Gallbladder
The gallbladder, in pathology (and general surgery), is a growth industry... due to the worsening obesity epidemic.
Normal
Anatomy
- Body.
- Fundus.
- Neck.
Variations:
- Hartmann's pouch - invagination of the gallbladder wall at the origin of the cystic duct.
Image:
Histology
- No muscularis mucosae.
- Small amount of lymphocytes in the lamina propria.
Note:
- As there is no muscularis mucosae, the cancer staging is different; pT1a is lamina propria invasion. pT1b is muscle layer invasion.
Image

Normal gallbladder - intermed. mag. (WC/Nephron)

Overview
Most common:
- Cholelithiasis with cholecystitis.
Common:
- Antral-type metaplasia.
Uncommon:
- Intestinal metaplasia.
- Gallbladder dysplasia.
- Gallbladder carcinoma.
Common
Chronic cholecystitis
Acute cholecystitis
Gallbladder cholesterolosis
Cholelithiasis
- AKA gallstones.
General
- Often accompanies cholecystitis/contributes and/or causes cholecystitis.
- The gallbladder is removed following biliary pancreatitis (gallstone pancreatitis) to reduce recurrence risk.[2][3]
- Gallstones may compress the common bile duct - known as Mirizzi Syndrome.[4]
- Can be associated with jaundice.[5]
The two types of gallstones:
- Cholesterol stones.
- Pigment stones.
Note:
- Most stones technically speaking are a mix, i.e. cholesterol and pigment. Many call yellow stones that are a mix "cholesterol stones".
Epidemiology
Classic risk factors for gallstones - 4 Fs:[6]
- Female.
- Fat.
- Forty.
- Fertile.
Additional:
- Family history.
Cholesterol stones
- More common than pigment stone.
Appearance:
- Clear or yellow.
- Opaque or translucent.
- Sometimes shinny.
Image

Yellow gallstones. (WC)

