed, soft.
- Can be cystic with mural nodule.
- Optic gliomas may present as fusiform mass.
- Occ. calcium deposits and hemosiderin.
Microscopic
Features:[2]
- Classically biphasic (though either may be absent):
- Fibrillar.
- Microcystic/loose.
- Hair-like fibres ~ 1 micrometer; pilo- = hair.[3]
- Best seen on smear or with GFAP IHC.
- Rosenthal fibres - key feature.
- May be rare. Not pathognomonic (see below).
- Eosinophilic granular bodies.
- Low cellularity - when compared to medulloblastoma and ependymoma.
Notes:
- +/-Microvascular proliferation.
- +/-Focal necrosis.
- Necrosis with pseudopalisading more likely glioblastoma.
- +/-Mitoses - not significant in the context of the Dx.
DDx (of Rosenthal fibers):[4]
- Chronic reactive gliosis.
- Subependymoma.
- Ganglioglioma.
- Alexander's disease (rare leukodystrophy).
DDx of pilocystic astrocytoma (brief):
- Piloid gliosis (esp. in sellar lesions).
- Oligodendroglioma.
- Glioblastoma (uncommon - but important).
- Tanycytic Ependymoma
- Pilocytic tumor components may be found in Ganglioglioma, DNET, RGNT
Images
Smears
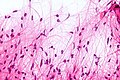
Bipolar cells with hair-like processes - smear - very high mag. (WC)
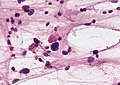
EGBs - smear. (WC/AFIP)
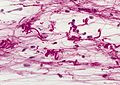
Rosenthal fibres - smear. (WC/AFIP)


Sections
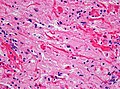
Rosenthal fibres. (WC)
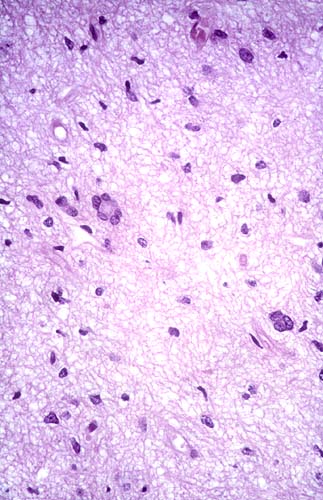
Occasional pleomorphism. (WC)
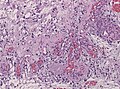
Microvascular proliferation. (WC)



www:
- Rosenthal fibre (ouhsc.edu).
- Pilocytic astrocytoma (upmc.edu).
- Pilocytic astrocytoma - another case (upmc.edu).
- Pilocytic astrocytoma - pennies on a plate (upmc.edu).[5]
- Pilocytic astrocytoma (upmc.edu).
{kind=link}
Stains
- PAS-D: eosinophilic granular bodies +ve.
IHC
Features:[6]
- GFAP +ve (fibres).
- CD68: may have a significant macrophage component.
- KI-67: may be "high" (~20% ???).
- Olig 2: Usually strongly present.[7]
- IDH1 (R132H) -ve.
- H3F3A (K27M) -ve.
Molecular
- Almost all alteration associated with the MAPK pathway.[8]
- KIAA1549-BRAF fusion transcripts most common in sporadic PA (up to 2/3 of all cases).
- DDx: Fusion reported in rare Diffuse Leptomeingeal Glioneuronal Tumors and Oligodendroglioma.
- Rarely BRAF, KRAS or FGFR1 mutations, NTRK2, SRGAP3-RAF1 or FAM131B-BRAF fusions.[9][10]
- Up to 15% of all NF1 patients develop a PA ("optic glioma" as predilection).[11]
- Rare reports of PA in Noonan-Syndrome (PTPN11 mutation).[12]
Prognosis
- Excellent (10-year OS: 90%)
- In thalamic/chiasmatic region not so good (incomplete resection, often Pilomyxoid astrocytoma).
