|
|
| (24 intermediate revisions by 2 users not shown) |
| Line 1: |
Line 1: |
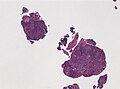
| | [[Image:Mixed_Germ_Cell_Tumor_of_Testis_(3260625567).jpg|thumb|right|Testicular [[mixed germ cell tumour]]. (WC/euthman)]] |
| This article covers '''germ cell tumours''', often abbreviated [[GCT]], which classically arise in the gonads ([[ovary]], [[testis]]). They are also found in the midline and make appearances in [[neuropathology]] (e.g. [[pineal gland]]) and in the [[mediastinum]]. | | This article covers '''germ cell tumours''', often abbreviated [[GCT]], which classically arise in the gonads ([[ovary]], [[testis]]). They are also found in the midline and make appearances in [[neuropathology]] (e.g. [[pineal gland]]) and in the [[mediastinum]]. |
|
| |
|
| Line 21: |
Line 22: |
|
| |
|
| ===Grossing=== | | ===Grossing=== |
| *1 cm^2 of tumour per cm of maximal tumour dimension - guideline for testicular cancer.<ref>URL: [http://www.uroweb.org/gls/pdf/10_Testicular_Cancer.pdf http://www.uroweb.org/gls/pdf/10_Testicular_Cancer.pdf]. Accessed on: 30 October 2012.</ref> | | {{Main|Orchiectomy}} |
| | *1 cm<sup>2</sup> of tumour per cm of maximal tumour dimension - guideline for testicular cancer.<ref>URL: [http://www.uroweb.org/gls/pdf/10_Testicular_Cancer.pdf http://www.uroweb.org/gls/pdf/10_Testicular_Cancer.pdf]. Accessed on: 30 October 2012.</ref> |
|
| |
|
| ===IHC for GCTs=== | | ===IHC for GCTs=== |
| ABCDs of GCTs: | | ====ISUP==== |
| | An algorithmic approach based on the ISUP consensus paper by Ulbright ''et al.'':<ref name=pmid24832161>{{cite journal |author=Ulbright TM, Tickoo SK, Berney DM, Srigley JR |title=Best practices recommendations in the application of immunohistochemistry in testicular tumors: report from the international society of urological pathology consensus conference |journal=Am. J. Surg. Pathol. |volume=38 |issue=8 |pages=e50–9 |year=2014 |month=August |pmid=24832161 |doi=10.1097/PAS.0000000000000233 |url=}}</ref> |
| | {{familytree/start}} |
| | {{familytree | | | | | | | | | | | | | A01 | | | | | | | | | | | | | | | | | | |A01=[[Germ cell tumours]]}} |
| | {{familytree | | | | | |,|-|-|-|-|-|-|-|^|-|-|-|-|-|-|-|.| | | | | | | | | | | |}} |
| | {{familytree | | | | | B01 | | | | | | | | | | | | | | B02 | | | | | | | | | | |B01=OCT4 +ve | B02=OCT4 -ve}} |
| | {{familytree | |,|-|-|-|^|-|-|-|.| | | | | |,|-|-|-|-|-|+|-|-|-|-|-|.| | | | | |}} |
| | {{familytree | C01 | | | | | | C02 | | | | C03 | | | | C04 | | | | C05 | | | | |C01=CD117 +ve<br>CD30 -ve |C02= CD117 -ve<br>CD30 +ve|C03=[[Glypican 3]] +ve<br>AFP +ve<br>beta-hCG -ve|C04=Glypican 3 ?<br>AFP -ve<br>beta-hCG +ve|C05=Glypican 3 -ve<br>AFP -ve<br>beta-hCG -ve}} |
| | {{familytree | |!| | | | | | | |!| | | | | |!| | | | | |!| | | | | |!| | | | | |}} |
| | {{familytree | D01 | | | | | | D02 | | | | D03 | | | | D04 | | | | D05 | | | | |D01=[[Seminoma]]|D02=[[Embryonal carcinoma]]|D03=[[Yolk sac tumour]]|D04=[[Choriocarcinoma]] |D05= [[Spermatocytic seminoma]] }} |
| | {{familytree/end}} |
| | |
| | ====ABCDs of GCTs==== |
| *AFP - yolk sac tumour. | | *AFP - yolk sac tumour. |
| *Beta-hCG - choriocarcinoma. | | *Beta-hCG - choriocarcinoma. |
| *CD30 - embryonal carcinoma. | | *CD30 - embryonal carcinoma. |
| *D2-40 - seminoma. | | *D2-40 - seminoma. |
| | |
| | ====GCT versus sex cord-stromal tumour==== |
| | The ISUP recommends:<ref name=pmid25025364>{{cite journal |author=Amin MB, Epstein JI, Ulbright TM, ''et al.'' |title=Best practices recommendations in the application of immunohistochemistry in urologic pathology: report from the international society of urological pathology consensus conference |journal=Am. J. Surg. Pathol. |volume=38 |issue=8 |pages=1017–22 |year=2014 |month=August |pmid=25025364 |doi=10.1097/PAS.0000000000000254 |url=}}</ref> |
| | *[[SALL4]] +ve (in GCTs).<ref name=pmid24525512>{{cite journal |author=Miettinen M, Wang Z, McCue PA, ''et al.'' |title=SALL4 expression in germ cell and non-germ cell tumors: a systematic immunohistochemical study of 3215 cases |journal=Am. J. Surg. Pathol. |volume=38 |issue=3 |pages=410–20 |year=2014 |month=March |pmid=24525512 |doi=10.1097/PAS.0000000000000116 |url=}}</ref> |
| | *Alpha-inhibin -ve (+ve in [[SCST]]). |
| | *Calretinin -ve (+ve in SCST). |
| | |
| | Alternates for SALL4 are:<ref name=pmid25025364/> |
| | *OCT4 and GPC3. |
|
| |
|
| ===Tabular summary of GCTs=== | | ===Tabular summary of GCTs=== |
