Difference between revisions of "Atypical ductal hyperplasia"
Jump to navigation
Jump to search
(+cat.) |
|||
| (11 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
{{ Infobox diagnosis | |||
| Name = {{PAGENAME}} | |||
| Image = Atypical_ductal_hyperplasia_-_very_high_mag.jpg | |||
| Width = | |||
| Caption = Atypical ductal hyperplasia. [[H&E stain]]. (WC/Nephron) | |||
| Synonyms = | |||
| Micro = cytologic and architectural features of low-grade DCIS (equal cell spacing, lumina round, variable architecture (classically [[cribriform]] or solid - may be micropapillary or papillary), small nuclei, small indistinct nucleoli); limited extent - either (1) two or less complete ducts, (2) <2 mm in size | |||
| Subtypes = | |||
| LMDDx = [[ductal carcinoma in situ]], [[invasive ductal carcinoma of the breast]] | |||
| Stains = | |||
| IHC = | |||
| EM = | |||
| Molecular = | |||
| IF = | |||
| Gross = | |||
| Grossing = | |||
| Staging = | |||
| Site = [[breast]] - see ''[[non-invasive breast carcinoma]]'' | |||
| Assdx = | |||
| Syndromes = | |||
| Clinicalhx = | |||
| Signs = | |||
| Symptoms = none | |||
| Prevalence = relatively common | |||
| Bloodwork = | |||
| Rads = suspicious calcifications | |||
| Endoscopy = | |||
| Prognosis = benign, increased risk of malignancy | |||
| Other = | |||
| ClinDDx = | |||
| Tx = lumpectomy when found on biopsy, follow-up if on excisional specimen | |||
}} | |||
'''Atypical ductal hyperplasia''', abbreviated '''ADH''', is a benign [[breast pathology|breast lesion]] associated with an increased risk of [[malignancy]]. | |||
==General== | |||
*Molecular studies have shown it is the same thing as low-grade DCIS; thus, some have called for abolition of the term.<ref>{{Cite journal | last1 = Ghofrani | first1 = M. | last2 = Tapia | first2 = B. | last3 = Tavassoli | first3 = FA. | title = Discrepancies in the diagnosis of intraductal proliferative lesions of the breast and its management implications: results of a multinational survey. | journal = Virchows Arch | volume = 449 | issue = 6 | pages = 609-16 | month = Dec | year = 2006 | doi = 10.1007/s00428-006-0245-y | PMID = 17058097 }}</ref> | |||
*ADH is considered an indication for a lumpectomy.<ref name=pmid7717215>{{cite journal |author=Liberman L, Cohen MA, Dershaw DD, Abramson AF, Hann LE, Rosen PP |title=Atypical ductal hyperplasia diagnosed at stereotaxic core biopsy of breast lesions: an indication for surgical biopsy |journal=AJR Am J Roentgenol |volume=164 |issue=5 |pages=1111–3 |year=1995 |month=May |pmid=7717215 |doi= |url=http://www.ajronline.org/cgi/pmidlookup?view=long&pmid=7717215}}</ref> | |||
**Two large studies suggest the conversion of an ADH on core biopsy to breast cancer on surgical excision, known as "up-grading", is approximately 30%.<ref name=pmid20619647>{{Cite journal | last1 = Deshaies | first1 = I. | last2 = Provencher | first2 = L. | last3 = Jacob | first3 = S. | last4 = Côté | first4 = G. | last5 = Robert | first5 = J. | last6 = Desbiens | first6 = C. | last7 = Poirier | first7 = B. | last8 = Hogue | first8 = JC. | last9 = Vachon | first9 = E. | title = Factors associated with upgrading to malignancy at surgery of atypical ductal hyperplasia diagnosed on core biopsy. | journal = Breast | volume = 20 | issue = 1 | pages = 50-5 | month = Feb | year = 2011 | doi = 10.1016/j.breast.2010.06.004 | PMID = 20619647 }}</ref><ref name=pmid16978969>{{Cite journal | last1 = Margenthaler | first1 = JA. | last2 = Duke | first2 = D. | last3 = Monsees | first3 = BS. | last4 = Barton | first4 = PT. | last5 = Clark | first5 = C. | last6 = Dietz | first6 = JR. | title = Correlation between core biopsy and excisional biopsy in breast high-risk lesions. | journal = Am J Surg | volume = 192 | issue = 4 | pages = 534-7 | month = Oct | year = 2006 | doi = 10.1016/j.amjsurg.2006.06.003 | PMID = 16978969 }}</ref> | |||
Epidemiology: | |||
