Endometrial carcinoma
Endometrial carcinoma, also endometrial adenocarcinoma, is a common gynecologic malingnancy[1] that often arises from endometrial hyperplasia. The incidence of endometrial carcinoma is increasing, as the proportion of obese individuals is increasing.
An introduction to the endometrium is in the article endometrium.
Clinical
Risk factors
Risk factors for endometrial carcinoma - mnemonic COLD NUT:[2]
- Cancer Hx (ovarian, breast, colon).
- Obesity.
- Late menopause.
- Diabetes.
- Nulliparity.
- Unopposed estrogen (polycystic ovarian syndrome (PCOS), anovulation, hormone replacement therapy (HRT)).
- Tamoxifen use.
Family history
Several syndromes are seen in association with endometrial cancer:[5]
- Cowden syndrome (PTEN mutation) - most common.
- Associated with endometrioid endometrial carcinoma.
- Lynch syndrome (mutation of a mismatch repair gene - there are several[6]).
- Associated with non-endometrioid endometrial carcinoma.[5]
- Autosomal dominant.
Management
- Hysterectomy is the standard treatment for endometrial carcinoma.
Details:
- Low grade and low stage endometrioid carcinoma: total hysterectomy (includes cervix).
- Non-endometrioid or high stage endometrioid or high-grade endometrioid: radical hysterectomy (includes cervix, vaginal cuff, parametrial tissue).
Subtypes - overview
They are commonly grouped based on clinicopathologic features:[9][10]
| Feature | Type I | Type II |
|---|---|---|
| Histologic types | endometrioid endometrial carcinoma, mucinous endometrial carcinoma | serous carcinoma of the endometrium, clear cell carcinoma of the endometrium, undifferentiated carcinoma |
| Clinical characteristics |
premenopausal, estrogen excess, obesity | postmenopausal, no estrogen excess, atrophic endometrium |
| Prognosis | good | poor |
| Genetic abnormalities |
microsatellite instability, PTEN & KRAS mutations | p53 mutations |
| Precursor lesion(s) | endometrial hyperplasia | possibly endometrial intraepithelial carcinoma[11] † |
Notes:
- † Endometrial intraepithelial carcinoma should not be confused with endometrial intraepithelial neoplasia (EIN).
Grading (FIGO)
Based on gland formation & adjusted by nuclear pleomorphism:[12][13][14][15]
- Grade 1: <5% solid component.
- Grade 2: 5-50% solid component.
- Grade 3: >50% solid component.
Modifiers/adjustment:
- High grade nuclei upgrades cancer by one; high grade nuclei = increased size, irregular large nucleoli, irregular chromatin pattern (clumped, coarse).[16]
Notes:
- Officially only sanctioned for endometrioid endometrial carcinoma.
- May be used for mucinous endometrial carcinoma.
- Papillary serous carcinoma and clear cell carcinomas are not assigned a grade or grade 3 by definition.
Staging
- Stage I: confined to uterine body.
- Ia = less than half of myometrium.
- Ib = greater than half of myometrium.
- Stage II: uterus + cervix.
- II = cervical stroma involved.
- Cervical epithelium involvement does not change stage.
- II = cervical stroma involved.
- Stage III: outside uterus - but inside pelvis.
- IIIa - involves serosa and/or adnexa (direct extension or metastasis)
- IIIb - vaginal involvement (direct extension or metastasis) or parametrial involvement
- Stage IV: outside true pelvis or in mucosa of bladder or GI tract.
Specific types
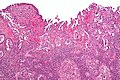
Endometrioid endometrial carcinoma
- AKA endometrioid endometrial adenocarcinoma.
General
- Good prognosis - usually.
- Women in 40s & 50s.
- Associated with estrogen excess.
- Typical patient is obese.
Gross
- Thickened endometrium.
Microscopic
Features:
- Atypical (ovoid) glands with - one of the following four:[21][22][23]
- Desmoplastic stromal response.
- Confluent cribriform growth. †
- Extensive papillary growth. †
- Severe cytologic atypia. †
- Squamous metaplasia - very common.
