Difference between revisions of "Desquamative interstitial pneumonia"
Jump to navigation
Jump to search
(chg. redirect +cat.) |
|||
| (20 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
{{ Infobox diagnosis | |||
| Name = {{PAGENAME}} | |||
| Image = Desquamative interstitial pneumonia -- intermed mag.jpg | |||
| Width = | |||
| Caption = Desquamative interstitial pneumonia. [[H&E stain]]. (WC/Nephron) | |||
| Synonyms = | |||
| Micro = abundant brown pigmented airspace macrophages (smoker's macrophages), architecture preserved ("linear fibrosis") | |||
| Subtypes = | |||
| LMDDx = amiodarone toxicity, fibrotic [[NSIP]], [[RBILD]] | |||
| Stains = | |||
| IHC = | |||
| EM = | |||
| Molecular = | |||
| IF = | |||
| Gross = | |||
| Grossing = | |||
| Staging = | |||
| Site = [[lung]] - see ''[[diffuse lung diseases]]'' | |||
| Assdx = +/-[[smoking]] | |||
| Syndromes = | |||
| Clinicalhx = | |||
| Signs = | |||
| Symptoms = | |||
| Prevalence = rare | |||
| Bloodwork = | |||
| Rads = ground glass airspaces changes - usu. all lobes but peripheral predominant and in lower lobe predominant | |||
| Endoscopy = | |||
| Prognosis = | |||
| Other = | |||
| ClinDDx = | |||
| Tx = stop smoking/remove insult | |||
}} | |||
'''Desquamative interstitial pneumonia''', abbreviated '''DIP''', is a [[diffuse lung diseases|diffuse lung disease]] that is strongly associated with [[smoking]]. | |||
The term ''desquamative interstitial pneumonia'' is a [[misnomer]]. The airspace cells that characterize the condition were once thought to represent desquamated epithelial cells, but they are now know to represent macrophages.<ref name=pmid18794314>{{Cite journal | last1 = Attili | first1 = AK. | last2 = Kazerooni | first2 = EA. | last3 = Gross | first3 = BH. | last4 = Flaherty | first4 = KR. | last5 = Myers | first5 = JL. | last6 = Martinez | first6 = FJ. | title = Smoking-related interstitial lung disease: radiologic-clinical-pathologic correlation. | journal = Radiographics | volume = 28 | issue = 5 | pages = 1383-96; discussion 1396-8 | month = | year = | doi = 10.1148/rg.285075223 | PMID = 18794314 | url=http://pubs.rsna.org/doi/full/10.1148/rg.285075223}}</ref> | |||
==General== | |||
*Rare.<ref name=pmid20854463/> | |||
*Strong association with smoking.<ref name=Ref_WMSP93>{{Ref WMSP|93}}</ref><ref name=pmid26324804>{{Cite journal | last1 = Margaritopoulos | first1 = GA. | last2 = Vasarmidi | first2 = E. | last3 = Jacob | first3 = J. | last4 = Wells | first4 = AU. | last5 = Antoniou | first5 = KM. | title = Smoking and interstitial lung diseases. | journal = Eur Respir Rev | volume = 24 | issue = 137 | pages = 428-35 | month = Sep | year = 2015 | doi = 10.1183/16000617.0050-2015 | PMID = 26324804 }}</ref> | |||
**Thought to be advanced ''[[RBILD]]''. | |||
*May be seen in non-smokers (up to ~40% of cases) due to occupational exposures, drugs, viral illnesses and autoimmune diseases.<ref name=pmid23728865>{{Cite journal | last1 = Godbert | first1 = B. | last2 = Wissler | first2 = MP. | last3 = Vignaud | first3 = JM. | title = Desquamative interstitial pneumonia: an analytic review with an emphasis on aetiology. | journal = Eur Respir Rev | volume = 22 | issue = 128 | pages = 117-23 | month = Jun | year = 2013 | doi = 10.1183/09059180.00005812 | PMID = 23728865 }}</ref> | |||
