|
|
| (46 intermediate revisions by the same user not shown) |
| Line 1: |
Line 1: |
| '''Colorectal tumours''', especially '''colorectal carcinomas''', are very common. They are the bread and butter of GI pathology. Non-tumour colon is dealt with in the ''[[colon]]'' article. | | '''Colorectal tumours''', especially '''colorectal carcinomas''', are very common. They are the bread and butter of GI pathology. Non-tumour colon is dealt with in the ''[[colon]]'' article. |
| | |
| | ''Colonic tumours'' and ''rectal tumours'' redirect here. |
|
| |
|
| An introduction to gastrointestinal pathology is in the ''[[gastrointestinal pathology]]'' article. The precursor lesion of colorectal carcinoma (CRC) is, typically, an [[adenomatous polyps|adenomatous polyp]]. Polyps are discussed in the ''[[intestinal polyps]]'' article. | | An introduction to gastrointestinal pathology is in the ''[[gastrointestinal pathology]]'' article. The precursor lesion of colorectal carcinoma (CRC) is, typically, an [[adenomatous polyps|adenomatous polyp]]. Polyps are discussed in the ''[[intestinal polyps]]'' article. |
| Line 11: |
Line 13: |
| *[[Mucinous carcinoma]]. | | *[[Mucinous carcinoma]]. |
| **Need > 50% mucinous component.<ref name=pmid17679024 >{{cite journal |author=Tozawa E, Ajioka Y, Watanabe H, ''et al.'' |title=Mucin expression, p53 overexpression, and peritumoral lymphocytic infiltration of advanced colorectal carcinoma with mucus component: is mucinous carcinoma a distinct histological entity? |journal=Pathol. Res. Pract. |volume=203 |issue=8 |pages=567–74 |year=2007 |pmid=17679024 |doi=10.1016/j.prp.2007.04.013 |url=}}</ref> | | **Need > 50% mucinous component.<ref name=pmid17679024 >{{cite journal |author=Tozawa E, Ajioka Y, Watanabe H, ''et al.'' |title=Mucin expression, p53 overexpression, and peritumoral lymphocytic infiltration of advanced colorectal carcinoma with mucus component: is mucinous carcinoma a distinct histological entity? |journal=Pathol. Res. Pract. |volume=203 |issue=8 |pages=567–74 |year=2007 |pmid=17679024 |doi=10.1016/j.prp.2007.04.013 |url=}}</ref> |
| *Adenosquamous carcinoma. | | *[[Adenosquamous carcinoma]]. |
| *Signet-ring carcinoma. | | *Signet-ring carcinoma. |
| *Squamous carcinoma. | | *Squamous carcinoma. |
| Line 28: |
Line 30: |
| *Rare. | | *Rare. |
| **In the context of a rectal tumour, retrograde growth from the [[anus]] should be considered. | | **In the context of a rectal tumour, retrograde growth from the [[anus]] should be considered. |
|
| |
| ==Grading==
| |
| *"Adenocarcinoma in situ" and "high-grade dysplasia" is used interchangeably by many in the colon and rectum.
| |
| **Splitting hairs - ''adenocarcinoma in situ'' is ''invasion into the lamina propria'', high-grade dysplasia does not have lamina propria invasion. Ergo, the difference (in my opinion) amounts to seeing a [[desmoplastic stroma]] (adenocarcinoma) or not seeing one (dysplasia).
| |
|
| |
| Grading of tumours:
| |
| *Tis - in situ (intramucosal).
| |
| *T1 - into submucosa (through mucularis mucosae).
| |
| **This is '''different than elsewhere''', e.g. in the ''small bowel'' tumour cells in the ''lamina propria'' is defined as T1. The rationale for the ''T1'' definition in CRC is that no lymphatics are present in the mucosa, ergo no risk of distant spread.
| |
| *T2 - into muscularis propria.
| |
| *T3 - into fat beyond musclaris propria.
| |
| *T4 - into something else.
| |
|
| |
| Nodes:
| |
| *N0 - no positive nodes.
| |
| *N1 - 1-3 positive nodes.
| |
| *N2 - 4+ positive nodes.