- Primary treatment: surgery. Incomplete resection: RT has to be considered.
- Chx is given in rare cases that are still progredient[13]
See also
References
- ↑ 1.0 1.1 Perry, Arie; Brat, Daniel J. (2010). Practical Surgical Neuropathology: A Diagnostic Approach: A Volume in the Pattern Recognition series (1st ed.). Churchill Livingstone. pp. 82. ISBN 978-0443069826.
- ↑ Perry, Arie; Brat, Daniel J. (2010). Practical Surgical Neuropathology: A Diagnostic Approach: A Volume in the Pattern Recognition series (1st ed.). Churchill Livingstone. pp. 82-4. ISBN 978-0443069826.
- ↑ URL: http://dictionary.reference.com/browse/pilo-. Accessed on: 24 November 2010.
- ↑ Munoz D. 9 Mar 2009.
- ↑ URL: http://path.upmc.edu/cases/case195.html. Accessed on: 8 January 2012.
- ↑ Perry, Arie; Brat, Daniel J. (2010). Practical Surgical Neuropathology: A Diagnostic Approach: A Volume in the Pattern Recognition series (1st ed.). Churchill Livingstone. pp. 84. ISBN 978-0443069826.
- ↑ Otero, JJ.; Rowitch, D.; Vandenberg, S. (Sep 2011). "OLIG2 is differentially expressed in pediatric astrocytic and in ependymal neoplasms.". J Neurooncol 104 (2): 423-38. doi:10.1007/s11060-010-0509-x. PMID 21193945.
- ↑ Collins, VP.; Jones, DT.; Giannini, C. (Jun 2015). "Pilocytic astrocytoma: pathology, molecular mechanisms and markers.". Acta Neuropathol 129 (6): 775-88. doi:10.1007/s00401-015-1410-7. PMID 25792358.
- ↑ Jones, DT.; Hutter, B.; Jäger, N.; Korshunov, A.; Kool, M.; Warnatz, HJ.; Zichner, T.; Lambert, SR. et al. (Aug 2013). "Recurrent somatic alterations of FGFR1 and NTRK2 in pilocytic astrocytoma.". Nat Genet 45 (8): 927-32. doi:10.1038/ng.2682. PMID 23817572.
- ↑ Cin, H.; Meyer, C.; Herr, R.; Janzarik, WG.; Lambert, S.; Jones, DT.; Jacob, K.; Benner, A. et al. (Jun 2011). "Oncogenic FAM131B-BRAF fusion resulting from 7q34 deletion comprises an alternative mechanism of MAPK pathway activation in pilocytic astrocytoma.". Acta Neuropathol 121 (6): 763-74. doi:10.1007/s00401-011-0817-z. PMID 21424530.
- ↑ Friedrich, RE.; Nuding, MA. (Aug 2016). "Optic Pathway Glioma and Cerebral Focal Abnormal Signal Intensity in Patients with Neurofibromatosis Type 1: Characteristics, Treatment Choices and Follow-up in 134 Affected Individuals and a Brief Review of the Literature.". Anticancer Res 36 (8): 4095-121. PMID 27466519.
- ↑ Jones, DT.; Hutter, B.; Jäger, N.; Korshunov, A.; Kool, M.; Warnatz, HJ.; Zichner, T.; Lambert, SR. et al. (Aug 2013). "Recurrent somatic alterations of FGFR1 and NTRK2 in pilocytic astrocytoma.". Nat Genet 45 (8): 927-32. doi:10.1038/ng.2682. PMID 23817572.
- ↑ Metts, RD.; Bartynski, W.; Welsh, CT.; Kinsman, S.; Bredlau, AL. (Mar 2017). "Bevacizumab Therapy for Pilomyxoid Astrocytoma.". J Pediatr Hematol Oncol. doi:10.1097/MPH.0000000000000824. PMID 28338567.