Hepatitis B
Hepatitis B is a relatively common medical liver disease caused by the hepatitis B virus.
| Hepatitis B | |
|---|---|
| Diagnosis in short | |
 Ground glass hepatocytes in chronic hepatitis B. H&E stain. | |
|
| |
| LM | lobular inflammation - hepatocyte necrosis, +/-ground glass hepatocytes |
| LM DDx | hepatitis C, autoimmune hepatitis, primary biliary cholangitis without granulomas, drug reaction |
| Stains | Shikata stain +ve (not sensitive) |
| IHC | hepatitis B +ve |
| Molecular | HBV DNA present (serum) |
| Site | liver - see medical liver disease |
|
| |
| Associated Dx | cirrhosis, hepatocellular carcinoma, polyarteritis nodosa (PAN), membranoproliferative glomerulonephritis, membranous nephropathy |
| Prevalence | common - especially in Asia |
| Blood work | HBs Ag, HBs Ab, HBe Ag, HBe Ab - see Medical_liver_disease#Hepatitis_B |
| Clin. DDx | other hepatitides - viral and non-viral |
| Treatment | prevention through vaccination, medical treatments (pegylated interferon and nucleoside analogues) |
General
- May lead to hepatocellular carcinoma without cirrhosis.
- High prevalence.
- Diagnosis is by serology - details of serologic testing are in the medical liver disease article.
- A vaccination is available and done routinely in a many jurisdictions.[1]
- Medical treatments available for chronic infection - pegylated interferon and nucleoside analogue therapies.[2][3]
Associated pathology
Microscopic
Features:
- Lobular inflammation - this is non-specific finding.
- Hepatocyte necrosis:
- Necrotic hepatocytes look a lot like neutrophils - however:
- Cytoplasm is more pink.
- Round apoptotic bodies.
- Necrotic hepatocytes look a lot like neutrophils - however:
- Hepatocyte necrosis:
- Ground glass hepatocytes - important.
DDx:
- Hepatitis C.
- Autoimmune hepatitis.
- Primary biliary cholangitis without granulomas.
- Drug reaction.
- Pseudo-Lafora bodies in patients on disulfiram (anatabuse) can result in ground glass hepatocytes.
Image
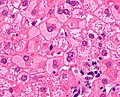
GGH - high mag. (WC)
HBV Modified HAI necroinflammatory score 5, Modified HAI fibrosis stage 2 HBV Modified HAI necroinflammatory score 5, Modified HAI fibrosis stage 2 HBV Modified HAI necroinflammatory score 5, Modified HAI fibrosis stage 2 HBV Modified HAI necroinflammatory score 5, Modified HAI fibrosis stage 2 HBV Modified HAI necroinflammatory score 5, Modified HAI fibrosis stage 2
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
42 yo woman with bepatitis B virus, modified HAI necroinflammatory grade 5, modified HAI fibrosis stage 1. (would be Metavir activity index 1, fibrosis stage 1). A Triads (red arrows) are slightly cellular, without much interface inflammation, with occasional spots suggestive of spotty necrosis (black arrows). B. Triads, this one being the most expanded, show a mild infiltrate (HAI score 1) of lymphocytes and macrophages, with only a small amount present at the interface between triad and lobule. C. A maximum of two foci of spotty necrosis (arrows) were seen in a 10X field (HAI score 2). D. Occasional foci of zone 3 collapse (thick black lines, green arrows), HAI score 1, and piecemeal necrosis (blue arrows) HAI score 1, were seen. E. Trichrome shows portal fibrosis of most triads, but no bridges, or nodules (HAI stage 2).