| Line 39: |
Line 62: |
| ! Image | | ! Image |
| |- | | |- |
| | Intratubular germ cell neoplasia (ITGCN) | | | [[Germ cell neoplasia in situ]] (GCNIS) |
| | nests of small fried egg cells | | | nests of small fried egg cells |
| | large central nucleus, clear <br>cytoplasm, squared-off nuclear membrane, nucleoli<ref name=Ref_GUP538>{{Ref GUP|538}}</ref> | | | large central nucleus, clear <br>cytoplasm, squared-off nuclear membrane, nucleoli<ref name=Ref_GUP538>{{Ref GUP|538}}</ref> |
| | CD117 | | | CD117 +ve, CD30 -ve |
| | appearance similar to seminoma | | | appearance similar to [[seminoma]] |
| | [[Image:Intratubular_germ_cell_neoplasia_high_mag_cropped.jpg|thumb|center|150px|ITGCN (WC/Nephron)]] | | | [[Image:Intratubular_germ_cell_neoplasia_high_mag_cropped.jpg|thumb|center|150px|GCNIS (WC/Nephron)]] |
| |- | | |- |
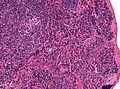
| | Germinoma / Seminoma / Dysgerminoma | | | [[Germinoma]] / [[Seminoma]] / [[Dysgerminoma]] |
| | fried egg cells | | | fried egg cells |
| | fried egg-like cells (central nucleus, clear <br>cytoplasm) with squared-off nuclear <br>membrane, nucleoli, lymphocytic infiltrate, granulomata,<br>syncytiotrophoblastic giant cells<ref name=Ref_GUP542>{{Ref GUP|542}}</ref> | | | fried egg-like cells (central nucleus, clear <br>cytoplasm) with squared-off nuclear <br>membrane, nucleoli, lymphocytic infiltrate, granulomata,<br>syncytiotrophoblastic giant cells<ref name=Ref_GUP542>{{Ref GUP|542}}</ref> |
| Line 56: |
Line 79: |
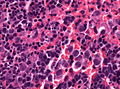
| | Schiller-Duval bodies | | | Schiller-Duval bodies |
| | Schiller-Duval b. = central blood vessel surrounded by epithelial-like cells a space and more epithelial-like cells, variable arch. | | | Schiller-Duval b. = central blood vessel surrounded by epithelial-like cells a space and more epithelial-like cells, variable arch. |
| | AFP | | | [[AFP]] +ve, [[Glypican 3]] +ve |
| | patterns: microcystic, solid, hepatoid | | | patterns: microcystic, solid, hepatoid |
| | [[Image:Mixed_germ_cell_tumour_-_very_high_mag.jpg|thumb|center|150px|Yolk sac tumour (WC)]] | | | [[Image:Mixed_germ_cell_tumour_-_very_high_mag.jpg|thumb|center|150px|Yolk sac tumour (WC)]] |
| Line 63: |
Line 86: |
| | prominent nucleoli, vescicular nuclei | | | prominent nucleoli, vescicular nuclei |
| | var. arch.: tubulopapillary, glandular, solid, embryoid bodies (ball of cells in surrounded by empty space on three sides), +/-nuclear overlap, mitoses common | | | var. arch.: tubulopapillary, glandular, solid, embryoid bodies (ball of cells in surrounded by empty space on three sides), +/-nuclear overlap, mitoses common |
| | CD30 | | | CD30 +ve, CD117 -ve |
| | usu. part of a mixed GCT | | | usu. part of a mixed GCT |
| | [[Image:Embryonal_carcinoma_high_mag.jpg|thumb|center|150px|Embryonal carcinoma (WC/Nephron)]] | | | [[Image:Embryonal_carcinoma_high_mag.jpg|thumb|center|150px|Embryonal carcinoma (WC/Nephron)]] |
| Line 70: |
Line 93: |
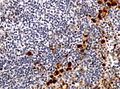
| | clear cytoplasm | | | clear cytoplasm |
| | cells with abundant clear cytoplasm and eccentric atypical nuclei (cytotrophoblast), very large (multinucleated) cells with abundant eosinophilic cytoplasm and extreme nuclear atypia (syncytiotrophoblast) | | | cells with abundant clear cytoplasm and eccentric atypical nuclei (cytotrophoblast), very large (multinucleated) cells with abundant eosinophilic cytoplasm and extreme nuclear atypia (syncytiotrophoblast) |
| | beta-hCG | | | beta-hCG +ve |
| | may be preceded by a [[complete mole|complete hydatidiform mole]] | | | may be preceded by a [[complete mole|complete hydatidiform mole]] |
| | [[Image:Choriocarcinoma_-2-_very_high_mag.jpg|thumb|center|150px|Choriocarcinoma. (WC/Nephron)]] | | | [[Image:Choriocarcinoma_-2-_very_high_mag.jpg|thumb|center|150px|Choriocarcinoma. (WC/Nephron)]] |
| Line 98: |
Line 121: |
| ===Molecular pathology=== | | ===Molecular pathology=== |
| Most common cytogenetic abnormality in GCTs: | | Most common cytogenetic abnormality in GCTs: |
| * Isochromosome p12.<ref name=pmid10357096>{{Cite journal | last1 = Looijenga | first1 = LH. | last2 = Oosterhuis | first2 = JW. | title = Pathogenesis of testicular germ cell tumours. | journal = Rev Reprod | volume = 4 | issue = 2 | pages = 90-100 | month = May | year = 1999 | doi = | PMID = 10357096 }}</ref> | | *[[Isochromosome 12p]].<ref name=pmid10357096>{{Cite journal | last1 = Looijenga | first1 = LH. | last2 = Oosterhuis | first2 = JW. | title = Pathogenesis of testicular germ cell tumours. | journal = Rev Reprod | volume = 4 | issue = 2 | pages = 90-100 | month = May | year = 1999 | doi = | PMID = 10357096 }}</ref> |
