Difference between revisions of "Uterine tubes"
m (→Microscopic) |
|||
| (38 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
[[Image:Normal Fallopian Tube, Human (2760475010).jpg|thumb|Cross section of a Fallopian tube with decidualization. [[H&E stain]]. (WC/euthman)]] | |||
'''Uterine tubes''', also known as the '''Fallopian tubes''', serve as a connection between the [[ovary|ovaries]] and the [[uterus]]. It is where fertilization usually takes place. | '''Uterine tubes''', also known as the '''Fallopian tubes''', serve as a connection between the [[ovary|ovaries]] and the [[uterus]]. It is where fertilization usually takes place. | ||
| Line 8: | Line 9: | ||
Cells: | Cells: | ||
#Ciliated | #Ciliated cell. | ||
#*Columnar. | #*Columnar. | ||
#*Eosinophilic cytoplasm. | #*Eosinophilic cytoplasm. | ||
#Peg | #Non-ciliated cell ([[AKA]] Peg cell). | ||
#*Nucleus more luminal. | #*Nucleus more luminal. | ||
#**Nuclei stick-out like a golf tee. | #**Nuclei stick-out like a golf tee. | ||
#Secretory cells. (???) | |||
#*Basal cells, fried egg-like. | |||
Images: | See also: | ||
*[[Walthard cell rest]]. | |||
===Images=== | |||
www: | |||
*[http://faculty.une.edu/com/abell/histo/ampovidw.jpg Fallopian tube (une.edu)].<ref>URL: [http://faculty.une.edu/com/abell/histo/histolab3f.htm http://faculty.une.edu/com/abell/histo/histolab3f.htm]. Accessed on: 18 October 2011.</ref> | *[http://faculty.une.edu/com/abell/histo/ampovidw.jpg Fallopian tube (une.edu)].<ref>URL: [http://faculty.une.edu/com/abell/histo/histolab3f.htm http://faculty.une.edu/com/abell/histo/histolab3f.htm]. Accessed on: 18 October 2011.</ref> | ||
*[http://medpics.ucsd.edu/index.cfm?curpage=image&course=hist&mode=browse&lesson=37&img=669 Fallopian tube (medpics.ucsd.edu)]. | *[http://medpics.ucsd.edu/index.cfm?curpage=image&course=hist&mode=browse&lesson=37&img=669 Fallopian tube (medpics.ucsd.edu)]. | ||
*[http://www.ouhsc.edu/histology/Glass%20slides/18_09.jpg Uterine tube - cells (ouhsc.edu)]. | |||
*[http://www.ouhsc.edu/histology/Glass%20slides/18_10.jpg Uterine tube - wall (ouhsc.edu)]. | |||
=Overview= | |||
===Benign lesions=== | |||
*[[Paratubal cyst]]. | |||
*[[Salpingitis isthmica nodosa]]. | |||
*[[Endometriosis]]. | |||
===Benign neoplasm=== | |||
*[[Adenomatoid tumour]]. | |||
===Pre-malignant=== | |||
*[[Serous tubal intraepithelial carcinoma]] (STIC). | |||
===Malignant diagnoses=== | |||
*Serous carcinoma. | |||
*Endometrioid adenocarcinoma.<ref name=pmid8946874>{{Cite journal | last1 = Navani | first1 = SS. | last2 = Alvarado-Cabrero | first2 = I. | last3 = Young | first3 = RH. | last4 = Scully | first4 = RE. | title = Endometrioid carcinoma of the fallopian tube: a clinicopathologic analysis of 26 cases. | journal = Gynecol Oncol | volume = 63 | issue = 3 | pages = 371-8 | month = Dec | year = 1996 | doi = 10.1006/gyno.1996.0338 | PMID = 8946874 }}</ref> | |||
= | =Ditzels= | ||
{{Main|Ditzels}} | {{Main|Ditzels}} | ||
==Paratubal cyst== | |||
*Also known as ''Hydatid cyst of Morgagni'' and ''Hydatid of Morgagni''. | |||
===General=== | |||
*Very common. | |||
*May lead to ovarian torsion if very large.<ref name=pmid22840942>{{Cite journal | last1 = Thakore | first1 = SS. | last2 = Chun | first2 = MJ. | last3 = Fitzpatrick | first3 = K. | title = Recurrent ovarian torsion due to paratubal cysts in an adolescent female. | journal = J Pediatr Adolesc Gynecol | volume = 25 | issue = 4 | pages = e85-7 | month = Aug | year = 2012 | doi = 10.1016/j.jpag.2011.10.012 | PMID = 22840942 }} | |||