*Relative risk of breast cancer, based on a median follow-up of 8 years, in a case control study of US registered nurses, is 3.7.<ref name=pmid1734106>{{Cite journal | last1 = London | first1 = SJ. | last2 = Connolly | first2 = JL. | last3 = Schnitt | first3 = SJ. | last4 = Colditz | first4 = GA. | title = A prospective study of benign breast disease and the risk of breast cancer. | journal = JAMA | volume = 267 | issue = 7 | pages = 941-4 | month = Feb | year = 1992 | doi = | PMID = 1734106 }}</ref> | |||
==Microscopic== | |||
Features: | |||
*Cytologic and architectural features of low-grade DCIS. | |||
**Cell spacing ~ equal. | |||
**Lumina round. | |||
**Architecture - classically ''cribriform'' or ''solid''; may be ''micropapillary'' or ''papillary''. | |||
**Small nuclei. | |||
***Small indistinct nucleoli. | |||
*Limited extent ([[diagnostic size cutoffs]]) - either:<ref>{{Ref DCHH|258}}</ref> | |||
*#< Two complete ducts. | |||
*#< 2 mm. ‡ | |||
DDx: | |||
*Low-grade [[ductal carcinoma in situ]] (DCIS). | |||
*[[Florid epithelial hyperplasia of the usual type]] (FEHUT). | |||
Notes: | |||
*''High-grade DCIS'' is '''not''' in the [[DDx]] of ADH. | |||
* ‡ 3 mm is used in papillary lesions.{{fact}} | |||
===Images=== | |||
<gallery> | |||
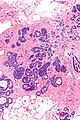
Image:Atypical_ductal_hyperplasia_-_very_low_mag.jpg|ADH. Very low mag. (WC/Nephron) | |||
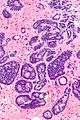
Image:Atypical_ductal_hyperplasia_-_low_mag.jpg|ADH - low mag. (WC/Nephron) | |||
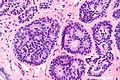
Image:Atypical_ductal_hyperplasia_-_intermed_mag.jpg|ADH - intermed. mag. (WC/Nephron) | |||
Image:Atypical_ductal_hyperplasia_-_high_mag.jpg|ADH - high mag. (WC/Nephron) | |||
Image:Atypical_ductal_hyperplasia_-_very_high_mag.jpg|ADH - very high mag. (WC/Nephron) | |||
</gallery> | |||
==IHC== | |||
*CK5 <20% +ve. | |||
*ER +ve - diffusely. | |||
**Heterogenous in [[FEHUT]]. | |||
==See also== | |||
*[[Non-invasive breast carcinoma]]. | |||
*[[Ductal carcinoma in situ]]. | |||
*[[Atypical lobular hyperplasia]]. | |||
==References== | |||
{{Reflist|1}} | |||
[[Category:Breast pathology]] | |||
[[Category:Diagnosis]] | [[Category:Diagnosis]] | ||
Latest revision as of 20:11, 30 April 2016
| Atypical ductal hyperplasia | |
|---|---|
| Diagnosis in short | |
 Atypical ductal hyperplasia. H&E stain. (WC/Nephron) | |
|
| |
| LM | cytologic and architectural features of low-grade DCIS (equal cell spacing, lumina round, variable architecture (classically cribriform or solid - may be micropapillary or papillary), small nuclei, small indistinct nucleoli); limited extent - either (1) two or less complete ducts, (2) <2 mm in size |
| LM DDx | ductal carcinoma in situ, invasive ductal carcinoma of the breast |
| Site | breast - see non-invasive breast carcinoma |
|
| |
| Symptoms | none |
| Prevalence | relatively common |
| Radiology | suspicious calcifications |
| Prognosis | benign, increased risk of malignancy |
| Treatment | lumpectomy when found on biopsy, follow-up if on excisional specimen |
Atypical ductal hyperplasia, abbreviated ADH, is a benign breast lesion associated with an increased risk of malignancy.