- Look for squamous morules:
- Ball of cells with an intensely eosinophilic cytoplasm - key feature.
- Central nucleus.
- Intercellular bridges - may be hard to find.
- +/-Dyskeratotic cells.
- Look for squamous morules:
Notes:
- † There is a size cut-off for criteria 2, 3 and 4: > 2.1 mm.[22]
- Dyskeratosis = abnormal keratinization;[24] classically have intensely eosinophilic cytoplasm +/- nuclear fragmentation (karyorrhexis) - see: several dyskeratotic cells.
- Squamous metaplasia != neoplastic -- it may occur due to hormones.[25]
- Squamous morules in endometrioid endometrial carcinoma - not associated with HPV infection.[26]
DDx:
- Complex endometrial hyperplasia with atypia.
- Complex endometrial hyperplasia.
- Microglandular hyperplasia of the cervix.
- Endocervical adenocarcinoma.
- Serous carcinoma of the endometrium - esp. if high-grade nuclear features are present diffusely.
- Clear cell carcinoma of the endometrium - esp. when clear cells present.
Images
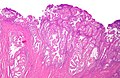
EEA - low mag. (WC)
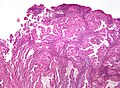
EEA - intermed. mag. (WC)
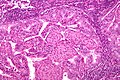
EEA - high mag. (WC)
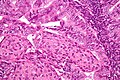
EEA - very high mag. (WC)




www:
IHC
- Vimentin +ve.
- ER +ve.
- PR +ve.
Others:
- p16 -ve -- positive in serous endometrial carcinoma[27] and endocervical adenocarcinoma.
- CEA -ve.
Sign out
ENDOMETRIUM, BIOPSY: - ENDOMETRIOID ENDOMETRIAL ADENOCARCINOMA, FIGO GRADE I/III.
Micro
The sections show endometrium with complex, fused and cribriform glands with scant intervening stroma over a region measuring greater than 2.1 millimetres. Focally, a desmoplastic stroma is also identified. No nuclear atypia is appreciated.
Endocervical versus endometrial - biopsy
The foamy histiocytes in the stroma and lack of desmoplasia slightly favour an endometrial origin; however, the lesion would be best classified with an excisional specimen and in conjunction with the clinical impression.
Mucinous carcinoma of the endometrium
- AKA endometrial mucinous carcinoma.
General
- Type I endometrial carcinoma.[citation needed]
- Good prognosis.
Microscopic
Features:[10]
- Cells with intracytoplasmic mucin (>50% of tumour).
- Usu. mild-to-moderate nuclear atypia.
DDx:
- Endometrioid endometrial carcinoma.
- Metastatic mucinous carcinoma.
IHC
Features:[28]
- ER-alpha +ve.
- PR-alpha +ve.
- PR-beta +ve.
Serous carcinoma of the endometrium
- AKA serous endometrial carcinoma.
- AKA serous carcinoma of the uterus.
- AKA uterine serous carcinoma.
- AKA uterine papillary serous carcinoma.
General
- Arising in the setting of atrophy.
- Usually post-menopausal.
- Precursor lesion: endometrial intraepithelial carcinoma.[11]
- Aggressive behaviour - high probability of disseminated disease.
Gross
- Thin endometrium.
- +/-Polypoid mass.
Microscopic
Features - serous:
- Architecture - classically papillary.
- May be glomeruloid, tubulocystic, solid (uncommon).
- Cytology:
- Columnar or cuboidal cells.
- Moderate to marked nuclear pleomorphism - variation of size, shape and staining.
- Large nuclear size variation between cells often esp. prominent.
- Singular prominent, classically red, nucleolus.
- Moderate to marked nuclear pleomorphism - variation of size, shape and staining.
- Columnar or cuboidal cells.
- +/-Psammoma bodies.
DDx:
- High-grade endometrioid endometrial carcinoma - uncommon, typically younger age.
- Clear cell carcinoma of the endometrium - usually have less nuclear pleomorphism and less mitoses.