</ref> | |||
*Associated with [[obesity]].<ref>{{Cite journal | last1 = Muolokwu | first1 = E. | last2 = Sanchez | first2 = J. | last3 = Bercaw | first3 = JL. | last4 = Sangi-Haghpeykar | first4 = H. | last5 = Banszek | first5 = T. | last6 = Brandt | first6 = ML. | last7 = Dietrich | first7 = JE. | title = Paratubal cysts, obesity, and hyperandrogenism. | journal = J Pediatr Surg | volume = 46 | issue = 11 | pages = 2164-7 | month = Nov | year = 2011 | doi = 10.1016/j.jpedsurg.2011.07.011 | PMID = 22075351 }}</ref> | |||
===Gross=== | |||
*Thin walled-cyst with serous fluid. | |||
===Microscopic=== | |||
Features: | |||
*Simple cyst with ciliated (tubal) epithelium. | |||
===Sign out=== | |||
<pre> | |||
PARATUBAL CYST, RIGHT, EXCISION: | |||
- BENIGN SIMPLE CYST. | |||
</pre> | |||
====No epithelium==== | |||
<pre> | |||
PARATUBAL CYST, LEFT, EXCISION: | |||
- BENIGN FIBROUS TISSUE COMPATIBLE WITH CYST WALL. | |||
</pre> | |||
==Tubal ligation== | ==Tubal ligation== | ||
*Abbreviated ''TL''. | |||
===General=== | ===General=== | ||
*Done to control fertility. | *Done to control fertility. | ||
| Line 32: | Line 85: | ||
*[[Serous carcinoma]] - nuclear atypia (marked), nuclear pleomorphism, prominent nucleoli. | *[[Serous carcinoma]] - nuclear atypia (marked), nuclear pleomorphism, prominent nucleoli. | ||
*[[Tubal intraepithelial carcinoma]] - discrete papillary growth, loss of nuclear polarity, nuclear atypia. | *[[Tubal intraepithelial carcinoma]] - discrete papillary growth, loss of nuclear polarity, nuclear atypia. | ||
*[[Endometriosis]]. | |||
===Sign out=== | ===Sign out=== | ||
====Left then right==== | |||
<pre> | |||
A. Fallopian Tube, Left, Tubal Ligation: | |||
- Fallopian tube within normal limits, consistent with complete cross sections. | |||
B. Fallopian Tube, Right, Tubal Ligation: | |||
- Fallopian tube within normal limits, consistent with complete cross sections. | |||
</pre> | |||
<pre> | |||
A. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: | |||
- FALLOPIAN TUBE WITHIN NORMAL LIMITS, CONSISTENT WITH COMPLETE CROSS SECTIONS. | |||
B. FALLOPIAN TUBE, RIGHT, TUBAL LIGATION: | |||
- FALLOPIAN TUBE WITHIN NORMAL LIMITS, CONSISTENT WITH COMPLETE CROSS SECTIONS. | |||
</pre> | |||
<pre> | <pre> | ||
A. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: | A. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: | ||
- FALLOPIAN TUBE WITHIN NORMAL LIMITS. | - FALLOPIAN TUBE WITHIN NORMAL LIMITS. | ||
B. FALLOPIAN TUBE, RIGHT, TUBAL LIGATION: | |||
- FALLOPIAN TUBE WITHIN NORMAL LIMITS. | |||
</pre> | |||
====Right then left==== | |||
<pre> | |||
A. Fallopian Tube, Right, Tubal Ligation: | |||
- Fallopian tube within normal limits, consistent with complete cross sections. | |||
B. Fallopian Tube, Left, Tubal Ligation: | |||
- Fallopian tube within normal limits, consistent with complete cross sections. | |||
</pre> | |||
<pre> | |||
A. FALLOPIAN TUBE, RIGHT, TUBAL LIGATION: | |||
- FALLOPIAN TUBE WITHIN NORMAL LIMITS, CONSISTENT WITH COMPLETE CROSS SECTIONS. | |||
B. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: | |||