General
- Molecular studies have shown it is the same thing as low-grade DCIS; thus, some have called for abolition of the term.[1]
- ADH is considered an indication for a lumpectomy.[2]
Epidemiology:
- Relative risk of breast cancer, based on a median follow-up of 8 years, in a case control study of US registered nurses, is 3.7.[5]
Microscopic
Features:
- Cytologic and architectural features of low-grade DCIS.
- Cell spacing ~ equal.
- Lumina round.
- Architecture - classically cribriform or solid; may be micropapillary or papillary.
- Small nuclei.
- Small indistinct nucleoli.
- Limited extent (diagnostic size cutoffs) - either:[6]
- < Two complete ducts.
- < 2 mm. ‡
DDx:
- Low-grade ductal carcinoma in situ (DCIS).
- Florid epithelial hyperplasia of the usual type (FEHUT).
Notes:
- High-grade DCIS is not in the DDx of ADH.
- ‡ 3 mm is used in papillary lesions.[citation needed]
Images

ADH. Very low mag. (WC/Nephron)

ADH - low mag. (WC/Nephron)
ADH - intermed. mag. (WC/Nephron)
ADH - high mag. (WC/Nephron)
ADH - very high mag. (WC/Nephron)




IHC
- CK5 <20% +ve.
- ER +ve - diffusely.
- Heterogenous in FEHUT.
See also
References
- ↑ Ghofrani, M.; Tapia, B.; Tavassoli, FA. (Dec 2006). "Discrepancies in the diagnosis of intraductal proliferative lesions of the breast and its management implications: results of a multinational survey.". Virchows Arch 449 (6): 609-16. doi:10.1007/s00428-006-0245-y. PMID 17058097.
- ↑ Liberman L, Cohen MA, Dershaw DD, Abramson AF, Hann LE, Rosen PP (May 1995). "Atypical ductal hyperplasia diagnosed at stereotaxic core biopsy of breast lesions: an indication for surgical biopsy". AJR Am J Roentgenol 164 (5): 1111–3. PMID 7717215. http://www.ajronline.org/cgi/pmidlookup?view=long&pmid=7717215.
- ↑ Deshaies, I.; Provencher, L.; Jacob, S.; Côté, G.; Robert, J.; Desbiens, C.; Poirier, B.; Hogue, JC. et al. (Feb 2011). "Factors associated with upgrading to malignancy at surgery of atypical ductal hyperplasia diagnosed on core biopsy.". Breast 20 (1): 50-5. doi:10.1016/j.breast.2010.06.004. PMID 20619647.
- ↑ Margenthaler, JA.; Duke, D.; Monsees, BS.; Barton, PT.; Clark, C.; Dietz, JR. (Oct 2006). "Correlation between core biopsy and excisional biopsy in breast high-risk lesions.". Am J Surg 192 (4): 534-7. doi:10.1016/j.amjsurg.2006.06.003. PMID 16978969.
- ↑ London, SJ.; Connolly, JL.; Schnitt, SJ.; Colditz, GA. (Feb 1992). "A prospective study of benign breast disease and the risk of breast cancer.". JAMA 267 (7): 941-4. PMID 1734106.
- ↑ Tadrous, Paul.J. Diagnostic Criteria Handbook in Histopathology: A Surgical Pathology Vade Mecum (1st ed.). Wiley. pp. 258. ISBN 978-0470519035.