Germ cell tumours
This article covers germ cell tumours, often abbreviated GCT, which classically arise in the gonads (ovary, testis). They are also found in the midline and make appearances in neuropathology (e.g. pineal gland) and in the mediastinum.
Overview
Germ cell tumour - types
Precusor:
Germ cell tumours (GCTs):
- Germinoma/Seminoma/Dysgerminoma.
- Yolk sac tumour (endodermal sinus tumour).
- Embryonal carcinoma.
- Choriocarcinoma.
- Teratoma.
- Mixed germ cell tumour (mixed GCT) - 60% of GCTs are mixed.
- Common combinations:
- teratoma + embryonal carcinoma + endodermal sinus tumour (yolk sac tumour) (TEE).
- seminoma + embryonal (SE).
- embryonal + teratoma (TE).
- Common combinations:
- Gonadoblastoma.
- Polyembryoma.
Grossing
- 1 cm^2 of tumour per cm of maximal tumour dimension - guideline for testicular cancer.[1]
IHC for GCTs
ABCDs of GCTs:
- AFP - yolk sac tumour.
- Beta-hCG - choriocarcinoma.
- CD30 - embryonal carcinoma.
- D2-40 - seminoma.
Tabular summary of GCTs
| Tumour | Key feature | Microscopic | IHC | Other | Image |
|---|---|---|---|---|---|
| Intratubular germ cell neoplasia (ITGCN) | nests of small fried egg cells | large central nucleus, clear cytoplasm, squared-off nuclear membrane, nucleoli[2] |
CD117 | appearance similar to seminoma | |
| Germinoma / Seminoma / Dysgerminoma | fried egg cells | fried egg-like cells (central nucleus, clear cytoplasm) with squared-off nuclear membrane, nucleoli, lymphocytic infiltrate, granulomata, syncytiotrophoblastic giant cells[3] |
D2-40 | seminoma = male version of this tumour; dysgerminoma = female version of this tumour | |
| Yolk sac tumour (endodermal sinus tumour) | Schiller-Duval bodies | Schiller-Duval b. = central blood vessel surrounded by epithelial-like cells a space and more epithelial-like cells, variable arch. | AFP | patterns: microcystic, solid, hepatoid | |
| Embryonal carcinoma | prominent nucleoli, vescicular nuclei | var. arch.: tubulopapillary, glandular, solid, embryoid bodies (ball of cells in surrounded by empty space on three sides), +/-nuclear overlap, mitoses common | CD30 | usu. part of a mixed GCT | |
| Choriocarcinoma | clear cytoplasm | cells with abundant clear cytoplasm and eccentric atypical nuclei (cytotrophoblast), very large (multinucleated) cells with abundant eosinophilic cytoplasm and extreme nuclear atypia (syncytiotrophoblast) | beta-hCG | may be preceded by a complete hydatidiform mole | |
| Teratoma, immature | primitive neuroepithelium | pseudostratified epithelium in rosettes (gland-like arrangement) | None | testicular teratomas in post-pubertal males are all considered malignant[4] | |
| Mixed germ cell tumour | NA | common combinations: teratoma + embryonal carcinoma + endodermal sinus tumour (yolk sac tumour) (TEE); seminoma + embryonal (SE); embryonal + teratoma (TE) | NA | - | |
| Gonadoblastoma | primitive germ cells (central nucleus, moderate (eosinophilic) cytoplasm); sex cord element | sex cord element may be either granulosa cells (follicle-like arch.) or Sertoli cells (trabecular arch.) | ? | often abnormal karyotype; usu. Y chromosome present |








Molecular pathology
Most common cytogenetic abnormality in GCTs:
- Isochromosome p12.[5]
- Isochromosome = one arm (p or q) is lost and replaced with a duplicate of the remaining one.
- Example: isochromosome p12 = chromosome 12 where q is lost and two p arms are present.[6]
- Isochromosome = one arm (p or q) is lost and replaced with a duplicate of the remaining one.
Germinoma
Comes in three flavours:
- Germinoma.
- Seminoma.
- Dysgerminoma.
