Difference between revisions of "An introduction to head and neck pathology"
m (w) |
|||
| Line 206: | Line 206: | ||
==Squamous papilloma== | ==Squamous papilloma== | ||
:''Laryngeal papilloma'' redirects here. | :''Laryngeal papilloma'' redirects here. | ||
:Caruncle lesion is dealt with in ''[[papilloma of the caruncle]]''. | |||
===General=== | ===General=== | ||
*Benign. | *Benign. | ||
Revision as of 14:35, 29 August 2013
Head and neck pathology is squamous cell carcinoma and weird stuff. The thyroid is dealt with in its own article, as is pathology of the salivary gland.
Cytopathology of the head and neck is dealt with in a separate article called head and neck cytopathology.
Clinical
Common lesions:[1]
- Leukoplakia.
- Homogeneous.
- Non-homogeneous.
- Erythroplakia - more worrisome for cancer than leukoplakia.
Leukoplakia
- Hairy leukoplakia is dealt with in a separate section
General
- Non-specific clinical finding - may be benign or malignant.
- Associated with tobacco use.[2]
Risk of malignancy:
- In twos series ~13% were associated with an invasive lesion.[3][4]
- Non-homogenous leukoplakia has a greater risk of malignancy than homogenous.[4]
- Location matters - floor of mouth and ventral tongue lesions higher risk for malignancy.[5]
Gross
- White lesion - may be subdivided:
- Non-homogenous.
- Homogenous.
Microscopic
Features:[1]
- Often associated with epithelial thickening (hyperkeratosis, acanthosis).
DDx:
- Food debris.
- Oral candidiasis.
- Lichen planus.
- Benign alveolar ridge keratosis (oral lichen simplex chronicus).[6]
- Squamous cell carcinoma of the head and neck.
- Others - see Dermatopathology#Leukoplakia.
Erythroplakia
General
- Non-specific clinical finding - may be benign or malignant.
- Strong association with non-keratinizing squamous lesions (invasive and dysplastic).
Microscopic
Features:[1]
- Unidentified red lesion.
- Often erosion.
Overview
Cysts
- Rathke cleft cyst - nasal cavity.
- Thyroglossal duct cyst - midline, neck.
- Branchial cleft cyst - lateral neck.
Larynx
Oral
Infectious:
Nasal cavity/nose
- Rhinoscleroma.
- Nasal glial heterotopia.[7]
Benign cystic lesions
- Cytology dealt with in Head and neck cytopathology.
Cystic lesions - overview
Lateral cystic lesions:
Medial cystic lesions:
Lateral & medial lesions:
- Epidermoid cyst.
- Cystic squamous cell carcinoma.
Rathke cleft cyst
- Main article: Rathke cleft cyst
- Arises from intermediate lobe - embryonic remnant.
- Benign cystic lesion without calcification.
- Related to craniopharyngioma.
Thyroglossal duct cyst
General
- Congenital.
- Midline.
Treatment:
- Surgical excision (with piece of hyoid bone).
Microscopic
Features:
- Cyst.
- Lining:
- Squamous or respiratory epithelium.
- Cyst contents: debris.
- Lining:
- +/-Thyroid gland.
- +/-Granulomatous inflammation (phagocytosis of debris).
Images:
Branchial cleft cyst
- AKA branchial cleft remnant.
General
- Benign congenital thingy in the lateral neck.[9]
- Most common cystic neck lesion in young adults.[10]
- Treatment: excision.
Gross
- Lateral neck mass.
Image - clinical:
Microscopic
Features:
- Cystic space lined by squamous epithelium - usually.
- +/-Inflammation.
- Connective tissue:
- +/-Adipose tissue.
- +/-Cartilage.
- +/-Bone.
- +/-Muscle.
DDx:
- Cystic squamous cell carcinoma - may be deceptively benign appearing.[10]
Image:
IHC
- p16 -ve.
- May be done to exclude a HPV-associated head and neck squamous cell carcinoma.
- Ki-67 low.
Benign lymphoepithelial lesion
- AKA benign lymphoepithelial cyst
General
- Usually parotid gland.
- Associated with autoimmune disease, e.g. Sjoegren disease, may not remain benign.[12]
Microscopic
Features:
- Lymphocytes.