Diagnosis: | |||
*Requires - surgical biopsy.<ref name=pmid23728865/> | |||
Treatment: | |||
*Stop smoking/remove or manage underlying cause. | |||
==Gross/Radiology== | |||
Features:<ref name=pmid8497631>{{Cite journal | last1 = Hartman | first1 = TE. | last2 = Primack | first2 = SL. | last3 = Swensen | first3 = SJ. | last4 = Hansell | first4 = D. | last5 = McGuinness | first5 = G. | last6 = Müller | first6 = NL. | title = Desquamative interstitial pneumonia: thin-section CT findings in 22 patients. | journal = Radiology | volume = 187 | issue = 3 | pages = 787-90 | month = Jun | year = 1993 | doi = 10.1148/radiology.187.3.8497631 | PMID = 8497631 }}</ref> | |||
*Ground glass (airspace changes). | |||
**Usually peripheral predominant (~60% of cases) and lower lobe predominant (~70-75% of cases). | |||
**Typically all lobes are involved - though upper lobe spared in ~20% of cases. | |||
*Fibrotic (radiologic) changes ~50% of cases. | |||
==Microscopic== | |||
Features:<ref name=pmid20854463>{{Cite journal | last1 = Tazelaar | first1 = HD. | last2 = Wright | first2 = JL. | last3 = Churg | first3 = A. | title = Desquamative interstitial pneumonia. | journal = Histopathology | volume = 58 | issue = 4 | pages = 509-16 | month = Mar | year = 2011 | doi = 10.1111/j.1365-2559.2010.03649.x | PMID = 20854463 }}</ref> | |||
*Abundant airspace macrophages - usually with brown pigment (so called ''smoker's macrophages'') - '''key feature'''. | |||
*Interstitial inflammation ''or'' interstitial fibrosis with a preserved architecture - so called "linear fibrosis". | |||
Notes: | |||
*Some fields of view may be indistinguishable from [[RBILD]]. | |||
DDx: | |||
*Amiodarone toxicity. | |||
*Fibrotic [[NSIP]]. | |||
*[[RBILD]]. | |||
===Images=== | |||
<gallery> | |||
Image: Desquamative interstitial pneumonia -- low mag.jpg | DIP - low mag. | |||
Image: Desquamative interstitial pneumonia -- intermed mag.jpg | DIP - intermed. mag. | |||
Image: Desquamative interstitial pneumonia -- high mag.jpg | DIP - high mag. | |||
Image: Desquamative interstitial pneumonia -- very high mag.jpg | DIP - very high mag. | |||
Image: Desquamative interstitial pneumonia - alt -- low mag.jpg | DIP - low mag. | |||
Image: Desquamative interstitial pneumonia - alt -- intermed mag.jpg | DIP - intermed. mag. | |||
Image: Desquamative interstitial pneumonia - alt -- high mag.jpg | DIP - high mag. | |||
Image: Desquamative interstitial pneumonia - alt 2 -- intermed mag.jpg | DIP - intermed mag. | |||
</gallery> | |||
====www==== | |||
*[http://pathhsw5m54.ucsf.edu/case27/dip27.html DIP (ucsf.edu)]. | |||
==Stains== | |||
*Macrophages [[PAS stain|PAS]] +ve. | |||
==See also== | |||
*[[Diffuse lung diseases]]. | |||
*[[Smoking]]. | |||
*[[Smoking-related interstitial fibrosis]]. | |||
==References== | |||
{{Reflist|1}} | |||
[[Category:Diagnosis]] | [[Category:Diagnosis]] | ||
[[Category:Diffuse lung diseases]] | |||
Latest revision as of 14:57, 8 May 2019
Desquamative interstitial pneumonia, abbreviated DIP, is a diffuse lung disease that is strongly associated with smoking.