Germinoma
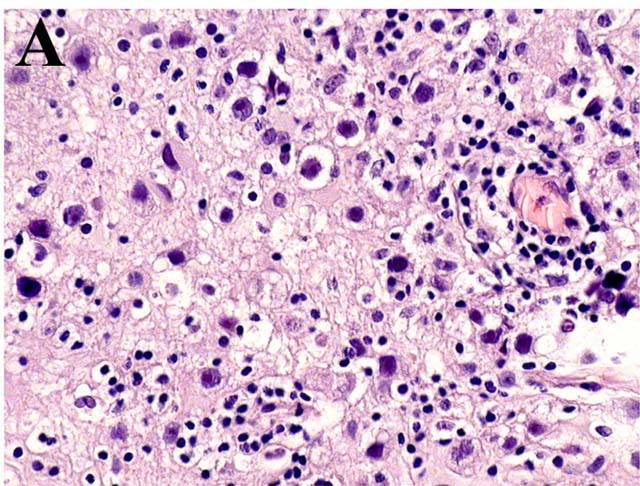
Is the generic version of this tumour. It is found in the midline (brain, mediastinum).
Image: Germinoma (upmc.edu).[7]
Seminoma
Main article: Seminoma
A common GCT in males.
Dysgerminoma
Main article: Ovarian tumours#Dysgerminoma
A common GCT in females.
Yolk sac tumour
Main article: Yolk sac tumour
Embryonal carcinoma
Main article: Embryonal carcinoma
Choriocarcinoma
Main article: Choriocarcinoma
Teratoma
Main article: Teratoma
Gonadoblastoma
Main article: Gonadoblastoma
Polyembryoma
General
- Poor prognosis.
- Almost never in pure form, i.e. usu. a component of a mixed germ cell tumour.[8]
Microscopic
Features:
- Disc shaped structure (embryo-like) with:
- The one side endoderm.
- Skin/CNS.
- The other side ectoderm.
- Internal organs - GI tract.
- The one side endoderm.
Images:
Mixed germ cell tumour
General
- 60% of GCTs are mixed.
Common combinations:
- Teratoma + embryonal carcinoma + endodermal sinus tumour (yolk sac tumour) (TEE).
- Seminoma + embryonal (SE).
- Teratoma + embryonal +(TE).
Memory device: TEE + all combinations have embryonal carcinoma.
Microscopic
Features:
- Depends on components.
Notes:
- If one cannot identify the component... it is probably yolk sac as this has so many different patterns.
Images
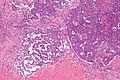
Mixed GCT - intermed mag. (WC/Nephron)
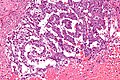
Mixed GCT - high mag. (WC/Nephron)

{kind=link}
www:
- Mixed germ cell tumour - several images (upmc.edu).
- Mixed germ cell tumour - several cases (upmc.edu).
IHC
- Beta-hCG +ve - if syncytiotrophoblasts are present.
- AFP +ve - a yolk sac tumour component is present.
- GFAP +ve - if neuroepithelium is present.
See also
References
- ↑ URL: http://www.uroweb.org/gls/pdf/10_Testicular_Cancer.pdf. Accessed on: 30 October 2012.
- ↑ Zhou, Ming; Magi-Galluzzi, Cristina (2006). Genitourinary Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 538. ISBN 978-0443066771.
- ↑ Zhou, Ming; Magi-Galluzzi, Cristina (2006). Genitourinary Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 542. ISBN 978-0443066771.
- ↑ Carver, BS.; Al-Ahmadie, H.; Sheinfeld, J. (May 2007). "Adult and pediatric testicular teratoma.". Urol Clin North Am 34 (2): 245-51; abstract x. doi:10.1016/j.ucl.2007.02.013. PMID 17484929.
- ↑ Looijenga, LH.; Oosterhuis, JW. (May 1999). "Pathogenesis of testicular germ cell tumours.". Rev Reprod 4 (2): 90-100. PMID 10357096.
- ↑ URL: http://ghr.nlm.nih.gov/handbook/illustrations/isochromosomes. Accessed on: 15 February 2012.
- ↑ URL: http://path.upmc.edu/cases/case525.html. Accessed on: 25 January 2012.
- ↑ Young, RH. (Apr 2008). "Testicular tumors--some new and a few perennial problems.". Arch Pathol Lab Med 132 (4): 548-64. doi:10.1043/1543-2165(2008)132[548:TTNAAF]2.0.CO;2. PMID 18384207.