- Ductal epithelial cells.[13]
Note:
- Must rule-out (MALT) lymphoma.
IHC
- CD20, CD3 -- mixed population.
- Kappa ~ lambda.
Other benign
Vocal cord nodule
General
- Benign.
- AKA singer's nodule.
- Etiology: overuse, mechanical trauma (?).
Microscopic
Features:[14]
- Early:
- Edema.
- Fibroblasts proliferation.
- Late:
- Subepithelial hyaline / stromal hyaline.
- Blood vessels - dilated.
Notes:
- No inflammation.
DDx:[15]
- Amyloidosis.
- Granular cell tumour.
- Spindle cell squamous cell carcinoma.
- Myxoma.
- Ductal-type cyst.
Images:
Sign out
VOCAL CORD LESION, EXCISION: - STRATIFIED SQUAMOUS EPITHELIUM WITH PARAKERATOSIS AND SUBEPITHELIAL HYALINE MATERIAL, CONSISTENT WITH WITH VOCAL CORD NODULE OR POLYP. - NEGATIVE FOR MALIGNANCY.
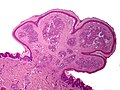
Squamous papilloma
- Laryngeal papilloma redirects here.
- Caruncle lesion is dealt with in papilloma of the caruncle.
General
- Benign.
- Typically related to HPV 6 and HPV 11.
Gross
Features:[16]
- Exophytic mass.
Microscopic
Features:[16]
- Branching papillae.
- Papilla = nipple-like projection with a fibrovascular core.
- Basal cell hyperplasia.
- Koilocytes.
Note:
- The threshold for dysplasia is somewhat higher in the head and neck than in the uterine cervix.
DDx:
- Squamous cell carcinoma of the head and neck - verrucous, papillary and exophytic subtypes.
- Verruca vulgaris - have granular layer, hyperkeratosis and parakeratosis.[17]
- Oral condyloma - broader projections with a blunted appearance.[17]
Images:
- Laryngeal papilloma - low mag. (webpathology.com).
- Laryngeal papilloma - high mag. (webpathology.com).
- Low-grade squamous dysplasia (els-cdn.com).[18]
Sign out
LARYNGEAL LESION ("LARYNGEAL PAPILLOMA"), RIGHT, BIOPSY:
- SQUAMOUS PAPILLOMA.
Not definite
TONGUE PAPULE, RIGHT, BIOPSY: - SQUAMOUS EPITHELIUM WITH PARAKERATOSIS AND VERY SCANT STROMA WITH FEATURES SUGGESTIVE OF A SQUAMOUS PAPILLOMA. - NEGATIVE FOR DYSPLASIA AND NEGATIVE FOR MALIGNANCY.
Dysplastic
LARYNGEAL LESION ("LARYNGEAL PAPILLOMA"), LEFT, BIOPSY:
- SQUAMOUS PAPILLOMA WITH LOW-GRADE DYSPLASIA.
- NEGATIVE FOR HIGH-GRADE DYSPLASIA AND NEGATIVE FOR MALIGNANCY.
- CLOSE FOLLOW-UP IS RECOMMENDED.
Micro
The sections show fibrovascular cores covered by stratified squamous epithelium with basal cell hyperplasia and edema. Scattered lymphocytes are present in the epithelium. No mitotic activity is appreciated. There is no significant nuclear atypia. Dyskeratotic cells are seen focally. Parakeratosis is present. Koilocytes are not apparent.
Low-grade dysplasia
The sections show fibrovascular cores covered by stratified squamous epithelium. Scattered lymphocytes are present in the epithelium. Rare mitotic activity is appreciated in the lower third of the epithelium. Mild nuclear atypia (hyperchromasia and mild nuclear enlargement in the lower third of the epithelium) is present. Dyskeratotic cells are seen focally. Parakeratosis is present. Koilocytes are seen focally.
Pemphigus vulgaris
- AKA pemphigus.
- Should not be confused with bullous pemphigoid (which is less serious).
General
- May lead to blindness.
- Oral lesion is classically: first to show & last to go.
- Oral lesions usually precede the skin lesions.
Etiology:
- Autoimmune disease.