- Arias-Stella reaction.
Images
Uterine serous carcinoma - low mag. (WC)
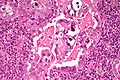
Uterine serous carcinoma - high mag. (WC)


{kind=link}
IHC
- p16 +ve[27] - should be strong.
- p53 +ve[29] diffuse & strong > 50% or 75% of the tumour - depending on the paper one reads.
- Subset is p53 -ve.
- Ki-67 "high" - no cut-point defined.
- ER often -ve.[30]
- PR often -ve.[30]
High-grade endometrioid carcinoma versus serous carcinoma:[31]
- p53 -ve, PR +ve, PTEN loss -- suggest endometrioid.
- p16 and PTEN superior to ER, PR, and p53.[32]
Notes:
- p16 +ve in tubal metaplasia.[33]
- WT1 usu. -ve -- useful to differentiate from ovarian serous carcinoma.[34]
Clear cell carcinoma of the endometrium
General
- Ten-year survival ~ 40%.[35]
- Uncommon <=5 % of endometrial carcinomas.[36]
- Type II endometrial cancer - estrogen-independent, usually post-menopausal women.
Microscopic
Features:[36]
- Clear cells - with moderate nuclear pleomorphism - key feature.
- Classically clear cells... but not always.
- Hobnail pattern -- apical cytoplasm > cytoplasm on basement membrane.
- Usually tubular/cystic, may be solid or papillary.
- Papillae may be pseudopapillae -- with edema instead of vessels.
Notes:
- May have psammoma bodies - esp. in papillary area; may lead to confusion with serous carcinoma.
DDx:
- Serous endometrial carcinoma - usually has more nuclear pleomorphism, esp. cell size variation.
- High grade endometrioid endometrial carcinoma - have non-clear areas.[36]
- Arias-Stella reaction - esp. in the context of pregnancy.
- Papillary cystadenoma - benign; bland nuclei.[36]
DDx weird stuff:[36]
- PEComa.
- Epithelioid leiomyosarcoma.
Images
www:
- Clear cell carcinoma of the endometrium - high mag. (webpathology.com).
- Clear cell carcinoma of the endometrium - low mag. (webpathology.com).
Stains
- PAS-D stain +ve ~ glycogen.[36]
IHC
Features:[37]
- p53 -ve usu. - unlike uterine serous carcinoma.
- ER -ve.
- PR -ve.
Others:[36]
- CAM5.2 +ve.
- CK34betaE12 +ve.
Note:
- HNF1beta - not useful[38] - unlike for ovarian clear cell carcinoma.
See also
- Endometrium.
- Uterine tumours - other uterine tumours, e.g. carcinosarcoma, endometrial stromal sarcoma.
- Uterine cervix.
- Gynecologic pathology - overview.
References
- ↑ Fowler W, Mutch D (September 2008). "Management of endometrial cancer". Womens Health (Lond Engl) 4 (5): 479–89. doi:10.2217/17455057.4.5.479. PMID 19072487.
- ↑ Greenwald, J.; Heng, M. (2007). Toronto Notes for Medical Students 2007 (2007 ed.). The Toronto Notes Inc. for Medical Students Inc.. pp. GY40. ISBN 978-0968592878.
- ↑ Brown, K. (Sep 2009). "Is tamoxifen a genotoxic carcinogen in women?". Mutagenesis 24 (5): 391-404. doi:10.1093/mutage/gep022. PMID 19505894.
- ↑ Ashraf, M.; Biswas, J.; Majumdar, S.; Nayak, S.; Alam, N.; Mukherjee, KK.; Gupta, S.. "Tamoxifen use in Indian women--adverse effects revisited.". Asian Pac J Cancer Prev 10 (4): 609-12. PMID 19827879.
- ↑ 5.0 5.1 Okuda T, Sekizawa A, Purwosunu Y, et al. (2010). "Genetics of endometrial cancers". Obstet Gynecol Int 2010: 984013. doi:10.1155/2010/984013. PMC 2852605. PMID 20396392. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2852605/.