| |
|
| |
| Notes:
| |
| *Memory device for N2 = 4+ +ve LNs: the number ''four'' in chinese sounds like ''death''.<ref>URL: [http://en.wikipedia.org/wiki/Numbers_in_Chinese_culture#Four http://en.wikipedia.org/wiki/Numbers_in_Chinese_culture#Four]. Accessed on: 28 June 2011.</ref>
| |
|
| |
|
| ==Staging of colorectal cancer== | | ==Staging of colorectal cancer== |
| ===Simple version===
| | {{Main|Colorectal cancer staging}} |
| Tumour/node grade for stage:<ref>{{Ref TN2006| GS27}}</ref>
| |
| *Stage I - '''T1 or T2''' N0 M0.
| |
| *Stage II - '''T3 or T4''' N0 M0.
| |
| *Stage III - Tx '''N1 or N2''' M0.
| |
| *Stage IV - Tx Nx '''M1'''.
| |
| | |
| ===Complex version===
| |
| Detailed tumour/node grade for stage:<ref>[http://www.cancer.org/docroot/CRI/content/CRI_2_4_3X_How_is_colon_and_rectum_cancer_staged.asp http://www.cancer.org/docroot/CRI/content/CRI_2_4_3X_How_is_colon_and_rectum_cancer_staged.asp]</ref>
| |
| *Stage I - T1 or T2.
| |
| *Stage IIA - T3.
| |
| *Stage IIB - T4.
| |
| *Stage IIIA - T1 N1 or T2 N1.
| |
| *Stage IIIB - T3 N1 or T4 N1.
| |
| *Stage IIIC - Tx N2.
| |
| *Stage IV - Tx Nx M1.
| |
|
| |
|
| ==Pathogenesis of colorectal carcinoma== | | ==Pathogenesis of colorectal carcinoma== |
| Line 84: |
Line 51: |
|
| |
|
| ====Mismatch repair pathway==== | | ====Mismatch repair pathway==== |
| *Associated with microsatellite instability (MSI). | | *Associated with [[microsatellite instability]] (MSI). |
| *Common associated gene mutations:
| |
| *#MLH1.
| |
| *#PMS2.
| |
| *#MSH2.
| |
| *#MSH6.
| |
| *Less common gene mutations:
| |
| *#PMS1.
| |
| *#MLH3.
| |
| *#MSH3.
| |
| | |
| =====IHC interpretation=====
| |
| *Loss of nuclear staining in nuclei of the tumour = mutation.
| |
| **Nuclear staining = normal.
| |
| | |
| MSI staining loss patterns:<ref name=pmid20632815/>
| |
| *MLH1 and PMS2 are often lost together, as MLH1 loss results in PMS2 loss.
| |
| *MSH2 and MSH6 are often lost together, as MSH2 loss results in MSH6 loss.
| |
| | |
| Implication of MSI staining loss patterns:
| |
| *PMS2 & MSH6 can be used as a screen.<ref name=pmid20632815>{{Cite journal | last1 = Hall | first1 = G. | last2 = Clarkson | first2 = A. | last3 = Shi | first3 = A. | last4 = Langford | first4 = E. | last5 = Leung | first5 = H. | last6 = Eckstein | first6 = RP. | last7 = Gill | first7 = AJ. | title = Immunohistochemistry for PMS2 and MSH6 alone can replace a four antibody panel for mismatch repair deficiency screening in colorectal adenocarcinoma. | journal = Pathology | volume = 42 | issue = 5 | pages = 409-13 | month = | year = 2010 | doi = 10.3109/00313025.2010.493871 | PMID = 20632815 }}</ref>
| |
| | |
| ======Etiology/significance loss of staining======
| |
| *MSH2 mutations (IHC stain -ve) - often associated with a germline mutation,<ref name=pmid16216036>{{cite journal |author=Mangold E, Pagenstecher C, Friedl W, ''et al.'' |title=Tumours from MSH2 mutation carriers show loss of MSH2 expression but many tumours from MLH1 mutation carriers exhibit weak positive MLH1 staining |journal=J. Pathol. |volume=207 |issue=4 |pages=385–95 |year=2005 |month=December |pmid=16216036 |doi=10.1002/path.1858 |url=}}</ref> while mutations in MLH1 are usually sporatic.<ref>A. Pollett. 2010.</ref>
| |
| *PMS2 mutations (IHC stain -ve) - often associated with a germline mutation.<ref name=pmid20205264>{{cite journal |author=Vaughn CP, Robles J, Swensen JJ, ''et al.'' |title=Clinical analysis of PMS2: mutation detection and avoidance of pseudogenes |journal=Hum. Mutat. |volume=31 |issue=5 |pages=588–93 |year=2010 |month=May |pmid=20205264 |doi=10.1002/humu.21230 |url=}}</ref>
| |
| | |
| | |
| How to remember the more important MSI stuff:
| |
| *The ''MSHs'' are paired together.
