Invasive ductal carcinoma of the pancreas
Jump to navigation
Jump to search
Invasive ductal carcinoma of the pancreas is the most common type of pancreatic cancer.
| Invasive ductal carcinoma of the pancreas | |
|---|---|
| Diagnosis in short | |
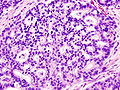
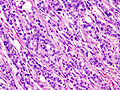
_Case_01.jpg) Pancreatic adenocarcinoma. H&E stain. | |
| LM DDx | chronic pancreatitis, cholangiocarcinoma |
| Molecular | +/-BRCA2 carrier |
| Site | pancreas, typically head of pancreas |
|
| |
| Associated Dx | pancreatic intraepithelial neoplasia, +/-diabetes mellitus |
| Clinical history | +/-smoking |
| Prevalence | common for site |
| Radiology | pancreatic mass |
| Prognosis | very poor |
| Clin. DDx | chronic pancreatitis, other pancreatic tumours |
| Treatment | surgery if possible |
It is typically gland forming and thus also referred to as pancreatic ductal adenocarcinoma and pancreatic adenocarcinoma.
Less specific terms that are used when the context is clear include ductal adenocarcinoma and invasive ductal carcinoma.
General
- Most common type of pancreatic cancer.[1]
- Location: usually in the head ~60%.
- 15% in the body, 5% tail, 20% diffuse (head, body & tail).[2]
- The vast majority of pancreatic cancers are solitary, but multifocal disease can occur.
- Abysmal prognosis.
Risk factors:[3]
- Smoking (RR ~ 2).
- Pancreatitis.
- Family history, esp. BRCA2.
- Diabetes mellitus - modest risk increase (RR ~ 1.5-2).
- Previous gastrectomy.
- Heavy drinking of alcohol may weakly increase risk.
Gross
- Firm, sclerotic and poorly defined masses that replace the normal lobular architecture of the gland.
- Cut surface are yellow to white.
- The mean diameter of pancreatic head tumor is between 2.5-3.5cm.
Microscopic
Features:[7]
- Often glandular, may be solid.
- Nuclei.
- May be bland - little pleomorphism.
- Often small nuclei.
- Sometimes coffee-bean appearance.
- Cytoplasm - granular, abundant.
- Quasi endocrine look.
- May stain positive for endocrine markers.
Other features:
- +/-Necrosis.
- +/-Myxoid degeneration.
- +/-Cells around vessels.
DDx:
Images
Pancreatic adenocarcinoma (WC)
Pancreatic adenocarcinoma (WC)

Normal pancreas, pancreatic intraepithelial neoplasia and pancreatic carcinoma (WC)
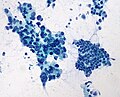
Pancreatic adenocarcinoma - cytopathology (WC)
_Case_01.jpg)

.jpg)
www:
IHC
Features:[9]
- CD7 +ve.
- CD20 +ve.
- SMAD4 -ve ~55% of cases -- stomach usually +ve.
- CDX2 -ve/+ve.
- CEA +ve.[10]
Sign out
MASS, PANCREAS, CORE BIOPSY: - ADENOCARCINOMA, MODERATELY DIFFERENTIATED.
Note:
- On biopsy, it isn't easy to separate from cholangiocarcinoma. Thus, it is better to stay vague.
See also
References
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 237. ISBN 978-0781765275.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 950. ISBN 0-7216-0187-1.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 471. ISBN 978-1416054542.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 470-1. ISBN 978-1416054542.
- ↑ Furukawa, T. (Nov 2009). "Molecular pathology of pancreatic cancer: implications for molecular targeting therapy.". Clin Gastroenterol Hepatol 7 (11 Suppl): S35-9. doi:10.1016/j.cgh.2009.07.035. PMID 19896096.
- ↑ Online 'Mendelian Inheritance in Man' (OMIM) 600160
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 951. ISBN 0-7216-0187-1.
- ↑ Adsay, NV.; Bandyopadhyay, S.; Basturk, O.; Othman, M.; Cheng, JD.; Klöppel, G.; Klimstra, DS. (Nov 2004). "Chronic pancreatitis or pancreatic ductal adenocarcinoma?". Semin Diagn Pathol 21 (4): 268-76. PMID 16273946.
- ↑ Lester, Susan Carole (2010). Manual of Surgical Pathology (3rd ed.). Saunders. pp. 94. ISBN 978-0-323-06516-0.
- ↑ Adsay, NV.; Basturk, O.; Cheng, JD.; Andea, AA. (Oct 2005). "Ductal neoplasia of the pancreas: nosologic, clinicopathologic, and biologic aspects.". Semin Radiat Oncol 15 (4): 254-64. doi:10.1016/j.semradonc.2005.04.001. PMID 16183479.