- Antibodies against: desmoglein 1, desmoglein 3.
Microscopic
Features:[19]
- Suprabasilar blistering.
DDx: Hailey-Hailey disease.
Pyogenic granuloma
General
- Sometimes pregnancy tumour.
- Seen in children, young adults, pregnant women.
Clinical:
- May grow quickly - clinically suspicious for a malignancy.
Notes:
- Name of entity is a misnomer:
- Not pyogenic, i.e. infectious.
- Not granulomatous.
- The WMSP advocates the name lobular capillary hemangioma.[21]
Gross
Features:[22]
- Erythematous.
- Hemorrhagic.
Usually location:[21]
- Lips.
- Tongue.
- Gingiva.
Microscopic
Features:[23]
- Polypoid or peduculated.
- Vascular, i.e. many blood vessels, with plump endothelium.
- Usu. thinned epithelium[24] or ulcerated.[21]
- Lobular arrangement of vascular (seen at low power).[25]
DDx:
Why it is not...
- Glomus tumour - cookie cutter arrangement of cells.
Image
Pyogenic granuloma. (WC)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg?uselang=en){kind=link}
.jpg?uselang=en){kind=link}
{kind=link}
www:
IHC
Features - positive for vascular markers:[21]
- CD34 +ve.
- CD31 +ve.
- Factor VIII +ve.
Sign out
TONGUE, LEFT LATERAL, BIOPSY: - LOBULAR CAPILLARY HEMANGIOMA (PYOGENIC GRANULOMA).
Micro
The sections shows a pendunculated vascular lesion with small capillaries arranged in a lobular fashion. The endothelial cells of the lesion show no atypia. The overlying acanthotic epidermis has hyperkeratosis and hypergranulosis, and is focally ulcerated and impetiginized. There is no significant keratocyte atypia. No melanocytic nests are seen. The dermis has a mild perivascular lymphoplasmacytic infiltrate. The lesion is excised in the plane of section.
Plummer-Vinson syndrome
Triad:[22]
- Iron-deficiency anemia.
- Glossitis.
- Esophageal dysphagia (usually related to webs).
Rhinoscleroma
General
- Caused by Klebsiella rhinoscleromatis.
- Nose involved +95% of the time.[27]
Gross
- Nasal mass - may be deforming.
Image:
{kind=link}
Microscopic
Features:[28]
- Macrophages - clear-to-foamy cytoplasm.
- Lymphocytes.
- Plasma cells.
DDx:
Images:
- WC:
- www:
{kind=link}
{kind=link}
{kind=link}
Stains
- Warthin-Starry stain +ve (rod-shaped organisms).
- Dieterle stain +ve (rod-shaped organisms).
Neoplasms
Odontogenic tumours and cysts
This is a rather large topic and dealt with in a separate article.
It includes:
- Keratocystic odontogenic tumour.
- Radicular cyst.
- Dentigerous cyst.
- Ameloblastoma.
- Adenomatoid odontogenic tumour.
- Ameloblastic fibroma.
- Odontogenic myxoma.
Pharyngeal/nasopharyngeal specimens
- Specimens may be challenging to interpret as there is normally an abundance of lymphoid cells.
- Malignant tissue can look benign.[30]
- May be difficult to differentiate from other malignancies.
Histology
- Upper airway distant from areas with friction: respiratory type epithelium.
Work-up of negative H&E Bx differs by site:
- Sunnybrook:[31]
- LMWK (CAM5.2).
- pankeratin (AE1/AE3).
- UHN.
- Nothing.
Laryngeal neoplasms
These are dealt with in a separate article.
Human papillomavirus-associated head and neck squamous cell carcinoma
- Abbreviated HPV-HNSCC.
General
- Tumours associated with high risk HPV, typically HPV 16.[32]
- Lesions more radiosensitive and usually have a better prognosis.[32]
Gross
Classic locations:
- Tonsil and base of tongue[35] (palatine tonsil, lingual tonsil, oropharynx).
Note:
- Memory device:
- Where the tip of the penis goes when someone is deep throating.
Microscopic
Features:[36]
- Typically non-keratinizing squamous cell carcinoma.
DDx:
- HPV-negative squamous cell carcinoma.