- FALLOPIAN TUBE WITHIN NORMAL LIMITS, CONSISTENT WITH COMPLETE CROSS SECTIONS. | |||
</pre> | |||
<pre> | |||
A. FALLOPIAN TUBE, RIGHT, TUBAL LIGATION: | A. FALLOPIAN TUBE, RIGHT, TUBAL LIGATION: | ||
- FALLOPIAN TUBE WITHIN NORMAL LIMITS. | - FALLOPIAN TUBE WITHIN NORMAL LIMITS. | ||
B. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: | |||
- FALLOPIAN TUBE WITHIN NORMAL LIMITS. | |||
</pre> | |||
====Both in one container==== | |||
<pre> | |||
Submitted as "Fallopian Tubes Right and Left", Tubal Ligation: | |||
- Pieces of Fallopian tube within normal limits, consistent with | |||
complete cross sections. | |||
</pre> | |||
<pre> | |||
Submitted as "Fallopian Tubes Right and Left", Partial Excision: | |||
- Pieces of Fallopian tube within normal limits, consistent with | |||
complete cross sections and fibril ends. | |||
</pre> | |||
=====Incomplete cross sections at microscopy===== | |||
<pre> | |||
Submitted as "Right and Left Fallopian Tubes", Tubal Ligation: | |||
- Fallopian tubes within normal limits, incomplete cross sections | |||
seen at microscopy; clinical correlation is suggested. | |||
</pre> | |||
=====Mild inflammation===== | |||
<pre> | |||
Submitted as "Fallopian Tubes Right and Left", Tubal Ligation: | |||
- Pieces of Fallopian tube with mild inflammation otherwise within | |||
normal limits, consistent with complete cross sections. | |||
</pre> | |||
====Surgical resection of previous tubal ligation==== | |||
<pre> | |||
LEFT FALLOPIAN TUBE AND OVARY, LEFT SALPINGO-OOPHORECTOMY: | |||
- FALLOPIAN TUBE WITH PARATUBAL CYSTS AND FOCAL FIBROSIS. | |||
- OVARY WITHIN NORMAL LIMITS. | |||
</pre> | |||
====Tubes with fimbria==== | |||
<pre> | |||
Submitted as "Right and Left Fallopian Tube Segments", Excision: | |||
- Fallopian tubes with fimbria within normal limits; complete cross sections seen. | |||
</pre> | </pre> | ||
| Line 58: | Line 194: | ||
*+/-Clusters of neutrophils = abscess; known as ''suppurative salpingitis''. | *+/-Clusters of neutrophils = abscess; known as ''suppurative salpingitis''. | ||
Images | ====Images==== | ||
<gallery> | |||
File:Salpingitis_-_low_mag.jpg | Salpingitis - low mag. (WC) | |||
File:Salpingitis_-_high_mag.jpg | Salpingitis - high mag. (WC) | |||
File:Granulomatous_salpingitis_-_intermed_mag.jpg | Granulomatous salpingitis - intermed mag. (WC) | |||
File:Granulomatous_salpingitis_-_high_mag.jpg | Granulomatous salpingitis - high mag. (WC) | |||
</gallery> | |||
===Stains=== | ===Stains=== | ||
If organisms are seen on routine stains: | If organisms are seen on routine stains: | ||
| Line 72: | Line 209: | ||
*[[GMS stain]] +ve/-ve. | *[[GMS stain]] +ve/-ve. | ||
*[[PASD stain]] +ve/-ve. | *[[PASD stain]] +ve/-ve. | ||
==Ectopic pregnancy== | |||
{{Main|Ectopic pregnancy}} | |||
==Adenofibroma== | ==Adenofibroma== | ||
| Line 130: | Line 270: | ||
*Abbreviated ''STIC''.<ref name=pmid21989347>{{Cite journal | last1 = Visvanathan | first1 = K. | last2 = Vang | first2 = R. | last3 = Shaw | first3 = P. | last4 = Gross | first4 = A. | last5 = Soslow | first5 = R. | last6 = Parkash | first6 = V. | last7 = Shih | first7 = IeM. | last8 = Kurman | first8 = RJ. | title = Diagnosis of serous tubal intraepithelial carcinoma based on morphologic and immunohistochemical features: a reproducibility study. | journal = Am J Surg Pathol | volume = 35 | issue = 12 | pages = 1766-75 | month = Dec | year = 2011 | doi = 10.1097/PAS.0b013e31822f58bc | PMID = 21989347 }}</ref> | *Abbreviated ''STIC''.