| |
| **''MSH'' (Mount Sinai Hospital) is where they started it in the city.
| |
| **''PMS'' sucks... it's with the other one (MLH).
| |
| *The higher numbers in the pairings ('''P'''MS2, '''M'''SH6) are the screening tests ('''''H'''igh Screen '''P'''ass'').
| |
| *The ''2''s (MSH2, PMS2) are associated with germline mutations (''Four legs good two legs bad!'').
| |
|
| |
|
| ===Other ancillary studies=== | | ===Other ancillary studies=== |
| *BRAF ''V600E'' missense mutation found in ~10% CRC.<ref name=pmid20635392>{{cite journal |author=Tie J, Gibbs P, Lipton L, ''et al.'' |title=Optimizing targeted therapeutic development: Analysis of a colorectal cancer patient population with the BRAF(V600E) mutation |journal=Int J Cancer |volume= |issue= |pages= |year=2010 |month=July |pmid=20635392 |doi=10.1002/ijc.25555 |url=}}</ref> | | *BRAF ''V600E'' missense mutation found in ~10% CRC.<ref name=pmid20635392>{{cite journal |author=Tie J, Gibbs P, Lipton L, ''et al.'' |title=Optimizing targeted therapeutic development: Analysis of a colorectal cancer patient population with the BRAF(V600E) mutation |journal=Int J Cancer |volume= |issue= |pages= |year=2010 |month=July |pmid=20635392 |doi=10.1002/ijc.25555 |url=}}</ref> |
| *KRAS mutation status. | | *[[KRAS mutation]] status. |
|
| |
|
| ====BRAF V600E mutation==== | | ====BRAF V600E mutation==== |
| | {{Main|BRAF V600E mutation}} |
| Features:<ref name=pmid20635392/> | | Features:<ref name=pmid20635392/> |
| *Independently associated with BRAF V600E: | | *Independently associated with BRAF V600E: |
| Line 131: |
Line 67: |
|
| |
|
| ====KRAS mutation==== | | ====KRAS mutation==== |
| | {{Main|KRAS mutation}} |
| Features:<ref name=pmid20956938>{{cite journal |author=Dunn EF, Iida M, Myers RA, ''et al.'' |title=Dasatinib sensitizes KRAS mutant colorectal tumors to cetuximab |journal=Oncogene |volume= |issue= |pages= |year=2010 |month=October |pmid=20956938 |doi=10.1038/onc.2010.430 |url=}}</ref><ref name=pmid19001320>{{cite journal |author=Di Nicolantonio F, Martini M, Molinari F, ''et al.'' |title=Wild-type BRAF is required for response to panitumumab or cetuximab in metastatic colorectal cancer |journal=J. Clin. Oncol. |volume=26 |issue=35 |pages=5705–12 |year=2008 |month=December |pmid=19001320 |doi=10.1200/JCO.2008.18.0786 |url=}}</ref> | | Features:<ref name=pmid20956938>{{cite journal |author=Dunn EF, Iida M, Myers RA, ''et al.'' |title=Dasatinib sensitizes KRAS mutant colorectal tumors to cetuximab |journal=Oncogene |volume= |issue= |pages= |year=2010 |month=October |pmid=20956938 |doi=10.1038/onc.2010.430 |url=}}</ref><ref name=pmid19001320>{{cite journal |author=Di Nicolantonio F, Martini M, Molinari F, ''et al.'' |title=Wild-type BRAF is required for response to panitumumab or cetuximab in metastatic colorectal cancer |journal=J. Clin. Oncol. |volume=26 |issue=35 |pages=5705–12 |year=2008 |month=December |pmid=19001320 |doi=10.1200/JCO.2008.18.0786 |url=}}</ref> |
| *Patient must have ''wild type'' KRAS to get drugs; KRAS mutation predicts resistance to [[cetuximab]] (Erbitux) and [[panitumumab]] (Vectibix). | | *Patient must have ''wild type'' KRAS to get drugs; KRAS mutation predicts resistance to [[cetuximab]] (Erbitux) and [[panitumumab]] (Vectibix). |
| **Cetuximab and panitumumab are [[EGFR inhibitors]]. | | **Cetuximab and panitumumab are [[EGFR inhibitors]]. |
|
| |
|
| ==MSI cancers== | | ==Microsatellite instability cancers== |
| ===General===
| | *Abbreviated ''MSI cancers''. |
| Features:<ref name=pmid20420947>{{cite journal |author=Boland CR, Goel A |title=Microsatellite instability in colorectal cancer |journal=Gastroenterology |volume=138 |issue=6 |pages=2073–2087.e3 |year=2010 |month=June |pmid=20420947 |doi=10.1053/j.gastro.2009.12.064 |url=}}</ref>
| | {{Main|Microsatellite instability in colorectal cancer}} |
| *Prognosis: slightly better than other CRC without MSI. | |
| *Treatment implication: different response to chemotherapy.
