Desquamative interstitial pneumonia
Jump to navigation
Jump to search
The printable version is no longer supported and may have rendering errors. Please update your browser bookmarks and please use the default browser print function instead.
| Desquamative interstitial pneumonia | |
|---|---|
| Diagnosis in short | |
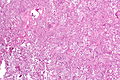
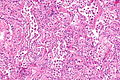
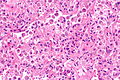
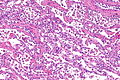
 Desquamative interstitial pneumonia. H&E stain. (WC/Nephron) | |
|
| |
| LM | abundant brown pigmented airspace macrophages (smoker's macrophages), architecture preserved ("linear fibrosis") |
| LM DDx | amiodarone toxicity, fibrotic NSIP, RBILD |
| Site | lung - see diffuse lung diseases |
|
| |
| Associated Dx | +/-smoking |
| Prevalence | rare |
| Radiology | ground glass airspaces changes - usu. all lobes but peripheral predominant and in lower lobe predominant |
| Treatment | stop smoking/remove insult |
Desquamative interstitial pneumonia, abbreviated DIP, is a diffuse lung disease that is strongly associated with smoking.
The term desquamative interstitial pneumonia is a misnomer. The airspace cells that characterize the condition were once thought to represent desquamated epithelial cells, but they are now know to represent macrophages.[1]
General
- Rare.[2]
- Strong association with smoking.[3][4]
- Thought to be advanced RBILD.
- May be seen in non-smokers (up to ~40% of cases) due to occupational exposures, drugs, viral illnesses and autoimmune diseases.[5]
Diagnosis:
- Requires - surgical biopsy.[5]
Treatment:
- Stop smoking/remove or manage underlying cause.
Gross/Radiology
Features:[6]
- Ground glass (airspace changes).
- Usually peripheral predominant (~60% of cases) and lower lobe predominant (~70-75% of cases).
- Typically all lobes are involved - though upper lobe spared in ~20% of cases.
- Fibrotic (radiologic) changes ~50% of cases.
Microscopic
Features:[2]
- Abundant airspace macrophages - usually with brown pigment (so called smoker's macrophages) - key feature.
- Interstitial inflammation or interstitial fibrosis with a preserved architecture - so called "linear fibrosis".
Notes:
- Some fields of view may be indistinguishable from RBILD.
DDx:
Images
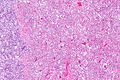
DIP - low mag.
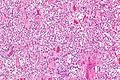
DIP - intermed. mag.
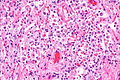
DIP - high mag.
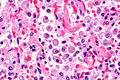
DIP - very high mag.
DIP - low mag.
DIP - intermed. mag.
DIP - high mag.
DIP - intermed mag.







www
Stains
- Macrophages PAS +ve.
See also
References
- ↑ Attili, AK.; Kazerooni, EA.; Gross, BH.; Flaherty, KR.; Myers, JL.; Martinez, FJ.. "Smoking-related interstitial lung disease: radiologic-clinical-pathologic correlation.". Radiographics 28 (5): 1383-96; discussion 1396-8. doi:10.1148/rg.285075223. PMID 18794314. http://pubs.rsna.org/doi/full/10.1148/rg.285075223.
- ↑ 2.0 2.1 Tazelaar, HD.; Wright, JL.; Churg, A. (Mar 2011). "Desquamative interstitial pneumonia.". Histopathology 58 (4): 509-16. doi:10.1111/j.1365-2559.2010.03649.x. PMID 20854463.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 93. ISBN 978-0781765275.
- ↑ Margaritopoulos, GA.; Vasarmidi, E.; Jacob, J.; Wells, AU.; Antoniou, KM. (Sep 2015). "Smoking and interstitial lung diseases.". Eur Respir Rev 24 (137): 428-35. doi:10.1183/16000617.0050-2015. PMID 26324804.
- ↑ 5.0 5.1 Godbert, B.; Wissler, MP.; Vignaud, JM. (Jun 2013). "Desquamative interstitial pneumonia: an analytic review with an emphasis on aetiology.". Eur Respir Rev 22 (128): 117-23. doi:10.1183/09059180.00005812. PMID 23728865.
- ↑ Hartman, TE.; Primack, SL.; Swensen, SJ.; Hansell, D.; McGuinness, G.; Müller, NL. (Jun 1993). "Desquamative interstitial pneumonia: thin-section CT findings in 22 patients.". Radiology 187 (3): 787-90. doi:10.1148/radiology.187.3.8497631. PMID 8497631.