| ** Isochromosome = one arm (p or q) is lost and replaced with a duplicate of the remaining one. | | ** Isochromosome = one arm (p or q) is lost and replaced with a duplicate of the remaining one. |
| ***Example: isochromosome p12 = chromosome 12 where q is lost and two p arms are present.<ref>URL: [http://ghr.nlm.nih.gov/handbook/illustrations/isochromosomes http://ghr.nlm.nih.gov/handbook/illustrations/isochromosomes]. Accessed on: 15 February 2012.</ref> | | ***Example: isochromosome 12p = chromosome 12 where q is lost and two p arms are present.<ref>URL: [http://ghr.nlm.nih.gov/handbook/illustrations/isochromosomes http://ghr.nlm.nih.gov/handbook/illustrations/isochromosomes]. Accessed on: 15 February 2012.</ref> |
|
| |
|
| ==Germinoma== | | ==Germinoma== |
| Line 112: |
Line 135: |
|
| |
|
| Image: [http://path.upmc.edu/cases/case525/images/fig02a.jpg Germinoma (upmc.edu)].<ref>URL: [http://path.upmc.edu/cases/case525.html http://path.upmc.edu/cases/case525.html]. Accessed on: 25 January 2012.</ref> | | Image: [http://path.upmc.edu/cases/case525/images/fig02a.jpg Germinoma (upmc.edu)].<ref>URL: [http://path.upmc.edu/cases/case525.html http://path.upmc.edu/cases/case525.html]. Accessed on: 25 January 2012.</ref> |
| | |
| | <gallery> |
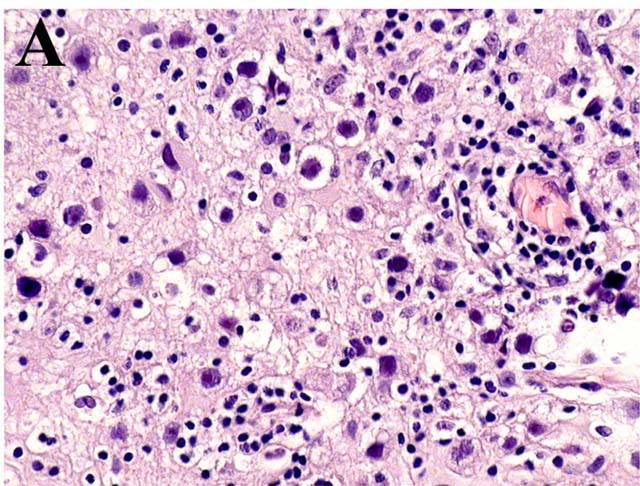
| | Image:Neuropathology_case_VIII_01.jpg | Germinoma of the brain, low mag. (WC/jensflorian) |
| | Image:Neuropathology_case_VIII_02.jpg | Germinoma intermed. mag. (WC/jensflorian) |
| | Image:Neuropathology_case_VIII_03.jpg | Germinoma very high. mag. (WC/jensflorian) |
| | Image:Neuropathology_case_VIII_05.jpg | Germinoma Oct3/4 staining (WC/jensflorian) |
| | </gallery> |
| | |
|
| |
|
| ===Seminoma=== | | ===Seminoma=== |
| {{Main|Testis#Seminoma}} | | {{Main|Seminoma}} |
| A common GCT in males. | | A common GCT in males. |
|
| |
|
| Line 122: |
Line 153: |
|
| |
|
| ==Yolk sac tumour== | | ==Yolk sac tumour== |
| *Abbreviated ''YST''.
| | {{Main|Yolk sac tumour}} |
| *[[AKA]] ''endodermal sinus tumour''.
| |
| ===General===
| |
| *Rare.
| |
| *Aggressive - especially extragonadal tumours.<ref name=pmid18767035/>
| |
| | |
| Epidemiology:
| |
| *Most common GCT in infants and young boys.
| |
| *Bimodal age distribution:<ref name=pmid18767035>{{Cite journal | last1 = Shah | first1 = JP. | last2 = Kumar | first2 = S. | last3 = Bryant | first3 = CS. | last4 = Ali-Fehmi | first4 = R. | last5 = Malone | first5 = JM. | last6 = Deppe | first6 = G. | last7 = Morris | first7 = RT. | title = A population-based analysis of 788 cases of yolk sac tumors: A comparison of males and females. | journal = Int J Cancer | volume = 123 | issue = 11 | pages = 2671-5 | month = Dec | year = 2008 | doi = 10.1002/ijc.23792 | PMID = 18767035 }}</ref>
| |
| **<4 years.
| |
| **10-30 years.
| |
| | |
| Clinical:
| |
| *Elevated AFP.
| |
| | |
| ===Gross===
| |
| *White/yellow mucinous infiltrative mass.<ref name=Ref_PCPBoD8_510>{{Ref PCPBoD8|510}}</ref>
| |
| | |
| ===Microscopic===
| |
| Classic feature:<ref name=Ref_PCPBoD8_510>{{Ref PCPBoD8|510}}</ref>
| |
| *Schiller-Duval bodies.
| |
| **Look like glomerulus - central blood vessel surrounded by epithelial-like cells a space and more epithelial-like cells
| |
| *Architecure - variable.
| |
| *#Reticular - most common according to WMSP.<ref name=Ref_WMSP369>{{Ref WMSP|369}}</ref>
| |
| *#Microcystic - most common according to ''webpathology.com''.<ref name=webpath_case34>URL: [http://webpathology.com/image.asp?case=34&n=1 http://webpathology.com/image.asp?case=34&n=1]. Accessed on: March 8, 2010.</ref>
| |
| *#*Lace-like pattern.
| |
| *#Endodermal sinus-like - has Schiller-Duval bodies.
| |
| *#Solid.
| |
| *#Papillary.
| |
| *#Glandular.
| |
| *#Alveolar.
| |
| *#Enteric.
| |
| *#Polyvesicular vitelline.
| |
| *#Hepatoid.
| |
| *+/-Eosinophilic hyaline globules (contain alpha-fetoprotein).
| |
| | |
| Notes:
| |
| *Has a loose stroma/vaguely discohesive -- unlike embryonal carcinoma.
| |
| *How to remember patterns ''REM PS GAPEH'' = reticular, endodermal sinus, microcystic, papillary, solid, glandular, alveolar, polyvesicular vitelline, enteric, hepatoid.