| Desquamative interstitial pneumonia | |
|---|---|
| Diagnosis in short | |
 Desquamative interstitial pneumonia. H&E stain. (WC/Nephron) | |
|
| |
| LM | abundant brown pigmented airspace macrophages (smoker's macrophages), architecture preserved ("linear fibrosis") |
| LM DDx | amiodarone toxicity, fibrotic NSIP, RBILD |
| Site | lung - see diffuse lung diseases |
|
| |
| Associated Dx | +/-smoking |
| Prevalence | rare |
| Radiology | ground glass airspaces changes - usu. all lobes but peripheral predominant and in lower lobe predominant |
| Treatment | stop smoking/remove insult |
The term desquamative interstitial pneumonia is a misnomer. The airspace cells that characterize the condition were once thought to represent desquamated epithelial cells, but they are now know to represent macrophages.[1]
General
- Rare.[2]
- Strong association with smoking.[3][4]
- Thought to be advanced RBILD.
- May be seen in non-smokers (up to ~40% of cases) due to occupational exposures, drugs, viral illnesses and autoimmune diseases.[5]
Diagnosis:
- Requires - surgical biopsy.[5]
Treatment:
- Stop smoking/remove or manage underlying cause.
Gross/Radiology
Features:[6]
- Ground glass (airspace changes).
- Usually peripheral predominant (~60% of cases) and lower lobe predominant (~70-75% of cases).
- Typically all lobes are involved - though upper lobe spared in ~20% of cases.
- Fibrotic (radiologic) changes ~50% of cases.
Microscopic
Features:[2]
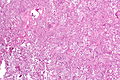
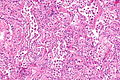
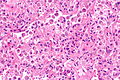
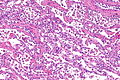
- Abundant airspace macrophages - usually with brown pigment (so called smoker's macrophages) - key feature.
- Interstitial inflammation or interstitial fibrosis with a preserved architecture - so called "linear fibrosis".
Notes:
- Some fields of view may be indistinguishable from RBILD.
DDx:
Images
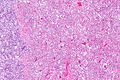
DIP - low mag.
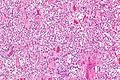
DIP - intermed. mag.
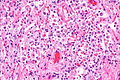
DIP - high mag.
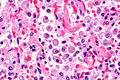
DIP - very high mag.
DIP - low mag.
DIP - intermed. mag.
DIP - high mag.
DIP - intermed mag.







www
Stains
- Macrophages PAS +ve.
See also
References
- ↑ Attili, AK.; Kazerooni, EA.; Gross, BH.; Flaherty, KR.; Myers, JL.; Martinez, FJ.. "Smoking-related interstitial lung disease: radiologic-clinical-pathologic correlation.". Radiographics 28 (5): 1383-96; discussion 1396-8. doi:10.1148/rg.285075223. PMID 18794314. http://pubs.rsna.org/doi/full/10.1148/rg.285075223.
- ↑ 2.0 2.1 Tazelaar, HD.; Wright, JL.; Churg, A. (Mar 2011). "Desquamative interstitial pneumonia.". Histopathology 58 (4): 509-16. doi:10.1111/j.1365-2559.2010.03649.x. PMID 20854463.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 93. ISBN 978-0781765275.
- ↑ Margaritopoulos, GA.; Vasarmidi, E.; Jacob, J.; Wells, AU.; Antoniou, KM. (Sep 2015). "Smoking and interstitial lung diseases.". Eur Respir Rev 24 (137): 428-35. doi:10.1183/16000617.0050-2015. PMID 26324804.
- ↑ 5.0 5.1 Godbert, B.; Wissler, MP.; Vignaud, JM. (Jun 2013). "Desquamative interstitial pneumonia: an analytic review with an emphasis on aetiology.". Eur Respir Rev 22 (128): 117-23. doi:10.1183/09059180.00005812. PMID 23728865.
- ↑ Hartman, TE.; Primack, SL.; Swensen, SJ.; Hansell, D.; McGuinness, G.; Müller, NL. (Jun 1993). "Desquamative interstitial pneumonia: thin-section CT findings in 22 patients.". Radiology 187 (3): 787-90. doi:10.1148/radiology.187.3.8497631. PMID 8497631.