A. 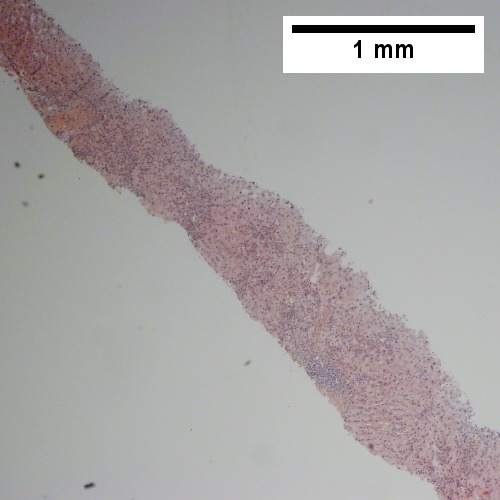 B.
B. 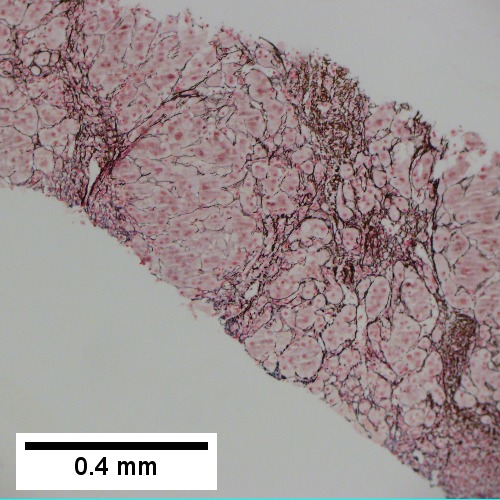
C. 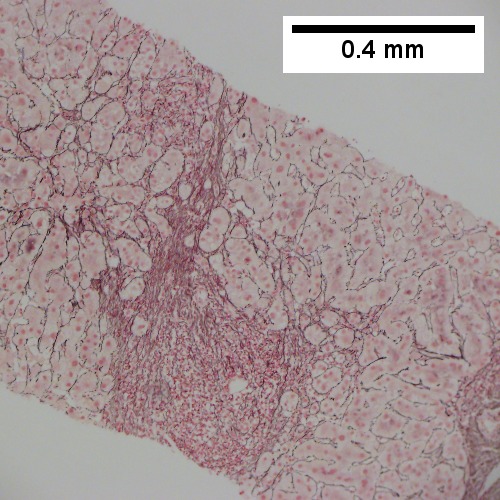 D.
D. 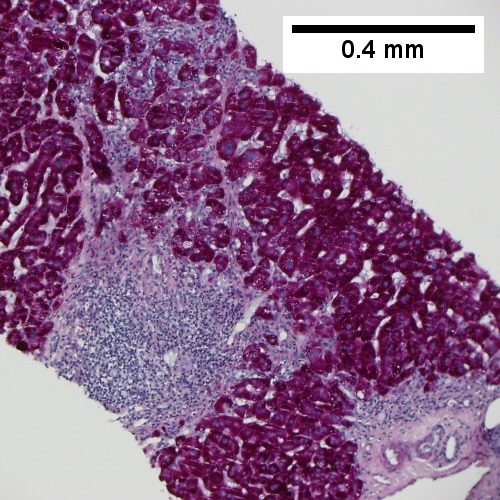
E. 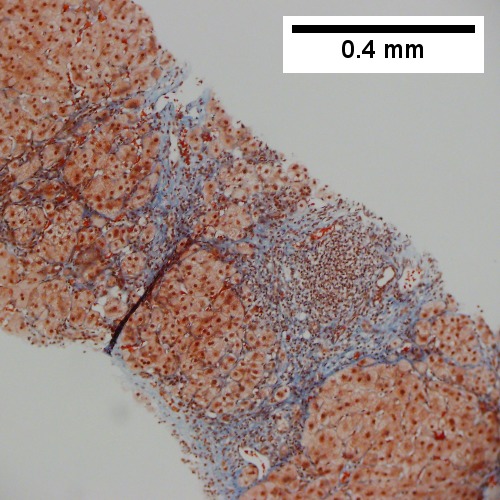 F.
F. 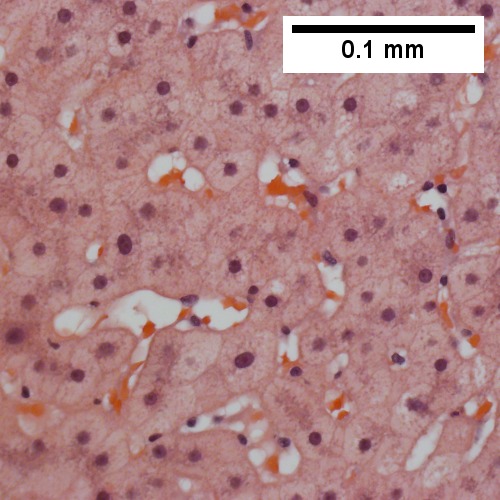
Hepatitis B. Metavir activity index 3. Piecemeal necrosis 2. Lobular necrosis 2. Fibrosis stage 3. A. Portal triads, expanded, inflamed and without sharp edges. Inflammation amid hepatocytes. B. Reticulin with bridging necrosis. C. Reticulin with extensive piecemeal necrosis. D. PAS without diastase with extensive piecemeal necrosis. E. Trichrome with bridging, no nodules or extensive bridging on slides as a whole. F. Ground glass hepatocytes.
A. Hepatitis B virus. Metavir activity index 3 {PMN 2 LN 2]. Metavir fibrosis stage 4 (advanced fibrosis/cirrhosis).
B. Hepatitis B virus. Metavir activity index 3 {PMN 2 LN 2]. Metavir fibrosis stage 4 (advanced fibrosis/cirrhosis).
C. Hepatitis B virus. Metavir activity index 3 {PMN 2 LN 2]. Metavir fibrosis stage 4 (advanced fibrosis/cirrhosis).
D. Hepatitis B virus. Metavir activity index 3 {PMN 2 LN 2]. Metavir fibrosis stage 4 (advanced fibrosis/cirrhosis).
E. Hepatitis B virus. Metavir activity index 3 {PMN 2 LN 2]. Metavir fibrosis stage 4 (advanced fibrosis/cirrhosis).
F. Hepatitis B virus. Metavir activity index 3 {PMN 2 LN 2]. Metavir fibrosis stage 4 (advanced fibrosis/cirrhosis).
Hepatitis B virus. Metavir activity index 3 {PMN 2 LN 2]. Metavir fibrosis stage 4 (advanced fibrosis/cirrhosis). A. A fragmented specimen shows apparent nodules [black arrows]. B. Inflammatory cells extending from band suggest piecemeal necrosis [green arrows]; inflammatory foci apart