| |
| *Yolk sac tumours in adults are essentially always a component of a [[mixed germ cell tumour]], i.e. if one sees a pure yolk sac tumour in an adult, it is probably under sampled.<ref name=pmid1203848>{{Cite journal | last1 = Talerman | first1 = A. | title = The incidence of yolk sac tumor (endodermal sinus tumor) elements in germ cell tumors of the testis in adults. | journal = Cancer | volume = 36 | issue = 1 | pages = 211-5 | month = Jul | year = 1975 | doi = | PMID = 1203848 }}</ref>
| |
| | |
| Variants:
| |
| *Hepatoid pattern.<ref>URL: [http://webpathology.com/image.asp?case=34&n=6 http://webpathology.com/image.asp?case=34&n=6]. Accessed on: March 8, 2010.</ref>
| |
| **Vaguely resembles liver.
| |
| ***[[Hyaline globules]] (light red well-circumscribed globs).
| |
| ***Bile canaculi.
| |
| *Solid pattern.<ref>URL: [http://webpathology.com/image.asp?case=34&n=8 http://webpathology.com/image.asp?case=34&n=8]. Accessed on: March 8, 2010.</ref>
| |
| **Vaguely resembles ''seminoma''.
| |
| | |
| DDx:
| |
| *[[Embryonal carcinoma]].
| |
| | |
| ====Images====
| |
| <gallery>
| |
| Image:Mixed_germ_cell_tumour_-_very_high_mag.jpg|Yolk sac tumour. (WC/Nephron)
| |
| </gallery>
| |
| www:
| |
| *[http://webpathology.com/image.asp?case=34&n=6 Hepatoid Pattern (webpathology.com)].
| |
| *[http://www.webpathology.com/image.asp?case=34&n=5 Schiller-Duval body (webpathology.com)].
| |
| *[http://www.webpathology.com/image.asp?n=6&Case=34 Hyaline globules (webpathology.com)].
| |
| *[http://path.upmc.edu/cases/case152.html Yolk sac tumour - case 1 - several images (upmc.edu)].
| |
| *[http://path.upmc.edu/cases/case492.html Yolk sac tumour - case 2 - several images (upmc.edu)].
| |
| *[http://www.moffitt.org/CCJRoot/v11n6/pdf/374.pdf Yolk sac tumour (moffitt.org)].<ref name=pmid15625525>{{Cite journal | last1 = Sesterhenn | first1 = IA. | last2 = Davis | first2 = CJ. | title = Pathology of germ cell tumors of the testis. | journal = Cancer Control | volume = 11 | issue = 6 | pages = 374-87 | month = | year = | doi = | PMID = 15625525 }}</ref>
| |
| | |
| ===IHC===
| |
| *AFP +ve.
| |
| *Glypican 3 +ve.
| |
| **More sensitive than AFP.<ref name=pmid20438407>{{Cite journal | last1 = Emerson | first1 = RE. | last2 = Ulbright | first2 = TM. | title = Intratubular germ cell neoplasia of the testis and its associated cancers: the use of novel biomarkers. | journal = Pathology | volume = 42 | issue = 4 | pages = 344-55 | month = Jun | year = 2010 | doi = 10.3109/00313021003767355 | PMID = 20438407 }}</ref>
| |
| *Alpha-1 AT +ve.
| |
| *Cytokeratin +ve.{{fact}}
| |
| | |
| Negative stains:<ref name=pmid19396148>{{Cite journal | last1 = Gopalan | first1 = A. | last2 = Dhall | first2 = D. | last3 = Olgac | first3 = S. | last4 = Fine | first4 = SW. | last5 = Korkola | first5 = JE. | last6 = Houldsworth | first6 = J. | last7 = Chaganti | first7 = RS. | last8 = Bosl | first8 = GJ. | last9 = Reuter | first9 = VE. | title = Testicular mixed germ cell tumors: a morphological and immunohistochemical study using stem cell markers, OCT3/4, SOX2 and GDF3, with emphasis on morphologically difficult-to-classify areas. | journal = Mod Pathol | volume = 22 | issue = 8 | pages = 1066-74 | month = Aug | year = 2009 | doi = 10.1038/modpathol.2009.66 | PMID = 19396148 }}</ref>
| |
| *OCT3/4 - positive in [[seminoma]] and embryonal carcinoma.
| |
| *CD30 - positive in [[embryonal carcinoma]].
| |
|
| |
|
| ==Embryonal carcinoma== | | ==Embryonal carcinoma== |
| ===General===
| | {{Main|Embryonal carcinoma}} |
| *Affects young adults.
| |
| **May be seen in women.
| |
| | |
| ===Microscopic===
| |
| Features:<ref name=Ref_GUP549>{{Ref GUP|549}}</ref>
| |
| #Nucleoli - '''key feature'''.
| |
| #Vesicular nuclei (clear, empty appearing nuclei) - '''key feature'''.
| |
| #Nuclei overlap.
| |
| #[[Necrosis]] - common.
| |
| #*Not commonly present in seminoma.
| |
| #Indistinct cell borders
| |
| #Mitoses - common.
| |
| #Variable architecture:
| |
| #*Tubulopapillary.
| |
| #*Glandular.
| |
| #*Solid.
| |
| #*Embryoid bodies - ball of cells in surrounded by empty space on three sides.
| |
| | |
| Notes:
| |
| *Cytoplasmic staining variable (eosinophilic to basophilic).
| |
| | |
| DDx:
| |
| *[[Yolk sac tumour]].
| |
| | |
| ====Images====
| |
| <gallery>
| |
| Image:Embryonal_carcinoma_-_very_high_mag_-_cropped.jpg | Embryonal carcinoma - very high mag. - cropped (WC/Nephron)
| |
| Image:Embryonal_carcinoma_-_high_mag.jpg | Embryonal carcinoma - high mag. (WC/Nephron)
| |
| </gallery>
| |
| <gallery>
| |
| Image:Embryonal_carcinoma_high_mag.jpg | Embryonal carcinoma - high mag. (WC/Nephron)
| |
| Image:Embryonal_carcinoma_intermed_mag.jpg | Embryonal carcinoma - intermed. mag. (WC/Nephron)
| |
| Image:Embryonal_carcinoma_low_mag.jpg | Embryonal carcinoma - low mag. (WC/Nephron)
| |
| </gallery>
| |
| ===IHC===
| |
| *AE1/AE3 +ve.