<ref name=pmid21989347>{{Cite journal | last1 = Visvanathan | first1 = K. | last2 = Vang | first2 = R. | last3 = Shaw | first3 = P. | last4 = Gross | first4 = A. | last5 = Soslow | first5 = R. | last6 = Parkash | first6 = V. | last7 = Shih | first7 = IeM. | last8 = Kurman | first8 = RJ. | title = Diagnosis of serous tubal intraepithelial carcinoma based on morphologic and immunohistochemical features: a reproducibility study. | journal = Am J Surg Pathol | volume = 35 | issue = 12 | pages = 1766-75 | month = Dec | year = 2011 | doi = 10.1097/PAS.0b013e31822f58bc | PMID = 21989347 }}</ref> | ||
*[[AKA]] ''tubal intraepithelial carcinoma''. | *[[AKA]] ''tubal intraepithelial carcinoma''. | ||
{{Main|Serous tubal intraepithelial carcinoma}} | |||
== | ==Serous carcinoma of the fallopian tube== | ||
{{Main|Serous carcinoma of the fallopian tube}} | |||
== | |||
=See also= | =See also= | ||
| Line 165: | Line 283: | ||
[[Category:Gynecologic pathology]] | [[Category:Gynecologic pathology]] | ||
[[Category:Uterine tubes]] | |||
Latest revision as of 05:11, 4 November 2024
Uterine tubes, also known as the Fallopian tubes, serve as a connection between the ovaries and the uterus. It is where fertilization usually takes place.
.jpg){kind=link}
This was ignored in the past... current thinking is that it may be the real culprit in what is often labeled as "ovarian cancer".[1]
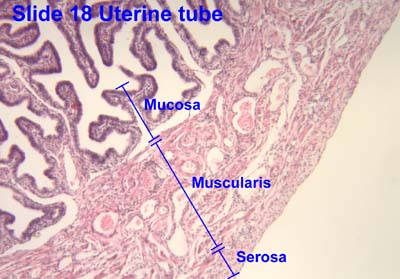
Normal uterine tube
Architecture:
- Finger-like projections into the lumen.
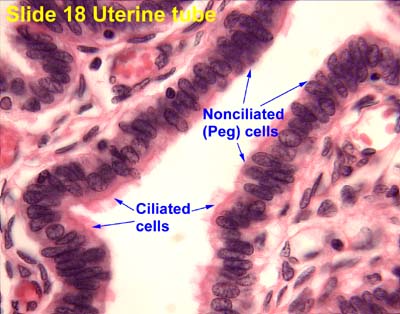
Cells:
- Ciliated cell.
- Columnar.
- Eosinophilic cytoplasm.
- Non-ciliated cell (AKA Peg cell).
- Nucleus more luminal.
- Nuclei stick-out like a golf tee.
- Nucleus more luminal.
- Secretory cells. (???)
- Basal cells, fried egg-like.
See also:
Images
www:
{kind=link}
{kind=link}
{kind=link}
Overview
Benign lesions
Benign neoplasm
Pre-malignant
Malignant diagnoses
- Serous carcinoma.
- Endometrioid adenocarcinoma.[3]
Ditzels
Paratubal cyst
- Also known as Hydatid cyst of Morgagni and Hydatid of Morgagni.
General
Gross
- Thin walled-cyst with serous fluid.
Microscopic
Features:
- Simple cyst with ciliated (tubal) epithelium.
Sign out
PARATUBAL CYST, RIGHT, EXCISION: - BENIGN SIMPLE CYST.
No epithelium
PARATUBAL CYST, LEFT, EXCISION: - BENIGN FIBROUS TISSUE COMPATIBLE WITH CYST WALL.
Tubal ligation
- Abbreviated TL.
General
- Done to control fertility.
Microscopic
See normal uterine tube.
DDx:
- Salpingitis - inflammatory cells.
- Serous carcinoma - nuclear atypia (marked), nuclear pleomorphism, prominent nucleoli.
- Tubal intraepithelial carcinoma - discrete papillary growth, loss of nuclear polarity, nuclear atypia.
- Endometriosis.
Sign out
Left then right
A. Fallopian Tube, Left, Tubal Ligation: - Fallopian tube within normal limits, consistent with complete cross sections. B. Fallopian Tube, Right, Tubal Ligation: - Fallopian tube within normal limits, consistent with complete cross sections.
A. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: - FALLOPIAN TUBE WITHIN NORMAL LIMITS, CONSISTENT WITH COMPLETE CROSS SECTIONS. B. FALLOPIAN TUBE, RIGHT, TUBAL LIGATION: - FALLOPIAN TUBE WITHIN NORMAL LIMITS, CONSISTENT WITH COMPLETE CROSS SECTIONS.
A. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: - FALLOPIAN TUBE WITHIN NORMAL LIMITS. B. FALLOPIAN TUBE, RIGHT, TUBAL LIGATION: - FALLOPIAN TUBE WITHIN NORMAL LIMITS.
Right then left
A. Fallopian Tube, Right, Tubal Ligation: - Fallopian tube within normal limits, consistent with complete cross sections. B. Fallopian Tube, Left, Tubal Ligation: - Fallopian tube within normal limits, consistent with complete cross sections.
A. FALLOPIAN TUBE, RIGHT, TUBAL LIGATION: - FALLOPIAN TUBE WITHIN NORMAL LIMITS, CONSISTENT WITH COMPLETE CROSS SECTIONS. B. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: - FALLOPIAN TUBE WITHIN NORMAL LIMITS, CONSISTENT WITH COMPLETE CROSS SECTIONS.
A. FALLOPIAN TUBE, RIGHT, TUBAL LIGATION: - FALLOPIAN TUBE WITHIN NORMAL LIMITS. B. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: - FALLOPIAN TUBE WITHIN NORMAL LIMITS.
Both in one container
Submitted as "Fallopian Tubes Right and Left", Tubal Ligation:
- Pieces of Fallopian tube within normal limits, consistent with
complete cross sections.
Submitted as "Fallopian Tubes Right and Left", Partial Excision:
- Pieces of Fallopian tube within normal limits, consistent with
complete cross sections and fibril ends.
Incomplete cross sections at microscopy
Submitted as "Right and Left Fallopian Tubes", Tubal Ligation:
- Fallopian tubes within normal limits, incomplete cross sections
seen at microscopy; clinical correlation is suggested.
Mild inflammation
Submitted as "Fallopian Tubes Right and Left", Tubal Ligation:
- Pieces of Fallopian tube with mild inflammation otherwise within
normal limits, consistent with complete cross sections.
Surgical resection of previous tubal ligation
LEFT FALLOPIAN TUBE AND OVARY, LEFT SALPINGO-OOPHORECTOMY: - FALLOPIAN TUBE WITH PARATUBAL CYSTS AND FOCAL FIBROSIS. - OVARY WITHIN NORMAL LIMITS.
Tubes with fimbria
Submitted as "Right and Left Fallopian Tube Segments", Excision:
- Fallopian tubes with fimbria within normal limits; complete cross sections seen.
Specific diagnoses
Salpingitis
- Also suppurative salpingitis.
- Also granulomatous salpingitis.
General
- Benign.
- May be part of pelvic inflammatory disease.
Microscopic
Features:
- Inflammatory cells:
- Neutrophils = acute.
- Lymphocytes and plasma cells = chronic.
- +/-Granulomas; known as granulomatous salpingitis.
- +/-Clusters of neutrophils = abscess; known as suppurative salpingitis.
Images
- Salpingitis - low mag.jpg
Salpingitis - low mag. (WC)
- Salpingitis - high mag.jpg
Salpingitis - high mag. (WC)
- Granulomatous salpingitis - intermed mag.jpg
Granulomatous salpingitis - intermed mag. (WC)
- Granulomatous salpingitis - high mag.jpg
Granulomatous salpingitis - high mag. (WC)
Stains
If organisms are seen on routine stains:
- Gram stain +ve/-ve.
Granulomatous inflammation:
- Ziehl-Neelsen stain +ve/-ve.
- GMS stain +ve/-ve.
- PASD stain +ve/-ve.
Ectopic pregnancy
Adenofibroma
General
- Rare.[6]
- More frequently seen than in the past -- presumably as pathologists are looking more closely at the Fallopian tube.
- Cannot be disguished from ovarian adenofibroma.[6]
Gross
- Solid, nodular.
Microscopic
Features:[6]
- Stroma + glandular elements.
- Glandular elements: secretory cells and ciliated cells.
IHC
Features:
- Stroma:[6]
- CD10 +ve.
- Inhibin +ve.
Salpingitis isthmica nodosa
General
- Associated with infertility and ectopic pregnancy.[9]
- SIN is uncommonly bilateral.[10]
Diagnosis (clinical):
- Hysterosalpingography.[11]
- Finding: diverticula.
Notes:
- The male cousin of this is: vasitis nodosa.