| |
| | |
| ====MSI classification====
| |
| MSI associated cancers can be classified into:<ref name=pmid16106253>{{cite journal |author=Lawes DA, Pearson T, Sengupta S, Boulos PB |title=The role of MLH1, MSH2 and MSH6 in the development of multiple colorectal cancers |journal=Br. J. Cancer |volume=93 |issue=4 |pages=472–7 |year=2005 |month=August |pmid=16106253 |pmc=2361590 |doi=10.1038/sj.bjc.6602708 |url=}}</ref><ref name=pmid11438476>{{cite journal |author=Guidoboni M, Gafà R, Viel A, ''et al.'' |title=Microsatellite instability and high content of activated cytotoxic lymphocytes identify colon cancer patients with a favorable prognosis |journal=Am. J. Pathol. |volume=159 |issue=1 |pages=297–304 |year=2001 |month=July |pmid=11438476 |pmc=1850401 |doi= |url=}}</ref>
| |
| *MSI-H >= 30% of loci have abnormality.
| |
| *MSI-L <30% of loci have abnormality.
| |
| | |
| Note:
| |
| *In the context of '''''no''''' chemotherapy, individuals with MSI-H tumours have a superior outcome to those with MSI-L tumours.<ref name=pmid12867608>{{Cite journal | last1 = Ribic | first1 = CM. | last2 = Sargent | first2 = DJ. | last3 = Moore | first3 = MJ. | last4 = Thibodeau | first4 = SN. | last5 = French | first5 = AJ. | last6 = Goldberg | first6 = RM. | last7 = Hamilton | first7 = SR. | last8 = Laurent-Puig | first8 = P. | last9 = Gryfe | first9 = R. | title = Tumor microsatellite-instability status as a predictor of benefit from fluorouracil-based adjuvant chemotherapy for colon cancer. | journal = N Engl J Med | volume = 349 | issue = 3 | pages = 247-57 | month = Jul | year = 2003 | doi = 10.1056/NEJMoa022289 | PMID = 12867608 }}</ref>
| |
| **With chemotherapy the outcomes are similar.
| |
| | |
| ===Gross===
| |
| Features:<ref name=pmid20420947>{{cite journal |author=Boland CR, Goel A |title=Microsatellite instability in colorectal cancer |journal=Gastroenterology |volume=138 |issue=6 |pages=2073–2087.e3 |year=2010 |month=June |pmid=20420947 |doi=10.1053/j.gastro.2009.12.064 |url=}}</ref>
| |
| *Location: proximal colon, i.e. right-sided, predominance.
| |
| | |
| ===Microscopic===
| |
| Features:<ref name=pmid20420947>{{cite journal |author=Boland CR, Goel A |title=Microsatellite instability in colorectal cancer |journal=Gastroenterology |volume=138 |issue=6 |pages=2073–2087.e3 |year=2010 |month=June |pmid=20420947 |doi=10.1053/j.gastro.2009.12.064 |url=}}</ref>
| |
| *Lymphocytic infiltrate - see ''[[intratumoural lymphocytic response]]''.