Pigment stones
- Due to high RBC turnover, e.g. sickle cell disease, thalassemia.
- Radio-opaque.[7]
Appearance:
- Black - key feature.
- Dull.
Microscopic
- Not routinely done on gallstones.
Sign out
GALLBLADDER CHOLECYSTECTOMY: - CHOLELITHIASIS. - MILD CHRONIC CHOLECYSTITIS.
Less common pathologic diagnoses
Adenomyoma of the gallbladder
General
- Glands in muscle.
- Analogous to what happens in the uterus.
- Significance - may mimic malignant tumours of the gallbladder.[8][9]
- Uncommon.
Gross
- Cystic spaces (Rokitansky-Aschoff sinuses) - may be seen on imaging.[10][11]
- Gallbladder wall thickening.
Microscopic
Features:[12]
- Glands in muscularis propria of the gallbladder wall - key feature.
- Significant muscular hypertrophy - key feature.
- No nuclear atypia.
DDx:
- Gallbladder carcinoma.
- Chronic cholecystitis - has less muscular hypertrophy; overlaps with this diagnosis.[12]
- Phrygian cap.[13]
Image
Sign out
GALLBLADDER, CHOLECYSTECTOMY: - CHRONIC CHOLECYSTITIS WITH MILD CHOLESTEROLOSIS AND ADENOMYOSIS (FUNDUS). - CHOLELITHIASIS.
Gallbladder polyps
General
- Polyps are significant as they may be adenomatous, i.e. pre-cancerous.
- These are similar to polyps found elsewhere GI tract.
Microscopic
- See intestinal polyps.
Flat dysplasia:[14]
- Nuclear changes.
- Increased NC ratio.
- Hyperchromasia (essential).
- +/-Intestinal metaplasia --> goblet cells.
Gallbladder diverticulosis
General
- Uncommon.
- Thought to arise in the context of an outflow obstruction.[15]
Microscopic
Features:
- Mucosal pouch penetrating the muscularis propria of the gallbladder wall - key feature.
DDx:
Sign out
GALLBLADDER, CHOLECYSTECTOMY: - CHRONIC CHOLECYSTITIS WITH DIVERTICULOSIS. - CHOLELITHIASIS.
Xanthogranulomatous cholecystitis
- Abbreviated XGC.
Premalignant lesions
General
- Metaplasia associated with carcinoma.[16]
Hypothesis:[17]
- Antral type metaplasia --> intestinal metaplasia --> dysplasia --> carcinoma.
Intestinal metaplasia of the gallbladder
- AKA gallbladder intestinal metaplasia.
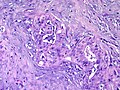
Antral type metaplasia
General
Microscopic
Features:[18]
- Columnar cells with:
- Abundant, pale, apical mucin.
- Small basal nucleus.
- Cells often in nests -- below luminal surface.
- Cells vaguely resemble foveollar epithelium of the stomach.
Notes:
- May look similar to cells of the gallbladder neck[18] and common bile duct.[19]
- These glandular cells are not as columnar and have less well-defined cell borders.
- Cells with antral type metaplasia >2:1 (height:width), benign mucosal glands <2:1.
- These glandular cells are not as columnar and have less well-defined cell borders.
Images:
Gallbladder adenoma
- Gallbladder dysplasia redirects here.
General
- Premalignant lesion.
- May be associated with familial adenomatous polyposis or Peutz-Jeghers syndrome.[20]
Microscopic
Features:
- Gallbladder epithelium with:
- Nuclear atypia - key feature.
- Nuclear hyperchromasia.
- Nuclear crowding (pseudostratification) or round enlarged nuclei.
- +/-Goblet cells.
- Nuclear atypia - key feature.
Architectural subclassification:[21]
- Papillary ~ 45%.
- Tubulopapillary ~ 30%.
- Tubular ~ 25%.
Notes:
- All of the gallbladder should be submitted prior to sign out to exclude non-sampled adenocarcinoma.
DDx:
- Gallbladder adenocarcinoma.
- Reactive changes.
Images
- Tubular adenoma, biliary type (rsna.org).[20]
- Gallbladder with high-grade dysplasia (flickr.com/lunar caustic).
Sign out
GALLBLADDER, CHOLECYSTECTOMY: - BILIARY TYPE TUBULAR ADENOMA WITH HIGH GRADE DYSPLASIA. - MARGINS CLEAR OF ADENOMA (NEAREST MARGIN 1.0 CM).
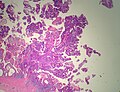
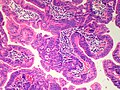
Intracholecystic Papillary Neoplasm[22]
General
- Probably some overlap with 'adenoma' above
- Lesion defined as being >1cm.
- Low-grade lesions previously designated “papillary adenoma”
- High-grade lesions previously designated “noninvasive papillary carcinoma.”
- Oten arise in a background of pyloric-gland metaplasia.
- May be associated with invasive adenocarcinoma, which should be reported as intracystic papillary neoplasm with an associated invasive carcinoma and staged.
- Population
- Female (F/M=2:1)
- Mean age 61
- Presentations
- Pain
- Incidental
- No particular association with gallstones.
Microscopic
- Cell types
- Pancreatobiliary type
- Intestinal types with goblet, Paneth, and/or serotonin-containing cells.
- Architecture
- Papillary
- Tubulopapillary
- Tubular
- Dysplasia - high or low grade
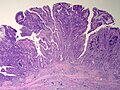
Gall Bladder - Intracholecystic Papillary Neoplasm with Invasive Adenocarcinoma - Low power (SKB)
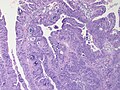
Gall Bladder - Intracholecystic Papillary Neoplasm with Invasive Adenocarcinoma - High power (SKB)
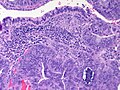
Gall Bladder - Intracholecystic Papillary Neoplasm with Invasive Adenocarcinoma - High power (SKB)
Gall Bladder - Intracholecystic Papillary Neoplasm with Invasive Adenocarcinoma - High power (SKB)
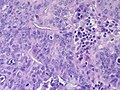
Gall Bladder - - Intracholecystic Papillary Neoplasm with Invasive Adenocarcinoma - Malignant gland infiltrating stroma - High power (SKB)
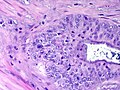
Gall Bladder - Intracholecystic Papillary Neoplasm with Invasive Adenocarcinoma - - Malignant gland infiltrating stroma - Very high power (SKB)
Gall Bladder - Intracholecystic Papillary Neoplasm with high grade dysplasia - Low power (SKB)
Gall Bladder - Intracholecystic Papillary Neoplasm with high grade dysplasia - Medium power (SKB)