from band denote spotty necrosis [blue arrows]. C. Reticulin stain shows piecemeal necrosis as black lines about hepatocyte clusters at band [blue arrows], regeneration as more than one cell thick cords [green arrows] and hepatocyte rosettes [magenta arrows]. D. On PAS without diastase, piecemeal necrosis can be seen as pink hepatocyte cytoplasmic fragments amid inflammatory cells [arrows]. E. The nodules seen at low power are confirmed to be collagen bounded, but the appreciation can be made frustrated by intense inflammation. F. Examination elsewhere shows a definite nodule pair amid fibrosis [green arrows]; note on the right the fibrous band extending from the portal triad [black arrow] with sinusoids being far more often perpendicular to the triad than they were in the regenerative nodules to the surrounding bands.
Stains
- Shikata stain - hepatitis B surface antigen.
- Sensitivity modest ~20% of serum positive stain positive.[4]
IHC
- Hepatitis B +ve.
See also
References
- ↑ Leuridan, E.; Van Damme, P. (Jul 2011). "Hepatitis B and the need for a booster dose.". Clin Infect Dis 53 (1): 68-75. doi:10.1093/cid/cir270. PMID 21653306.
- ↑ Su, TH.; Kao, JH. (Nov 2017). "Unmet Needs in Clinical and Basic Hepatitis B Virus Research.". J Infect Dis 216 (suppl_8): S750-S756. doi:10.1093/infdis/jix382. PMID 29156048.
- ↑ Chen, GF.; Wang, C.; Lau, G. (Jan 2017). "Treatment of chronic hepatitis B infection-2017.". Liver Int 37 Suppl 1: 59-66. doi:10.1111/liv.13309. PMID 28052634.
- ↑ Ghosh, AK.; Dasgupta, A.; Raha, K.; Jana, A.; Majumdar, DN. (Oct 1994). "Hepatic histology in chronic liver disease in hepatitis B surface antigen positive cases.". J Indian Med Assoc 92 (10): 333-5. PMID 7822848.