Intraductal carcinoma of the prostate
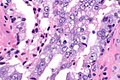
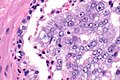
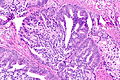
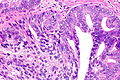
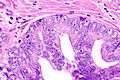
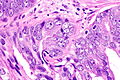
Intraductal carcinoma of the prostate, abbreviated IDC-P, is a proliferation of malignant prostate cells within glands that have an intact basal cell layer.
| Intraductal carcinoma of the prostate | |
|---|---|
| Diagnosis in short | |
 Intraductal carcinoma of prostate. H&E stain. | |
|
| |
| LM | major criteria : glands 2x normal (peripheral zone) glands, basal cells present, "cytologically malignant cells" (nuclear hyperchromasia, nuclear enlargement, nucleoli), fills the lumen ("expansile") but does not have to be "solid", +/-comedonecrosis; minor criteria : branching of ducts at right angles, rounded/smooth gland outlines, two cell populations (malignant appearing at periphery of gland, benign appearing - centre of gland) |
| LM DDx | invasive prostatic carcinoma, high grade prostatic intraepithelial neoplasia |
| IHC | basal cells are present (CK34betaE12 +ve, p63 +ve) |
| Site | prostate gland |
|
| |
| Prevalence | uncommon |
| Blood work | PSA typically elevated |
| Prognosis | poor, strongly suggestive invasion if not present |
It should not be confused with ductal adenocarcinoma of the prostate gland.
General
- May represent a precursor to invasive prostate carcinoma.[1]
- Associated with a poor prognosis.[2]
- Strong association with aggressive invasive carcinomas on prostatectomy when identified in isolation on biopsy.[3]
- High interobserver variability among experts ~43% agreement.[4]
- For comparison: HGPIN ~70% agreement, invasive carcinoma ~73% agreement.
- Uncommon finding ~ 3% of cases in a series of 1176 prostate biopsies.[5]
Microscopic
Epstein criteria
Epstein's IDCP criteria:[6]
- "Large" acini or ducts with basal cells and one of the following:
- Solid growth pattern or "dense" cribriform pattern.
- Micropapillary pattern or "loose" cribriform pattern with one of the following:
- Marked atypia 6x normal (area).‡
- Non-focal comedonecrosis.
Notes:
- ‡ Epstein's paper does not explicitly state that it is the area; however, there is near consensus in an ENUP survey that this is the case.[7] The equivalent diameter multiplier is sqrt(6) ~ 2.45; 6x area ~= 2.45x diameter.
Zhou criteria
Major criteria
Required major criteria:[8][9]
- Glands 2x normal (peripheral zone) glands.
- Basal cells present (proven by IHC).
- "Cytologically malignant cells" = nuclear hyperchromasia, nuclear enlargement, nucleoli.
- Fills the lumen ("expansile") but does not have to be "solid".
- Solid = no spaces between the cells.
Additional (major) criterion:[8]
- Comedonecrosis.
Minor criteria
Minor criteria:[8]
- Branching of ducts at right angles.
- Rounded/smooth gland outlines.
- Two cell populations:
- Malignant population (enlarged nuclei with hyperchromasia and nucleoli) = peripheral location in gland.
- Benign population (smaller nuclei, no nucleoli) = central location in gland.
DDx
- High-grade prostatic intraepithelial neoplasia (HGPIN).
- Invasive prostate adenocarcinoma.
Images
Case 1
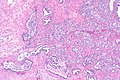
IDCP - low mag.
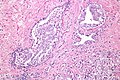
IDCP - intermed. mag.
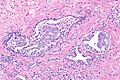
IDCP - intermed. mag.
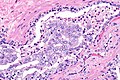
IDCP - high mag.
IDCP - very high mag.
IDCP - very high mag.





Case 2
IDCP - intermed. mag.
IDCP - high mag.
IDCP - very high mag.
IDCP - very high mag.




IHC
Features - basal cells present:
- CK34betaE12 +ve.
- p63 +ve.
See also
References
- ↑ Miyai, K.; Divatia, MK.; Shen, SS.; Miles, BJ.; Ayala, AG.; Ro, JY. (2014). "Heterogeneous clinicopathological features of intraductal carcinoma of the prostate: a comparison between "precursor-like" and "regular type" lesions.". Int J Clin Exp Pathol 7 (5): 2518-26. PMID 24966964.
- ↑ Henry, PC.; Evans, AJ. (Jul 2009). "Intraductal carcinoma of the prostate: a distinct histopathological entity with important prognostic implications.". J Clin Pathol 62 (7): 579-83. doi:10.1136/jcp.2009.065003. PMID 19246509.
- ↑ Robinson, BD.; Epstein, JI. (Oct 2010). "Intraductal carcinoma of the prostate without invasive carcinoma on needle biopsy: emphasis on radical prostatectomy findings.". J Urol 184 (4): 1328-33. doi:10.1016/j.juro.2010.06.017. PMID 20723921.
- ↑ Iczkowski, KA.; Egevad, L.; Ma, J.; Harding-Jackson, N.; Algaba, F.; Billis, A.; Camparo, P.; Cheng, L. et al. (Dec 2014). "Intraductal carcinoma of the prostate: interobserver reproducibility survey of 39 urologic pathologists.". Ann Diagn Pathol 18 (6): 333-42. doi:10.1016/j.anndiagpath.2014.08.010. PMID 25263387.
- ↑ Watts, K.; Li, J.; Magi-Galluzzi, C.; Zhou, M. (Oct 2013). "Incidence and clinicopathological characteristics of intraductal carcinoma detected in prostate biopsies: a prospective cohort study.". Histopathology 63 (4): 574-9. doi:10.1111/his.12198. PMID 23931616.
- ↑ Guo, CC.; Epstein, JI. (Dec 2006). "Intraductal carcinoma of the prostate on needle biopsy: Histologic features and clinical significance.". Mod Pathol 19 (12): 1528-35. doi:10.1038/modpathol.3800702. PMID 16980940.
- ↑ Varma M, Egevad L, Berney D, Bubendorf L, Compérat EM, Hes O, van Leenders G, Kristiansen G, Intraductal Carcinoma of the Prostate (IDCP) Reporting Practice: A Survey of Practicing Pathologists. United States and Canadian Academy of Pathology Annual Meeting 2018. Available at: https://www.xcdsystem.com/uscap/program/2018/index.cfm?pgid=1&qfixed=1&SessionType=Platform%20Presentation.
- ↑ 8.0 8.1 8.2 Shah, RB.; Zhou, M. (Jul 2012). "Atypical cribriform lesions of the prostate: clinical significance, differential diagnosis and current concept of intraductal carcinoma of the prostate.". Adv Anat Pathol 19 (4): 270-8. doi:10.1097/PAP.0b013e31825c6c0e. PMID 22692290.
- ↑ Cohen, RJ.; Wheeler, TM.; Bonkhoff, H.; Rubin, MA. (Jul 2007). "A proposal on the identification, histologic reporting, and implications of intraductal prostatic carcinoma.". Arch Pathol Lab Med 131 (7): 1103-9. doi:10.1043/1543-2165(2007)131[1103:APOTIH]2.0.CO;2. PMID 17616999.