| |
| *Pushing border.<ref>Pollet, A. 18 October 2010.</ref>
| |
| *Histomorphology:
| |
| **Poorly differentiated.
| |
| **Mucinous.
| |
| **[[Signet ring cell carcinoma|Signet ring]].
| |
| **Medullary.<ref name=pmid18283560>{{cite journal |author=Truta B, Chen YY, Blanco AM, ''et al.'' |title=Tumor histology helps to identify Lynch syndrome among colorectal cancer patients |journal=Fam. Cancer |volume=7 |issue=3 |pages=267–74 |year=2008 |pmid=18283560 |doi=10.1007/s10689-008-9186-8 |url=}}</ref>
| |
|
| |
|
| =Specific entities= | | =Specific entities= |
| Line 168: |
Line 80: |
| *[[AKA]] ''colorectal adenocarcinoma not otherwise specified''. | | *[[AKA]] ''colorectal adenocarcinoma not otherwise specified''. |
| *[[AKA]] ''colorectal carcinoma'', abbreviated ''CRC''. | | *[[AKA]] ''colorectal carcinoma'', abbreviated ''CRC''. |
| | {{Main|Colorectal adenocarcinoma}} |
| | |
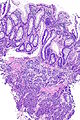
| | ==Secondary colorectal cancer== |
| ===General=== | | ===General=== |
| *Very common. | | *Uncommon. |
| *Rectum and sigmoid > proximal large bowel. | | *May be suspected. |
| | |
| Presentation:
| |
| *Bright red blood per rectum (BRBPR).
| |
| *Constipation.
| |
| *Symptoms of bowel obstruction - nausea, vomiting.
| |
| | |
| Pathogenesis - see ''[[Colorectal_tumours#Pathogenesis_of_colorectal_carcinoma|pathogenesis of colorectal carcinoma]]''.
| |
| | |
| ===Gross===
| |
| Often circumferential or near circumferential:
| |
| *These are referred to as "apple core lesion" ''or'' "napkin-ring" lesion.
| |
| | |
| Mucosa:
| |
| *Granular appearance.
| |
| *Raised (exophytic) ''or'' heaped edges with ulceration.
| |
| | |
| Note:
| |
| *''Total mesorectal excisions'' should be assessed for completeness.
| |
| *The (soft tissue) radial margins, as present in TMEs and right hemicolectomies, should be inked.<ref>URL: [http://www.cancercare.on.ca/common/pages/UserFile.aspx?fileId=13954 http://www.cancercare.on.ca/common/pages/UserFile.aspx?fileId=13954]. Accessed on: 6 February 2013. </ref><ref name=pmid15790712>{{Cite journal | last1 = Bateman | first1 = AC. | last2 = Carr | first2 = NJ. | last3 = Warren | first3 = BF. | title = The retroperitoneal surface in distal caecal and proximal ascending colon carcinoma: the Cinderella surgical margin? | journal = J Clin Pathol | volume = 58 | issue = 4 | pages = 426-8 | month = Apr | year = 2005 | doi = 10.1136/jcp.2004.019802 | PMID = 15790712 }}</ref>
| |
| | |
| ====Images====
| |
| <gallery>
| |
| Image:Colon_cancer.jpg | CRC - gross. (WC)
| |
| Image:Colon_cancer_2.jpg | CRC - gross. (WC)
| |
| </gallery>
| |
| <gallery>
| |
| Image:Rectum - anterior view.jpg | Rectum - anterior view. (WC)
| |
| Image:Rectum - lateral_view.jpg | Rectum - lateral view. (WC)
| |
| Image:Rectum - anterior and lateral - inked.jpg| Rectum - inked. (WC)
| |
| Image:Rectum - opened.jpg | Rectum - opened (WC)
| |
| </gallery>
| |
|
| |
|
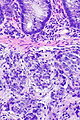
| ===Microscopic=== | | ===Microscopic=== |
| Features: | | Features: |
| *Nuclear atypia: | | *Normal colorectal mucosa. |
| **Nuclear pseudostratification.
| | *Atypical cells in the lamina propria or submucosa. |
| **Nuclear hyperchromasia. | | |
| **Chromatin clearing or granularity.
| | DDx: |
| *+/-Necrosis.
| | *Colorectal neuroendocrine tumour. |
| *Architecture - important for grading:
| |
| **Glands. | |
| **Sheets.