{kind=link}
{kind=link}
Notes: All of the gallbladder should be submitted prior to sign out to exclude invasive adenocarcinoma.
Malignant
Gallbladder carcinoma
See also
References
- ↑ URL: http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2020_%20Extrahepatic%20Biliary%20Tract%20and%20Gallbladder.htm. Accessed on: 13 December 2012.
- ↑ Bouwense, SA.; Besselink, MG.; van Brunschot, S.; Bakker, OJ.; van Santvoort, HC.; Schepers, NJ.; Boermeester, MA.; Bollen, TL. et al. (2012). "Pancreatitis of biliary origin, optimal timing of cholecystectomy (PONCHO trial): study protocol for a randomized controlled trial.". Trials 13: 225. doi:10.1186/1745-6215-13-225. PMID 23181667.
- ↑ van Baal, MC.; Besselink, MG.; Bakker, OJ.; van Santvoort, HC.; Schaapherder, AF.; Nieuwenhuijs, VB.; Gooszen, HG.; van Ramshorst, B. et al. (May 2012). "Timing of cholecystectomy after mild biliary pancreatitis: a systematic review.". Ann Surg 255 (5): 860-6. doi:10.1097/SLA.0b013e3182507646. PMID 22470079.
- ↑ Khalid, S.; Bhatti, AA.. "Mirizzi's syndrome: an interesting on table finding.". J Ayub Med Coll Abbottabad 26 (4): 621-4. PMID 25672201.
- ↑ Elhanafy, E.; Atef, E.; El Nakeeb, A.; Hamdy, E.; Elhemaly, M.; Sultan, AM.. "Mirizzi Syndrome: How it could be a challenge.". Hepatogastroenterology 61 (133): 1182-6. PMID 25513064.
- ↑ Szwed, Z.; Zyciński, P. (2007). "[4F's--still up to date risk factors of cholelithiasis].". Wiad Lek 60 (11-12): 570-3. PMID 18540184.
- ↑ URL: http://www.rxmed.com/b.main/b2.pharmaceutical/b2.1.monographs/CPS-%20Monographs/CPS-%20%28General%20Monographs-%20U%29/URSOFALK.html. Accessed on: 29 October 2011.
- ↑ Saul, WM.; Herrmann, PK. (1988). "[Adenomyoma of the gallbladder].". Dtsch Z Verdau Stoffwechselkr 48 (2): 112-6. PMID 3168899.
- ↑ Sasatomi, E.; Miyazaki, K.; Mori, M.; Satoh, T.; Nakano, S.; Tokunaga, O. (Oct 1997). "Polypoid adenomyoma of the gallbladder.". J Gastroenterol 32 (5): 704-7. PMID 9350002.
- ↑ Ching, BH.; Yeh, BM.; Westphalen, AC.; Joe, BN.; Qayyum, A.; Coakley, FV. (Jul 2007). "CT differentiation of adenomyomatosis and gallbladder cancer.". AJR Am J Roentgenol 189 (1): 62-6. doi:10.2214/AJR.06.0866. PMID 17579153.
- ↑ 11.0 11.1 Boscak, AR.; Al-Hawary, M.; Ramsburgh, SR.. "Best cases from the AFIP: Adenomyomatosis of the gallbladder.". Radiographics 26 (3): 941-6. doi:10.1148/rg.263055180. PMID 16702464.
- ↑ 12.0 12.1 Iacobuzio-Donahue, Christine A.; Montgomery, Elizabeth A. (2005). Gastrointestinal and Liver Pathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 439. ISBN 978-0443066573.
- ↑ URL: http://radiopaedia.org/articles/phrygian_cap. Accessed on: 16 May 2014.
- ↑ Tadrous, Paul.J. Diagnostic Criteria Handbook in Histopathology: A Surgical Pathology Vade Mecum (1st ed.). Wiley. pp. 172. ISBN 978-0470519035.
- ↑ Beilby, JO. (Aug 1967). "Diverticulosis of the gall bladder. The fundal adenoma.". Br J Exp Pathol 48 (4): 455-61. PMC 2093791. PMID 4963758. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2093791/.
- ↑ Duarte I, Llanos O, Domke H, Harz C, Valdivieso V (September 1993). "Metaplasia and precursor lesions of gallbladder carcinoma. Frequency, distribution, and probability of detection in routine histologic samples". Cancer 72 (6): 1878–84. PMID 8364865.
- ↑ 17.0 17.1 Mukhopadhyay S, Landas SK (March 2005). "Putative precursors of gallbladder dysplasia: a review of 400 routinely resected specimens". Arch. Pathol. Lab. Med. 129 (3): 386–90. PMID 15737036. http://www.archivesofpathology.org/doi/pdf/10.1043/1543-2165%282005%29129%3C386%3APPOGDA%3E2.0.CO%3B2.
- ↑ 18.0 18.1 18.2 Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Oberman, Harold A; Reuter, Victor E (2004). Sternberg's Diagnostic Surgical Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 1789. ISBN 978-0781740517.
- ↑ Cutz, E. 3 March 2011.
- ↑ 20.0 20.1 Levy, AD.; Murakata, LA.; Abbott, RM.; Rohrmann, CA.. "From the archives of the AFIP. Benign tumors and tumorlike lesions of the gallbladder and extrahepatic bile ducts: radiologic-pathologic correlation. Armed Forces Institute of Pathology.". Radiographics 22 (2): 387-413. PMID 11896229. http://radiographics.rsna.org/content/22/2/387.full.
- ↑ Adsay, V.; Jang, KT.; Roa, JC.; Dursun, N.; Ohike, N.; Bagci, P.; Basturk, O.; Bandyopadhyay, S. et al. (Sep 2012). "Intracholecystic papillary-tubular neoplasms (ICPN) of the gallbladder (neoplastic polyps, adenomas, and papillary neoplasms that are ≥1.0 cm): clinicopathologic and immunohistochemical analysis of 123 cases.". Am J Surg Pathol 36 (9): 1279-301. doi:10.1097/PAS.0b013e318262787c. PMID 22895264.
- ↑ Adsay, V.; Jang, KT.; Roa, JC.; Dursun, N.; Ohike, N.; Bagci, P.; Basturk, O.; Bandyopadhyay, S. et al. (Sep 2012). "Intracholecystic papillary-tubular neoplasms (ICPN) of the gallbladder (neoplastic polyps, adenomas, and papillary neoplasms that are ≥1.0 cm): clinicopathologic and immunohistochemical analysis of 123 cases.". Am J Surg Pathol 36 (9): 1279-301. doi:10.1097/PAS.0b013e318262787c. PMID 22895264.