| |
| *CD30 +ve.
| |
|
| |
|
| ==Choriocarcinoma== | | ==Choriocarcinoma== |
| ===General===
| | {{Main|Choriocarcinoma}} |
| *Aggressive clinical course.
| |
| *Usually a mixed tumour, i.e. pure choriocarcinoma is rare, e.g. [[dysgerminoma]] + choriocarcinoma.
| |
| | |
| ====Clinical====
| |
| *High beta-hCG -- usually > 10,000 IU.
| |
| *Vaginal bleeding.
| |
| *Occasionally thyrotoxicosis.<ref name=pmid8395487>{{Cite journal | last1 = O'Reilly | first1 = S. | last2 = Lyons | first2 = DJ. | last3 = Harrison | first3 = M. | last4 = Gaffney | first4 = E. | last5 = Cullen | first5 = M. | last6 = Clancy | first6 = L. | title = Thyrotoxicosis induced by choriocarcinoma a report of two cases. | journal = Ir Med J | volume = 86 | issue = 4 | pages = 124, 127 | month = | year = | doi = | PMID = 8395487 }}</ref>
| |
| | |
| ====Epidemiology====
| |
| *May be preceded by a [[complete hydatidiform mole]].<ref name=Ref_PBoD1110-1>{{Ref PBoD|1110-1111}}</ref>
| |
| *More common in the far east.
| |
| *More common at extremes of fertile age (teens and 40-50 years).
| |
| | |
| ===Microscopic===
| |
| Features:
| |
| *Two cell populations:
| |
| #'''C'''ytotrophoblasts - '''key feature'''.
| |
| #*'''C'''lear cytoplasm.
| |
| #*Polygonal shaped cells in cords/masses.
| |
| #*Distinct cell borders.
| |
| #*Single uniform nucleus.
| |
| #Syncytiotrophoblasts - may be absent.<ref>URL: [http://www.webpathology.com/image.asp?n=4&Case=36 http://www.webpathology.com/image.asp?n=4&Case=36]. Accessed on: 8 February 2011.</ref>
| |
| #*Large + many irreg. or lobular hyperchromatic nuclei.
| |
| #*Eosinophilic vacuolated cytoplasm (contains hCG).
| |
| *+/-Hemorrhage - classically in the centre of the lesion.
| |
| *+/-Necrosis.
| |
| | |
| Notes:
| |
| *No ''[[chorionic villi]]'' should be present.
| |
| **If chorionic villi are present... it is likely a type of [[hydatidiform mole]].
| |
| *The dual cell population may not be evident at first.
| |
| **Hemorrhage and marked nuclear pleomorphism are suggestive of the diagnosis.
| |
| | |
| DDx:
| |
| *[[Invasive hydatidiform mole]].
| |
| *[[Placental site trophoblastic tumour]] (PSTT).
| |
| | |
| ====Images====
| |
| www:
| |
| *[http://www.webpathology.com/image.asp?n=5&Case=36 Choriocarcinoma - low mag. (webpathology.com)].
| |
| *[http://www.webpathology.com/image.asp?case=36&n=1 Choriocarcinoma (webpathology.com)].
| |
| *[http://www.webpathology.com/image.asp?n=4&Case=36 Choriocarcinoma (webpathology.com)].
| |
| *[http://chestjournal.chestpubs.org/content/138/1/220.full Choriocarcinoma (chestjournal.chestpubs.org)].<ref>{{Cite journal | last1 = Venkatram | first1 = S. | last2 = Muppuri | first2 = S. | last3 = Niazi | first3 = M. | last4 = Fuentes | first4 = GD. | title = A 24-year-old pregnant patient with diffuse alveolar hemorrhage. | journal = Chest | volume = 138 | issue = 1 | pages = 220-3 | month = Jul | year = 2010 | doi = 10.1378/chest.09-2688 | PMID = 20605823 }}</ref>
| |
| *[http://oac.med.jhmi.edu/Pathology/Repro/Placenta/279B_Full.html Choriocarcinoma - uterus (med.jhmi.edu)].
| |
| <gallery>
| |
| Image:Choriocarcinoma_-2-_high_mag.jpg | Choriocarcinoma - high mag. (WC/Nephron)
| |
| Image:Choriocarcinoma_-2-_very_high_mag.jpg | Choriocarcinoma - very high mag. (WC/Nephron)
| |
| </gallery>
| |
| ===IHC===
| |
| *Beta-hCG +ve.
| |
| **Classically said to be produced by syncytiotrophoblasts.<ref name=pmid20735820>{{Cite journal | last1 = Cole | first1 = LA. | title = Biological functions of hCG and hCG-related molecules. | journal = Reprod Biol Endocrinol | volume = 8 | issue = | pages = 102 | month = | year = 2010 | doi = 10.1186/1477-7827-8-102 | PMID = 20735820 | PMC = 2936313 | URL = http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2936313/ }}</ref>
| |
| ***Cytotrophoblasts also produce some<ref name=pmid20735820/><ref name=pmid12242037>{{Cite journal | last1 = Kovalevskaya | first1 = G. | last2 = Genbacev | first2 = O. | last3 = Fisher | first3 = SJ. | last4 = Caceres | first4 = E. | last5 = O'Connor | first5 = JF. | title = Trophoblast origin of hCG isoforms: cytotrophoblasts are the primary source of choriocarcinoma-like hCG. | journal = Mol Cell Endocrinol | volume = 194 | issue = 1-2 | pages = 147-55 | month = Aug | year = 2002 | doi = | PMID = 12242037 }}</ref> - usu. no staining.