| |
|
| |
|
| ====Images====
| | ===Images=== |
| www:
| |
| *[http://www.flickr.com/photos/euthman/2480926690/in/set-72057594114099781 Colorectal adenocarcinoma (flickr.com/euthman)].
| |
| <gallery> | | <gallery> |
| Image:Adenocarcinoma_coli.jpg | Colorectal adenocarcinoma. (WC) | | Image:Prostate carcinoma in rectum -- very low mag.jpg | Pca in rectum - very low mag. (WC) |
| Image:Colonic_mucinous_adenocarcinoma_-_low_mag.jpg | Mucinous adenocarcinoma of the colon - low mag. (WC/Nephron) | | Image:Prostate carcinoma in rectum -- low mag.jpg | Pca in rectum - low mag. (WC) |
| | Image:Prostate carcinoma in rectum -- intermed mag.jpg | Pca in rectum - intermed. mag. (WC) |
| | Image:Prostate carcinoma in rectum -- high mag.jpg | Pca in rectum - high mag. (WC) |
| </gallery> | | </gallery> |
| ====Grading====
| |
| Based on component composed of glands:
| |
| *>=50% of tumour = low-grade (''well-differentiated'' and ''moderately differentiated'').
| |
| *<50% of tumour = high-grade (''poorly-differentiated'' and ''undifferentiated'').
| |
|
| |
| ====Peritumour lymphocytic response====
| |
| *[[AKA]] ''Crohn's-like lymphoid reaction''.
| |
| *[[AKA]] ''Crohn's like reaction''.<ref name=pmid19825961>{{Cite journal | last1 = Ogino | first1 = S. | last2 = Nosho | first2 = K. | last3 = Irahara | first3 = N. | last4 = Meyerhardt | first4 = JA. | last5 = Baba | first5 = Y. | last6 = Shima | first6 = K. | last7 = Glickman | first7 = JN. | last8 = Ferrone | first8 = CR. | last9 = Mino-Kenudson | first9 = M. | title = Lymphocytic reaction to colorectal cancer is associated with longer survival, independent of lymph node count, microsatellite instability, and CpG island methylator phenotype. | journal = Clin Cancer Res | volume = 15 | issue = 20 | pages = 6412-20 | month = Oct | year = 2009 | doi = 10.1158/1078-0432.CCR-09-1438 | PMID = 19825961 }}</ref>
| |
| *[[AKA]] ''Crohn-like repsonse''.<ref>URL: [http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2012/Colon_12protocol_3200.pdf http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2012/Colon_12protocol_3200.pdf]. Accessed on: 14 September 2012.</ref>
| |
|
| |
| =====General=====
| |
| *Finding associated with improved survival in CRC.<ref name=pmid7821914 >{{Cite journal | last1 = Harrison | first1 = JC. | last2 = Dean | first2 = PJ. | last3 = el-Zeky | first3 = F. | last4 = Vander Zwaag | first4 = R. | title = Impact of the Crohn's-like lymphoid reaction on staging of right-sided colon cancer: results of multivariate analysis. | journal = Hum Pathol | volume = 26 | issue = 1 | pages = 31-8 | month = Jan | year = 1995 | doi = | PMID = 7821914 }}</ref>
| |
|
| |
| =====Microscopic=====
| |
| [[Onlinepathology]] advocates use of the Ueno criteria. They have a better inter-rater reproducibility than the older Graham criteria<ref name=pmid2362940/> and are less complicated.
| |
|
| |
| ======Ueno criteria (2013)======
| |
| Required criteria:<ref name=pmid23525613>{{Cite journal | last1 = Ueno | first1 = H. | last2 = Hashiguchi | first2 = Y. | last3 = Shimazaki | first3 = H. | last4 = Shinto | first4 = E. | last5 = Kajiwara | first5 = Y. | last6 = Nakanishi | first6 = K. | last7 = Kato | first7 = K. | last8 = Maekawa | first8 = K. | last9 = Miyai | first9 = K. | title = Objective Criteria for Crohn-like Lymphoid Reaction in Colorectal Cancer. | journal = Am J Clin Pathol | volume = 139 | issue = 4 | pages = 434-41 | month = Apr | year = 2013 | doi = 10.1309/AJCPWHUEFTGBWKE4 | PMID = 23525613 }}</ref>
| |
| *Non-MALT lymphoid aggregates (peritumoural) >= 1 mm.
