Difference between revisions of "Mucoepidermoid carcinoma"
Jump to navigation
Jump to search
(more) |
|||
| Line 126: | Line 126: | ||
==See also== | ==See also== | ||
*[[Salivary glands]]. | *[[Salivary glands]]. | ||
*[[Squamous cell carcinoma]]. | |||
==References== | ==References== | ||
Revision as of 15:06, 10 November 2013
| Mucoepidermoid carcinoma | |
|---|---|
| Diagnosis in short | |
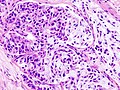
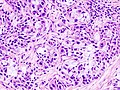
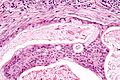
 Mucoepidermoid carcinoma. H&E stain. | |
|
| |
| LM | mucous cells (abundant fluffy cytoplasm and large mucin vacuoles - nucleus distorted by mucin vacuole, cells may be scarce); epidermoid cells (non-keratinized, polygonal squamoid cell with clear or oncocytic cytoplasm); architecture - cystic (low grade) or solid (high grade) |
| LM DDx | squamous cell carcinoma of the head and neck, adenosquamous carcinoma |
| Stains | mucous cells: alcian blue stain +ve, mucicarmine stain +ve |
| Molecular | t(11;19)(q21;p13) |
| Gross | solid, cystic or both |
| Site | salivary gland, classically parotid gland |
|
| |
| Signs | mass lesion |
| Prevalence | most common malignant salivary gland tumour, generally uncommon |
Mucoepidermoid carcinoma, abbreviated MEC, the is the most common malignant neoplasm of the salivary gland.
General
- Most common malignant neoplasm of salivary gland in all age groups.[1]
- Female:male ~= 3:2.
- Site: parotid > submandibular.
Gross
- Cystic or solid, usu. a mix of both.
Microscopic
Features:
- Architecture:[2]
- Cystic (low grade).
- Solid (high grade).
- Mucous cells with abundant fluffy cytoplasm and large mucin vacuoles - key feature.
- Nucleus distorted by mucin vacuole.
- Mucous cell may be scarce - more difficult to diagnose.
- Epidermoid cells:
Notes:
- The classic description - composed of 3 cell types: epidermoid, intermediate, and mucin producing.[3]
- "Intermediate cells" are described in textbooks. Weinreb thinks they are a pretty much a myth.[4]
- Mucin vacuoles may be rare; in a superficial glance -- it may mimic squamous cell carcinoma.
- The thought of high-grade MEC should prompt consideration of squamous cell carcinoma.
DDx:[5]
Images
Mucoepidermoid carcinoma 2. (WC)
Mucoepidermoid carcinoma 3. (WC)

Mucoepidermoid carcinoma - 2 - intermed. mag. (WC/Nephron)

Mucoepidermoid carcinoma - 2 - high mag. (WC/Nephron)
Mucoepidermoid carcinoma - 2 - very high mag. (WC/Nephron)
_HE_stain.jpg)
_HE_stain.jpg)


www:
Subtypes
- Conventional.
- Oncocytic.
- Definition: composed of 50% oncocytes.
- Good outcome.[6]
- Clear cell.
- Unicystic (cystadenocarcinoma).
- Based on the gross. (???)
- Sclerosing MEC +/- eosinophilia.
- Rare.
Grading
General:
Notes:
- Both systems have their pros and cons.
- Weinreb uses the AFIP system with a slight modification.
AFIP
- Low cystic content (<20%) - 2 points.
- Perineural invasion - 2 points.
- Necrosis - 3 points.
- Mitoses > 4 per 10 HPFs (HPF not defined in paper - see HPFitis) - 3 points.
- Anaplasia - 4 points.
Scoring:
- Low grade = 0-4 points.
- Intermediate grade = 5-6 points.
- High grade = 7+ points.
Weinreb modification
Weinreb looks for the following:
- Tumour invades in small nests/islands - 2 points.
- If applicable, the two points are added to the AFIP score.
- The tumour is graded using the AFIP (scoring) cut points -- see above.
Notes:
- It seems pointless to memorize this but it is occasionally asked on exams.
- How to remember: think of the Nottingham grading system (architecture, mitoses, nuclear grade) + necrosis + LVI.
Stains
Mucous cells:
- Alcian blue +ve.
- Mucicarmine +ve.
Molecular
- t(11;19)(q21;p13) -- MECT1-MAML2 fusion.[9][10]
- Present in ~65% of MECs.
- Presence assoc. with low-grade MEC (vs. high-grade MEC) & favourable prognosis.
- Not seen in tumours that are in the DDx of MEC.
See also
References
- ↑ URL: http://path.upmc.edu/cases/case715/dx.html. Accessed on: 2 February 2012.
- ↑ URL: http://moon.ouhsc.edu/kfung/jty1/opaq/PathQuiz/D2A001-PQ01-M.htm. Accessed on: 19 October 2010.
- ↑ Lennerz, JK.; Perry, A.; Mills, JC.; Huettner, PC.; Pfeifer, JD. (Jun 2009). "Mucoepidermoid carcinoma of the cervix: another tumor with the t(11;19)-associated CRTC1-MAML2 gene fusion.". Am J Surg Pathol 33 (6): 835-43. doi:10.1097/PAS.0b013e318190cf5b. PMID 19092631.
- ↑ IW. 10 January 2011.
- ↑ Mokhtari, S.; Mokhtari, S. (2012). "Clinical features and differential diagnoses in laryngeal mucoepidermoid carcinoma.". Clin Med Insights Pathol 5: 1-6. doi:10.4137/CPath.S8435. PMID 22262946.
- ↑ Weinreb I, Seethala RR, Perez-Ordoñez B, Chetty R, Hoschar AP, Hunt JL (March 2009). "Oncocytic mucoepidermoid carcinoma: clinicopathologic description in a series of 12 cases". Am. J. Surg. Pathol. 33 (3): 409–16. doi:10.1097/PAS.0b013e318184b36d. PMID 18971778.
- ↑ Goode RK, Auclair PL, Ellis GL (April 1998). "Mucoepidermoid carcinoma of the major salivary glands: clinical and histopathologic analysis of 234 cases with evaluation of grading criteria". Cancer 82 (7): 1217–24. PMID 9529011.
- ↑ Brandwein MS, Ivanov K, Wallace DI, et al. (July 2001). "Mucoepidermoid carcinoma: a clinicopathologic study of 80 patients with special reference to histological grading". Am. J. Surg. Pathol. 25 (7): 835–45. PMID 11420454.
- ↑ Tonon G, Modi S, Wu L, et al. (February 2003). "t(11;19)(q21;p13) translocation in mucoepidermoid carcinoma creates a novel fusion product that disrupts a Notch signaling pathway". Nat. Genet. 33 (2): 208–13. doi:10.1038/ng1083. PMID 12539049.
- ↑ Seethala RR, Dacic S, Cieply K, Kelly LM, Nikiforova MN (August 2010). "A reappraisal of the MECT1/MAML2 translocation in salivary mucoepidermoid carcinomas". Am. J. Surg. Pathol. 34 (8): 1106–21. doi:10.1097/PAS.0b013e3181de3021. PMID 20588178.