| |
| *MUC-4 +ve.<ref name=pmid18059230>{{Cite journal | last1 = Mao | first1 = TL. | last2 = Kurman | first2 = RJ. | last3 = Huang | first3 = CC. | last4 = Lin | first4 = MC. | last5 = Shih | first5 = IeM. | title = Immunohistochemistry of choriocarcinoma: an aid in differential diagnosis and in elucidating pathogenesis. | journal = Am J Surg Pathol | volume = 31 | issue = 11 | pages = 1726-32 | month = Nov | year = 2007 | doi = 10.1097/PAS.0b013e318058a529 | PMID = 18059230 }}</ref>
| |
| *Ki-67 +ve -- typically >30%.
| |
|
| |
|
| ==Teratoma== | | ==Teratoma== |
| ===General===
| | {{Main|Teratoma}} |
| *May be benign or malignant.
| |
| *Are supposed to consists of all three [[germ layers]] - this is not always true.
| |
| *May be associated with sacral agenesis.<ref name=omim176450>{{OMIM|176450}}</ref>
| |
| | |
| Important note:
| |
| *The site of the tumour, age and sex are very important for predicting the behaviour of a teratoma:<ref>URL: [http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2011/GermCell_11protocol.pdf http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2011/GermCell_11protocol.pdf]. Accessed on: 29 April 2012.</ref>
| |
| **Immature teratomas may have a benign or malignant behaviour.
| |
| **Mature teratomas may have a benign or malignant behaviour.
| |
|
| |
|
| ====Classification====
| |
| #Mature.
| |
| #*Common in females.
| |
| #*Usually benign.
| |
| #*Mature component may give rise to a malignancy like elsewhere in the body.
| |
| #**Most common malignancy arising from a mature teratoma: [[squamous cell carcinoma]].
| |
| #Immature.
| |
| #*Uncommon.
| |
| #*Often malignant.
| |
| #Monodermal.
| |
| #*Rare.
| |
| #*Highly specialized.
| |
|
| |
| ===Mature teratoma===
| |
| Features - three germ cell layers (usually):<ref>{{cite book |author=Moore, Keith L.; Persaud, T.V.N.|title=The Developing Human: Clinically Oriented Embryology |publisher=Saunders |location= |year=2002 |pages= 83 |edition=7th |isbn=978-0721694122 |oclc= |doi= |accessdate=}}</ref>
| |
| #Endoderm:
| |
| #*Skin, (mature) CNS.
| |
| #Mesoderm:
| |
| #*Muscle, bone, connective tissue, blood.
| |
| #Ectoderm:
| |
| #*Internal organs.
| |
|
| |
| Note:
| |
| *May consist of skin only - in which case it is commonly called a ''dermoid''.
| |
|
| |
| =====Images=====
| |
| <gallery>
| |
| Image:Teratoma_2_low_mag.jpg | Mature teratoma - low mag. (WC/Nephron)
| |
| Image:Teratoma_2_high_mag.jpg | Mature teratoma - high mag. (WC/Nephron)
| |
| </gallery>
| |
|
| |
| ====Fetus in fetu====
| |
| *Grouped with ''mature teratoma'', as it is considered a well-developed mature teratoma.<ref name=pmid3045784>{{Cite journal | last1 = Heifetz | first1 = SA. | last2 = Alrabeeah | first2 = A. | last3 = Brown | first3 = BS. | last4 = Lau | first4 = H. | title = Fetus in fetu: a fetiform teratoma. | journal = Pediatr Pathol | volume = 8 | issue = 2 | pages = 215-26 | month = | year = 1988 | doi = | PMID = 3045784 }}</ref><ref name=pmid17183856>{{Cite journal | last1 = Basu | first1 = A. | last2 = Jagdish | first2 = S. | last3 = Iyengar | first3 = KR. | last4 = Basu | first4 = D. | title = Fetus in fetu or differentiated teratomas? | journal = Indian J Pathol Microbiol | volume = 49 | issue = 4 | pages = 563-5 | month = Oct | year = 2006 | doi = | PMID = 17183856 }}</ref>
| |
| **It has been suggested they are distinct from teratomas.<ref>{{Cite journal | last1 = Basu | first1 = A. | last2 = Jagdish | first2 = S. | last3 = Iyengar | first3 = KR. | last4 = Basu | first4 = D. | title = Fetus in fetu or differentiated teratomas? | journal = Indian J Pathol Microbiol | volume = 49 | issue = 4 | pages = 563-5 | month = Oct | year = 2006 | doi = | PMID = 17183856 }}</ref>
| |
| ***They could be thought of as a parasitic twin.
| |
|
| |
| Features:
| |
| *Discrete mass consisting of mature tissues that form well-developed structures with the normal anatomical relations.
| |
| **Separated from teratoma by the presence of a vertebral column.<ref name=pmid17334616>{{Cite journal | last1 = Majhi | first1 = AK. | last2 = Saha | first2 = K. | last3 = Karmakar | first3 = M. | last4 = Sinha Karmakar | first4 = K. | last5 = Sen | first5 = A. | last6 = Das | first6 = S. | title = Fetus in fetu--a mystery in medicine. | journal = ScientificWorldJournal | volume = 7 | issue = | pages = 252-7 | month = | year = 2007 | doi = 10.1100/tsw.2007.56 | PMID = 17334616 }}</ref>
| |
|
| |
| ===Immature teratoma===
| |
| Features:
| |
| *Immature if neural tissue is present:<ref>RS. 2 May 2010.</ref>
| |
| **Vaguely resembles pseudostratified respiratory epithelium.
| |
| *Islands of small hyperchromatic cells - "blastema".
| |
| *+/-Cartilage.
| |
| *+/-Adipocytes.
| |
| *+/-Colonic type mucosa.
| |
| *+/-Stratified squamous epithelium (skin).
| |
|
| |
| DDx:<ref>{{Ref BITFS|34}}</ref>
| |
| *[[Cerebellum]].
| |
| *[[Retina]].