- ↑ Online 'Mendelian Inheritance in Man' (OMIM) 120435
- ↑ Zivanovic O, Carter J, Kauff ND, Barakat RR (December 2009). "A review of the challenges faced in the conservative treatment of young women with endometrial carcinoma and risk of ovarian cancer". Gynecol. Oncol. 115 (3): 504–9. doi:10.1016/j.ygyno.2009.08.011. PMID 19758691.
- ↑ Ware, RA.; van Nagell, JR. (2010). "Radical hysterectomy with pelvic lymphadenectomy: indications, technique, and complications.". Obstet Gynecol Int 2010. doi:10.1155/2010/587610. PMID 20871657.
- ↑ Lim, D.; Oliva, E. (Nov 2010). "Nonendometrioid endometrial carcinomas.". Semin Diagn Pathol 27 (4): 241-60. PMID 21309259.
- ↑ 10.0 10.1 Nucci, Marisa R.; Oliva, Esther (2009). Gynecologic Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 241. ISBN 978-0443069208.
- ↑ 11.0 11.1 Roelofsen, T.; van Kempen, LC.; van der Laak, JA.; van Ham, MA.; Bulten, J.; Massuger, LF. (Mar 2012). "Concurrent endometrial intraepithelial carcinoma (EIC) and serous ovarian cancer: can EIC be seen as the precursor lesion?". Int J Gynecol Cancer 22 (3): 457-64. doi:10.1097/IGC.0b013e3182434a81. PMID 22249577.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 1087-8. ISBN 0-7216-0187-1.
- ↑ URL: http://www.pathologyoutlines.com/uterus.html#endometrialcarc.
- ↑ URL: http://www.emedicine.com/med/topic2832.htm.
- ↑ Ayhan A, Taskiran C, Yuce K, Kucukali T (January 2003). "The prognostic value of nuclear grading and the revised FIGO grading of endometrial adenocarcinoma". Int. J. Gynecol. Pathol. 22 (1): 71–4. PMID 12496701.
- ↑ Tadrous, Paul.J. Diagnostic Criteria Handbook in Histopathology: A Surgical Pathology Vade Mecum (1st ed.). Wiley. pp. 240. ISBN 978-0470519035.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 1088. ISBN 0-7216-0187-1.
- ↑ http://www.emedicine.com/med/topic2832.htm
- ↑ Staging with groovy graphics (cancerfacts.com)
- ↑ URL: http://en.wikibooks.org/wiki/Radiation_Oncology/Endometrium/Staging. Accessed on: 2 May 2012.
- ↑ Nucci, Marisa R.; Oliva, Esther (2009). Gynecologic Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 239. ISBN 978-0443069208.
- ↑ 22.0 22.1 Kurman, RJ.; Norris, HJ. (Jun 1982). "Evaluation of criteria for distinguishing atypical endometrial hyperplasia from well-differentiated carcinoma.". Cancer 49 (12): 2547-59. PMID 7074572.
- ↑ URL: http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2011/Endometrium_11protocol.pdf. Accessed on: 12 January 2012.
- ↑ URL: http://dictionary.reference.com/browse/dyskeratosis. Accessed on: 5 September 2011.
- ↑ Miranda, MC.; Mazur, MT. (May 1995). "Endometrial squamous metaplasia. An unusual response to progestin therapy of hyperplasia.". Arch Pathol Lab Med 119 (5): 458-60. PMID 7748076.
- ↑ Chinen, K.; Kamiyama, K.; Kinjo, T.; Arasaki, A.; Ihama, Y.; Hamada, T.; Iwamasa, T. (Sep 2004). "Morules in endometrial carcinoma and benign endometrial lesions differ from squamous differentiation tissue and are not infected with human papillomavirus.". J Clin Pathol 57 (9): 918-26. doi:10.1136/jcp.2004.017996. PMID 15333650.