| |
|
| |
| Ignore:
| |
| #Muscosa-associated lymphoid tissue (MALT) = mucosal lymphoid aggregates, submucosal lymphoid aggregates adjacent to the musuclaris mucosae.
| |
| #Lymph nodes - these have a (fibrous) capsule.
| |
| #Irregular shape (not round).
| |
|
| |
| ======Graham criteria (1990)======
| |
| Required criteria:<ref name=pmid2362940>{{Cite journal | last1 = Graham | first1 = DM. | last2 = Appelman | first2 = HD. | title = Crohn's-like lymphoid reaction and colorectal carcinoma: a potential histologic prognosticator. | journal = Mod Pathol | volume = 3 | issue = 3 | pages = 332-5 | month = May | year = 1990 | doi = | PMID = 2362940 }}</ref>
| |
| *Peritumoral:
| |
| *#Lymphoid aggregates with germinal centres focally.
| |
| *#Stellate fibrosis.
| |
| *#No previous clinical and pathologic evidence of [[Crohn's disease]].
| |
|
| |
| Note:
| |
| *Should '''not''' be confused with [[intratumoural lymphocytic response]].
| |
| **The intratumoural lymphocytic response is associated with MSI-H cancers.
| |
|
| |
| Images:
| |
| *[http://jcp.bmjjournals.com/content/62/8/679/F2.large.jpg Peritumour lymphocytic response in endometrial carcinoma (bmjjournals.com)].
| |
| *[http://ajcp.ascpjournals.org/content/134/3/478/F3.expansion.html Peritumour lymphocytic response in CRC (ascpjournals.org)].<ref name=pmid20716806>{{Cite journal | last1 = Ross | first1 = JS. | last2 = Torres-Mora | first2 = J. | last3 = Wagle | first3 = N. | last4 = Jennings | first4 = TA. | last5 = Jones | first5 = DM. | title = Biomarker-based prediction of response to therapy for colorectal cancer: current perspective. | journal = Am J Clin Pathol | volume = 134 | issue = 3 | pages = 478-90 | month = Sep | year = 2010 | doi = 10.1309/AJCP2Y8KTDPOAORH | PMID = 20716806 | URL = http://ajcp.ascpjournals.org/content/134/3/478.full}}</ref>
| |
|
| |
| ====Intratumoural lymphocytic response====
| |
| *[[AKA]] '' tumour-infiltrating lymphocytes'', abbreviated ''TILs''.
| |
|
| |
| =====General=====
| |
| *Finding is suggestive of microsatellite instabillity.<ref name=pmid21114775>{{Cite journal | last1 = Iacopetta | first1 = B. | last2 = Grieu | first2 = F. | last3 = Amanuel | first3 = B. | title = Microsatellite instability in colorectal cancer. | journal = Asia Pac J Clin Oncol | volume = 6 | issue = 4 | pages = 260-9 | month = Dec | year = 2010 | doi = 10.1111/j.1743-7563.2010.01335.x | PMID = 21114775 }}</ref>
| |
| **May be seen in the context of [[Lynch syndrome]].
| |
|
| |
| =====Microscopic=====
| |
| Features:
| |
| *Lymphocytes are between the tumour cells.<ref name=pmid19638537/> †
| |
| **Other lymphocytes do not count.