Images:
IHC
- p16 +ve.[35]
- EBER -ve.
Sinonasal undifferentiated carcinoma
- Abbreviated SNUC
General
- Aggressive/poor prognosis.
Microscopic
Features:[39]
- Architecture: nested, trabecular or lobular.
- Distinct cellular borders.
- Small-to-moderate cytoplasm.
- +/-Distinct nucleoli.
- Tumour cell size variable (small to large).
Note:
- Glandular and squamous differentiation are absent by definition.[40]
Images:
- www:
- WC:
{kind=link}
{kind=link}
{kind=link}
IHC
Features:[39]
- Pankeratin +ve.
- EMA +ve.
- CK7 +ve.
- CK5/6 -ve.
Others:
- NSE +ve/-ve.
- Chromogranin A -ve.
- Synaptophysin -ve.
- p63 +ve/-ve.[41]
Nasopharyngeal carcinoma
- Abbreviated NPC.
General
- "Nasopharyngeal carcinoma" is the name of an entity - it is not a descriptive term.
- Strong association with Epstein-Barr virus (EBV).
Note:
- A morphologically identical tumour elsewhere is called lymphoepithelioma-like carcinoma.
Gross
- Nasopharynx - as the name would suggest.
Microscopic
Features:[42]
- Prominent lymphoid component - key feature.
- Features of squamous cell carcinoma:
- Cohesive cells with:
- Abundant dense eosinophilic cytoplasm.
- Central nuclei +/- small/indistinct nucleoli.
- Cohesive cells with:
Images:
- Nasopharyngeal carcinoma - in a LN - low mag. (WP).
- Nasopharyngeal carcinoma - in a LN - intermed. mag. (WC).
- Nasopharyngeal carcinoma - in a LN - high mag. (WP).
{kind=link}
{kind=link}
{kind=link}
Histologic subclassification
World Health Classification (2005) for NPC:[43]
| Type | Histology | Description | EBV | Prevalence | Prognosis |
|---|---|---|---|---|---|
| 1 | keratinizing SCC | graded poorly-well-diff. | -ve | ? | bad |
| 2a | nonkeratinizing carcinoma, differentiated | well def. cell borders & tumour nest borders, mimics appearance of UCC | +ve | ? | good |
| 2b | nonkeratinizing carcinoma, undifferentiated | sheets/syncytial, vescicular nuclei, prominent nucleoli, pink cytoplasm | ? | most common | ? |
| 3 | basaloid SCC | mimics BCC - see basaloid SCC | ? | least common | ? |
How to remember KNUB:
- Keratinizing, Non-keratinizing diff., non-keratinizing Undiff., Basaloid SCC.
IHC
- EBER +ve.
- p16 -ve.[44]
Notes:
Squamous lesions
- Premalignant lesions
- Mild dysplasia.
- Low risk of progression to invasive lesions.
- Moderate dysplasia.
- Severe dysplasia/carcinoma in situ (CIS).
- Histologically severe dysplasia and CIS cannot be differentiated reliably; ergo, there can be considered the same thing.
- Severe dysplasia is not a necessary intermediate for cancer, i.e. invasive squamous cell carcinoma may be present with moderate dysplasia.
- Mild dysplasia.
- Invasive squamous cell carcinoma (SCC).
- "Microinvasive" squamous cell carcinoma - term should be avoided as there is no concenus on what it means.
- There are several subtypes of SCC.
Squamous dysplasia of the head and neck
General
- Similar to squamous dysplasia elsewhere.
Sign out
PHARYNGEAL WALL, POSTERIOR, BIOPSY: - SQUAMOUS MUCOSA WITH MILD SQUAMOUS DYSPLASIA. - NEGATIVE FOR MALIGNANCY.
Squamous cell carcinoma of the head and neck
General
- Most common malignant tumour of the head & neck.
- Most common spindle cell tumour of the head & neck.
Microscopic
Classification
SCC is subdivided by the WHO into:[46]
- Keratinizing type (KT).
- Worst prognosis.
- Undifferentiated type (UT).
- Intermediate prognosis.
- EBV association.
- Nonkeratinizing type (NT).
- Good prognosis.
- EBV association.