| |
|
| |
| =====Images=====
| |
| <gallery>
| |
| Image:Immature_teratoma_high_mag.jpg | Primitive neuroepithelium - high mag. (WC/Nephron)
| |
| Image:Primitive_neuroepithelium_intermed_mag.jpg | Primitive neuroepithelium - intermed mag. (WC/Nephron)
| |
| Image:Teratoma_intermed_mag.jpg | Teratoma - mature components (WC/Nephron)
| |
| </gallery>
| |
| <gallery>
| |
| Image:Teratoma 2 low mag.jpg| Mature teratoma - low mag. (WC/Nephron)
| |
| Image:Teratoma 2 intermed mag.jpg| Mature teratoma - intermed. mag. (WC/Nephron)
| |
| Image:Teratoma 2 high mag.jpg| Mature teratoma - high mag. (WC/Nephron)
| |
| </gallery>
| |
|
| |
| Other images:
| |
| *[http://www.webpathology.com/image.asp?n=5&Case=35 Immature teratoma - myxomatous stroma (webpathology.com)].
| |
| *[http://www.webpathology.com/image.asp?n=6&Case=35 Immature teratoma - blastema (webpathology.com)].
| |
| *[http://www.webpathology.com/image.asp?n=7&Case=35 Immature teratoma - primitive neuroepithelium (webpathology.com)].
| |
| *[http://moon.ouhsc.edu/kfung/jty1/opaq/PathQuiz/N0C001-PQ01-M.htm Immature teratoma - primitive neuroepithelium (ouhsc.edu)].
| |
|
| |
| ====Grading (immature)====
| |
| Based on quantity of immature neuroepithelium:<ref name=pmid17080330>{{cite journal |author=Harms D, Zahn S, Göbel U, Schneider DT |title=Pathology and molecular biology of teratomas in childhood and adolescence |journal=Klin Padiatr |volume=218 |issue=6 |pages=296–302 |year=2006 |pmid=17080330 |doi=10.1055/s-2006-942271 |url=}}</ref><ref name=pmid15761467>{{cite journal |author=Ulbright TM |title=Germ cell tumors of the gonads: a selective review emphasizing problems in differential diagnosis, newly appreciated, and controversial issues |journal=Mod. Pathol. |volume=18 Suppl 2 |issue= |pages=S61–79 |year=2005 |month=February |pmid=15761467 |doi=10.1038/modpathol.3800310 |url=http://www.nature.com/modpathol/journal/v18/n2s/full/3800310a.html}}</ref><ref name=pmid7814189>{{cite journal |author=O'Connor DM, Norris HJ |title=The influence of grade on the outcome of stage I ovarian immature (malignant) teratomas and the reproducibility of grading |journal=Int. J. Gynecol. Pathol. |volume=13 |issue=4 |pages=283–9 |year=1994 |month=October |pmid=7814189 |doi= |url=}}</ref>
| |
| *G0 - mature teratoma; no immature neuroepithelium.
| |
| *G1 - less than one lower power field ([[LPF]]) of immature neuroepithelium; LPF defined field at 4X magnification.
| |
| *G2 - 1-3 LPFs.
| |
| *G3 - more than 3 LPFs.
| |
|
| |
| Note:
| |
| *LPF not adequately defined - see [[LPFitis]]. Same BS as HPF.
| |
|
| |
| ====IHC (immature)====
| |
| Features:
| |
| *Primitive neuroepithelium:<ref name=pmid11598856>{{cite journal |author=Craver RD, Lipscomb JT, Suskind D, Velez MC |title=Malignant teratoma of the thyroid with primitive neuroepithelial and mesenchymal sarcomatous components |journal=Ann Diagn Pathol |volume=5 |issue=5 |pages=285–92 |year=2001 |month=October |pmid=11598856 |doi=10.1053/adpa.2001.27918 |url=}}</ref>
| |
| **Neuron-specific enolase (NSE) +ve.
| |
| **Neuron-specific B tubulin +ve.
| |
| **Synaptophysin +ve.
| |
|
| |
| ===Monodermal teratomas===
| |
| ====Struma ovarii====
| |
| Features:
| |
| *Thyroid tissue present - colloid is seen.
| |
| **May develop pathologies seen in the [[thyroid gland]], e.g. [[papillary thyroid carcinoma]].
| |
|
| |
| =====Images=====
| |
| <gallery>
| |
| Image:Struma_ovarii_-_low_mag.jpg | Struma ovarii - low mag. (WC/Nephron)
| |
| Image:Struma_ovarii_-_high_mag.jpg | Struma ovarii - high mag. (WC/Nephron)
| |
| </gallery>
| |
| ====Strumal carcinoid====
| |
| Features:<ref name=pmid18509188>{{Cite journal | last1 = Gorin | first1 = I. | last2 = Sastre-Garau | first2 = X. | title = Strumal carcinoid tumor of the ovary. | journal = J Clin Oncol | volume = 26 | issue = 16 | pages = 2780-1 | month = Jun | year = 2008 | doi = 10.1200/JCO.2008.16.1620 | PMID = 18509188 }}</ref><ref>{{Cite journal | last1 = Tamsen | first1 = A. | last2 = Mazur | first2 = MT. | title = Ovarian strumal carcinoid in association with multiple endocrine neoplasia, type IIA. | journal = Arch Pathol Lab Med | volume = 116 | issue = 2 | pages = 200-3 | month = Feb | year = 1992 | doi = | PMID = 1346363 }}</ref>
| |
| *Has components that suggest:
| |
| *#Carcinoid ([[neuroendocrine tumour]]).
| |
| *#*Nuclei with stippled chromatin (salt-and-pepper chromatin).
| |
| *#[[Thyroid]] - cystic spaces/follicular-like structures.
| |
|
| |
| =====Images=====
| |
| <gallery>
| |
| Image:Strumal_carcinoid_-_intermed_mag.jpg | Strumal carcinoid - intermed. mag. (WC/Nephron)
| |
| Image:Strumal_carcinoid_-_high_mag.jpg | Strumal carcinoid - high mag. (WC/Nephron)
| |
| </gallery>
| |
| ==Gonadoblastoma== | | ==Gonadoblastoma== |
| ===General===
| | {{Main|Gonadoblastoma}} |
| *Associated with abnormal sexual development.
| |
| *Often coexist with a [[dysgerminoma]].