| |
|
| |
| Note:
| |
| * † Definitions vary substantially - some authors consider lymphocytes adjacent to the tumour (in the stroma around the tumour cells) "intratumoural".<reF name=pmid9349235>{{Cite journal | last1 = Ropponen | first1 = KM. | last2 = Eskelinen | first2 = MJ. | last3 = Lipponen | first3 = PK. | last4 = Alhava | first4 = E. | last5 = Kosma | first5 = VM. | title = Prognostic value of tumour-infiltrating lymphocytes (TILs) in colorectal cancer. | journal = J Pathol | volume = 182 | issue = 3 | pages = 318-24 | month = Jul | year = 1997 | doi = 10.1002/(SICI)1096-9896(199707)182:3318::AID-PATH8623.0.CO;2-6 | PMID = 9349235 |URL = http://onlinelibrary.wiley.com/doi/10.1002/%28SICI%291096-9896%28199707%29182:3%3C318::AID-PATH862%3E3.0.CO;2-6/pdf}}</ref>
| |
|
| |
| ======Images======
| |
| <gallery> | | <gallery> |
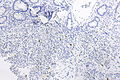
| Image:Tumour_infiltrating_lymphocytes_in_colorectal_carcinoma_-_high_mag.jpg | TILs - high mag. (WC/Nephron) | | Image:Prostate carcinoma in rectum - PSAP -- intermed mag.jpg | Pca in rectum - PSAP - intermed. mag. (WC) |
| Image:Tumour_infiltrating_lymphocytes_in_colorectal_carcinoma_-_very_high_mag.jpg | TILs - very high mag. (WC/Nephron) | | Image:Prostate carcinoma in rectum - PSA -- intermed mag.jpg | Pca in rectum - PSA - intermed. mag. (WC) |
| | Image:Prostate carcinoma in rectum - CK20 -- intermed mag.jpg | Pca in rectum - CK20 - intermed. mag. (WC) |
| </gallery> | | </gallery> |
| www:
| |
| *[http://jcp.bmjjournals.com/content/62/8/679/F3.large.jpg TILs in endometrial carcinoma (bmjjournals.com)].<ref name=pmid19638537>{{Cite journal | last1 = Garg | first1 = K. | last2 = Soslow | first2 = RA. | title = Lynch syndrome (hereditary non-polyposis colorectal cancer) and endometrial carcinoma. | journal = J Clin Pathol | volume = 62 | issue = 8 | pages = 679-84 | month = Aug | year = 2009 | doi = 10.1136/jcp.2009.064949 | PMID = 19638537 | URL = http://jcp.bmjjournals.com/content/62/8/679.full?related-urls=yes&legid=jclinpath;62/8/679 }}</ref>
| |
| *[http://ajcp.ascpjournals.org/content/134/3/478/F2.expansion.html TILs in CRC (ascpjournals.org)].<ref name=pmid20716806/>
| |
|
| |
| ===IHC===
| |
| *CK7 -ve.
| |
| *CK20 +ve.
| |
| *CEA +ve.
| |
| *CDX2 +ve.
| |
|
| |
| ===Molecular===
| |
| *KRAS mutation analysis.
| |
| **Mutation present ~ 40% of [[CRC]].
| |
| **Mutations in codons 12 or 13 associated with failure of anti-EGFR therapy (e.g. ''cetuximab'', ''panitumumab'').<ref name=pmid19792050>{{Cite journal | last1 = Monzon | first1 = FA. | last2 = Ogino | first2 = S. | last3 = Hammond | first3 = ME. | last4 = Halling | first4 = KC. | last5 = Bloom | first5 = KJ. | last6 = Nikiforova | first6 = MN. | title = The role of KRAS mutation testing in the management of patients with metastatic colorectal cancer. | journal = Arch Pathol Lab Med | volume = 133 | issue = 10 | pages = 1600-6 | month = Oct | year = 2009 | doi = 10.1043/1543-2165-133.10.1600 | PMID = 19792050 }}</ref>
| |
| *BRAF mutation analysis.
| |
| **''V600E'' missense mutation found in ~10% CRC.<ref name=pmid20635392>{{cite journal |author=Tie J, Gibbs P, Lipton L, ''et al.'' |title=Optimizing targeted therapeutic development: Analysis of a colorectal cancer patient population with the BRAF(V600E) mutation |journal=Int J Cancer |volume= |issue= |pages= |year=2010 |month=July |pmid=20635392 |doi=10.1002/ijc.25555 |url=}}</ref>
| |
|
| |
| Note:
| |
| *KRAS mutations and BRAF mutations are considered mutually exclusive as they occur in the same pathway.
| |
|
| |
|
| =See also= | | =See also= |
| Line 305: |
Line 112: |
| *[[Colon]]. | | *[[Colon]]. |
| *[[Gastrointestinal pathology]]. | | *[[Gastrointestinal pathology]]. |
| | *[[Tumour budding]]. |
| | *[[Tumour perforation in colorectal cancer]]. |
| | *[[Transanal minimally invasive surgery]]. |
|
| |
|
| =References= | | =References= |