- ↑ 27.0 27.1 Chiesa-Vottero, AG.; Malpica, A.; Deavers, MT.; Broaddus, R.; Nuovo, GJ.; Silva, EG. (Jul 2007). "Immunohistochemical overexpression of p16 and p53 in uterine serous carcinoma and ovarian high-grade serous carcinoma.". Int J Gynecol Pathol 26 (3): 328-33. doi:10.1097/01.pgp.0000235065.31301.3e. PMID 17581420.
- ↑ Shabani, N.; Mylonas, I.; Jeschke, U.; Thaqi, A.; Kuhn, C.; Puchner, T.; Friese, K.. "Expression of estrogen receptors alpha and beta, and progesterone receptors A and B in human mucinous carcinoma of the endometrium.". Anticancer Res 27 (4A): 2027-33. PMID 17649817.
- ↑ Yemelyanova, A.; Ji, H.; Shih, IeM.; Wang, TL.; Wu, LS.; Ronnett, BM. (Oct 2009). "Utility of p16 expression for distinction of uterine serous carcinomas from endometrial endometrioid and endocervical adenocarcinomas: immunohistochemical analysis of 201 cases.". Am J Surg Pathol 33 (10): 1504-14. doi:10.1097/PAS.0b013e3181ac35f5. PMID 19623034.
- ↑ 30.0 30.1 Kounelis, S.; Kapranos, N.; Kouri, E.; Coppola, D.; Papadaki, H.; Jones, MW. (Apr 2000). "Immunohistochemical profile of endometrial adenocarcinoma: a study of 61 cases and review of the literature.". Mod Pathol 13 (4): 379-88. doi:10.1038/modpathol.3880062. PMID 10786803.
- ↑ Darvishian, F.; Hummer, AJ.; Thaler, HT.; Bhargava, R.; Linkov, I.; Asher, M.; Soslow, RA. (Dec 2004). "Serous endometrial cancers that mimic endometrioid adenocarcinomas: a clinicopathologic and immunohistochemical study of a group of problematic cases.". Am J Surg Pathol 28 (12): 1568-78. PMID 15577675.
- ↑ Alkushi, A.; Köbel, M.; Kalloger, SE.; Gilks, CB. (Jul 2010). "High-grade endometrial carcinoma: serous and grade 3 endometrioid carcinomas have different immunophenotypes and outcomes.". Int J Gynecol Pathol 29 (4): 343-50. doi:10.1097/PGP.0b013e3181cd6552. PMID 20567148.
- ↑ Horree, N.; Heintz, AP.; Sie-Go, DM.; van Diest, PJ. (2007). "p16 is consistently expressed in endometrial tubal metaplasia.". Cell Oncol 29 (1): 37-45. PMID 17429140.
- ↑ Bárcena, C.; Oliva, E. (Nov 2011). "WT1 expression in the female genital tract.". Adv Anat Pathol 18 (6): 454-65. doi:10.1097/PAP.0b013e318234aaed. PMID 21993272.
- ↑ Abeler, VM.; Vergote, IB.; Kjørstad, KE.; Tropé, CG. (Oct 1996). "Clear cell carcinoma of the endometrium. Prognosis and metastatic pattern.". Cancer 78 (8): 1740-7. PMID 8859187.
- ↑ 36.0 36.1 36.2 36.3 36.4 36.5 36.6 Offman, SL.; Longacre, TA. (Sep 2012). "Clear cell carcinoma of the female genital tract (not everything is as clear as it seems).". Adv Anat Pathol 19 (5): 296-312. doi:10.1097/PAP.0b013e31826663b1. PMID 22885379.
- ↑ Nucci, Marisa R.; Oliva, Esther (2009). Gynecologic Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 250. ISBN 978-0443069208.
- ↑ Fadare, O.; Liang, SX. (Apr 2012). "Diagnostic Utility of Hepatocyte Nuclear Factor 1-Beta Immunoreactivity in Endometrial Carcinomas: Lack of Specificity For Endometrial Clear Cell Carcinoma.". Appl Immunohistochem Mol Morphol. doi:10.1097/PAI.0b013e31824973d1. PMID 22495362.