| |
| *A mixed tumour that consists of (1) primitive germ cells and (2) sex cord elements.
| |
|
| |
|
| ===Gross===
| |
| *+/-Cystic.
| |
|
| |
| ===Microscopic===
| |
| Features:<ref name=Ref_PBoD1104>{{Ref PBoD|1104}}</ref>
| |
| *Immature germ cells resembling Sertoli cells or granulosa cells.
| |
| **Sertoli cells = moderate cytoplasm in a trabecular or tubular architecture.
| |
| **Granulosa cells = form follicle-like structures.
| |
| ***May form nests.
| |
| *Primitive germ cells resemble those of a [[dysgerminoma]].
| |
| **Polygonal cells with a central nucleus, squared-off nuclear membrane and clear cytoplasm.
| |
| *+/-Calcification (very common).
| |
| *+/-Eosinophilic basement membrane material between the (primitive) germ cells and support cells.<ref>URL: [http://www.flickr.com/photos/ckrishnan/3972432044/in/photostream/ http://www.flickr.com/photos/ckrishnan/3972432044/in/photostream/]. Accessed on: 11 September 2011.</ref>
| |
|
| |
| ====Images====
| |
| www:
| |
| *[http://www.webpathology.com/image.asp?n=40&Case=532 Gonadoblastoma - low mag. (webpathology.com)].
| |
| *[http://www.webpathology.com/image.asp?case=532&n=42 Gonadoblastoma - high mag. (webpathology.com)].
| |
| *[http://www.webpathology.com/image.asp?case=532&n=44 Gonadoblastoma - high mag. (webpathology.com)].
| |
| *[http://www.flickr.com/photos/ckrishnan/3972431774/in/photostream/ Gonadoblastoma - low mag. (flickr.com)].
| |
| *[http://www.flickr.com/photos/ckrishnan/3972432404/in/photostream/ Gonadoblastoma - intermed. mag. (flickr.com)].
| |
| *[http://www.flickr.com/photos/ckrishnan/3972432044/in/photostream/ Gonadoblastoma - high mag. (flickr.com)].
| |
| *[http://path.upmc.edu/cases/case356.html Gonadoblastoma - several cases (upmc.edu)].
| |
| <gallery>
| |
| Image:Gonadoblastoma_-_intermed_mag.jpg | Gonadoblastoma - intermed. mag. (WC/Nephron)
| |
| Image:Gonadoblastoma_-_b_-_high_mag.jpg | Gonadoblastoma - high mag. (WC/Nephron)
| |
| </gallery>
| |
| ==Polyembryoma== | | ==Polyembryoma== |
| ===General===
| | {{Main|Polyembryoma}} |
| *Poor prognosis.
| |
| *Almost never in pure form, i.e. usu. a component of a [[mixed germ cell tumour]].<ref>{{Cite journal | last1 = Young | first1 = RH. | title = Testicular tumors--some new and a few perennial problems. | journal = Arch Pathol Lab Med | volume = 132 | issue = 4 | pages = 548-64 | month = Apr | year = 2008 | doi = 10.1043/1543-2165(2008)132[548:TTNAAF]2.0.CO;2 | PMID = 18384207 }}</ref>
| |
| | |
| ===Microscopic===
| |
| Features:
| |
| *Disc shaped structure (embryo-like) with:
| |
| **The one side endoderm.
| |
| ***Skin/CNS.
| |
| **The other side ectoderm.
| |
| ***Internal organs - GI tract.
| |
| | |
| Images:
| |
| *[http://www.webpathology.com/image.asp?case=37&n=6 Polyembryoma - low mag. (webpathology.com)].
| |
| *[http://www.webpathology.com/image.asp?n=7&Case=37 Polyembryoma - high mag. (webpathology.com)].
| |
|
| |
|
| ==Mixed germ cell tumour== | | ==Mixed germ cell tumour== |
| ===General===
| | {{Main|Mixed germ cell tumour}} |
| *60% of GCTs are mixed.
| |
| | |
| Common combinations:
| |
| # Teratoma + embryonal carcinoma + endodermal sinus tumour (yolk sac tumour) (TEE).
| |
| # Seminoma + embryonal (SE).
| |
| # Teratoma + embryonal +(TE).
| |
| | |
| Memory device: ''TEE'' + all combinations have embryonal carcinoma.
| |
| ===Microscopic===
| |
| Features:
| |
| *Depends on components.
| |
| | |
| Notes:
| |
| *If one cannot identify the component... it is probably yolk sac as this has so many different patterns.
| |
| | |
| ====Images====
| |
| <gallery>
| |
| Image:Mixed_germ_cell_tumour_-_intermed_mag.jpg | Mixed GCT - intermed mag. (WC/Nephron)
| |
| Image:Mixed germ cell tumour - high mag.jpg | Mixed GCT - high mag. (WC/Nephron)
| |
| </gallery>
| |
| www:
| |
| *[http://path.upmc.edu/cases/case192/micro.html Mixed germ cell tumour - several images (upmc.edu)].
| |
| *[http://path.upmc.edu/cases/case356.html Mixed germ cell tumour - several cases (upmc.edu)].
| |
| | |
| ===IHC===
| |
| *Beta-hCG +ve - if syncytiotrophoblasts are present.
| |
| *AFP +ve - a yolk sac tumour component is present.
| |
| *GFAP +ve - if neuroepithelium is present.
| |
|
| |
|
| ==See also== | | ==See also== |
| Line 502: |
Line 177: |
| *[[Ovarian tumours]]. | | *[[Ovarian tumours]]. |
| *[[Trophoblast]]. | | *[[Trophoblast]]. |
| | *[[Sex cord-stromal tumours]]. |
|
| |
|
| ==References== | | ==References== |
| Line 508: |
Line 184: |
| [[Category:Gynecologic pathology]] | | [[Category:Gynecologic pathology]] |
| [[Category:Genitourinary pathology]] | | [[Category:Genitourinary pathology]] |
| | [[Category:Germ cell tumours|Germ cell tumours]] |
.jpg)












{kind=link}