Microscopic
Features:[12]
- Nodular thickening of the tunica muscularis of the isthmic portion.
- Cystically dilated glands.
- +/-Complete obliteration of tubal lumen.
Images:
{kind=link}
Adenomatoid tumour
See: Adenomatoid tumours (uterine tumours).
General
- Relatively common tumour of the fallopian tube.[13]
Microscopic
See: Adenomatoid tumours (uterine tumours).
Serous tubal intraepithelial carcinoma
Serous carcinoma of the fallopian tube
See also
References
- ↑ Hirst, JE.; Gard, GB.; McIllroy, K.; Nevell, D.; Field, M. (Jul 2009). "High rates of occult fallopian tube cancer diagnosed at prophylactic bilateral salpingo-oophorectomy.". Int J Gynecol Cancer 19 (5): 826-9. doi:10.1111/IGC.0b013e3181a1b5dc. PMID 19574767.
- ↑ URL: http://faculty.une.edu/com/abell/histo/histolab3f.htm. Accessed on: 18 October 2011.
- ↑ Navani, SS.; Alvarado-Cabrero, I.; Young, RH.; Scully, RE. (Dec 1996). "Endometrioid carcinoma of the fallopian tube: a clinicopathologic analysis of 26 cases.". Gynecol Oncol 63 (3): 371-8. doi:10.1006/gyno.1996.0338. PMID 8946874.
- ↑ Thakore, SS.; Chun, MJ.; Fitzpatrick, K. (Aug 2012). "Recurrent ovarian torsion due to paratubal cysts in an adolescent female.". J Pediatr Adolesc Gynecol 25 (4): e85-7. doi:10.1016/j.jpag.2011.10.012. PMID 22840942.
- ↑ Muolokwu, E.; Sanchez, J.; Bercaw, JL.; Sangi-Haghpeykar, H.; Banszek, T.; Brandt, ML.; Dietrich, JE. (Nov 2011). "Paratubal cysts, obesity, and hyperandrogenism.". J Pediatr Surg 46 (11): 2164-7. doi:10.1016/j.jpedsurg.2011.07.011. PMID 22075351.
- ↑ 6.0 6.1 6.2 6.3 Bossuyt, V.; Medeiros, F.; Drapkin, R.; Folkins, AK.; Crum, CP.; Nucci, MR. (Jul 2008). "Adenofibroma of the fimbria: a common entity that is indistinguishable from ovarian adenofibroma.". Int J Gynecol Pathol 27 (3): 390-7. doi:10.1097/PGP.0b013e3181639a82. PMID 18580316.
- ↑ Stedman's Medical Dictionary. 27th Ed. Lippincott Williams & Wilkins.
- ↑ URL: http://www.medcyclopaedia.com/library/topics/volume_iv_2/s/salpingitis_isthmica_nodosa.aspx. Accessed on: 28 July 2010.
- ↑ Jenkins, CS.; Williams, SR.; Schmidt, GE. (Oct 1993). "Salpingitis isthmica nodosa: a review of the literature, discussion of clinical significance, and consideration of patient management.". Fertil Steril 60 (4): 599-607. PMID 8405510.
- ↑ Skibsted, L.; Sperling, L.; Hansen, U.; Hertz, J. (Jul 1991). "Salpingitis isthmica nodosa in female infertility and tubal diseases.". Hum Reprod 6 (6): 828-31. PMID 1757522.
- ↑ URL: http://radiology.rsna.org/content/154/3/597.abstract. Accessed on: 28 July 2010.
- ↑ Chawla, N.; Kudesia, S.; Azad, S.; Singhal, M.; Rai, SM.. "Salpingitis isthmica nodosa.". Indian J Pathol Microbiol 52 (3): 434-5. doi:10.4103/0377-4929.55019. PMID 19679986.
- ↑ Christensen C (1990). "Adenomatoid tumors of the uterus". Eur. J. Gynaecol. Oncol. 11 (2): 85–9. PMID 2199199.
- ↑ Visvanathan, K.; Vang, R.; Shaw, P.; Gross, A.; Soslow, R.; Parkash, V.; Shih, IeM.; Kurman, RJ. (Dec 2011). "Diagnosis of serous tubal intraepithelial carcinoma based on morphologic and immunohistochemical features: a reproducibility study.". Am J Surg Pathol 35 (12): 1766-75. doi:10.1097/PAS.0b013e31822f58bc. PMID 21989347.