Features based on classification:[46]
- KT subtype:
- Keratinization & intercellular bridges through-out most of the malignant lesion.
- UT:
- Non-distinct borders/syncytial pattern.
- Nucleoli.
- NT:
- Well-defined cell borders.
Invasion
Features:
- Eosinophilia.
- Extra large nuclei/bizarre nuclei.
- Inflammation (lymphocytes, plasma cells).
- Long rete ridges.
- Numerous beeds/blobs of epithelial cells that seem unlikely to be rete ridges.
Pitfalls:
- Tangential cuts.
- If you can trace the squamous cells from a gland to the surface it is less likely to be invasive cancer.
Notes on invasion:
- Nice review paper by Wenig.[47]
- See SCC of the cervix versus CIN III.
Image(s):
_squamous_cell_carcinoma_histopathology.jpg?uselang=de){kind=link}
Overview of subtypes
There are several subtypes:[48]
- Basaloid - poor prognosis, usu. diagnosed by recognition of typical SCC.
- Warty (Condylomatous).
- Verrucous - good prognosis, rare.
- Papillary.
- Lymphoepithelial, rare.
- Spindle cell, a common spindle cell lesion of the H&N.
Verrucous squamous cell carcinoma
Features:
- Exophytic growth.
- Well-differentiated.
- "Glassy" appearance.
- Pushing border.
DDx: papilloma.
Spindle cell squamous carcinoma
- Key to diagnosis is finding a component of conventional squamous cell carcinoma.
IHC:
- Typically keratin -ve.
- p63 +ve.
DDx:
- Spindle cell melanoma.
- Mesenchymal neoplasm.
Basaloid squamous cell carcinoma
- May mimic adenoid cystic carcinoma.
- Classically base of tongue.[49]
- Typically poor prognosis.
Features:
- Need keratinization. (???)
DDx:
- Neuroendocrine tumour.
Lymphoepithelial (squamous cell) carcinoma
- Rare.
- +/-EBV.
Small cell anaplastic carcinoma
- Rare.
DDx:
- Metastatic small cell carcinoma of the lung.
Granular cell tumour
General
- May mimic (well-differentiated) squamous cell carcinoma - histopathologically.
- There is a well-described phenomenon called pseudoepitheliomatous hyperplasia.[50]
- Usually a benign tumour.
Microscopic
Features:
- Large polygonal cells with abundant (eosinophilic) granular cytoplasm.
Image:
{kind=link}
Olfactory neuroblastoma
- See also: neuroblastoma.
- AKA esthesioneuroblastoma.
General
Epidemiology:[51]
- Prognosis: poor.
- Wide age range with bimodal distribution - teens and 60s.
- No sex predilection.
Clinical presentation:[51]
- Nasal obstruction ~ 70%.
- Epistaxis ~ 50%.
- Anosmia.
- Headache.
Gross
- Arises from olfactory mucosa - upper nasal cavity.[52]
Microscopic
Features:[51]
- Small round (blue) cell tumour with:
- Stippled chromatin.
- High NC ratio.
- +/-Flexner-Wintersteiner rosette - rosette with empty centre (donut hole).
- +/-Fibrillary, eosinophilic material (neuropil-like).[52]
DDx:
- Lymphoma.
- Small cell carcinoma.
- Other small round cell tumours.
- Basaloid squamous carcinoma.[citation needed]
Images:
{kind=link}
IHC
- S100:
- Sustentacular cells +ve.
- Small round cells -ve.
- Neuroendocrine markers +ve (CD56, synaptophysin).
Others:
Craniopharyngioma
- Cystic lesion +/- calcifications +/-squamous nests.
- Related to Rathke cleft cyst.
Nasopharyngeal angiofibroma
- See also: Angiofibroma.
- AKA juvenile nasopharyngeal angiofibroma.
General
- Classically adolescent males with recurrent nose bleeds.
Microscopic
Features:[54]
- Fibroblastic cells with plump (near cuboidal) nuclei.
- Fibrous stroma.
- Abundant capillaries.
Images:
{kind=link}
{kind=link}
Nasal polyps
Overview
DDx (benign - multiple):[55]
- Autoimmune/idiopathic:
- Asthma.
- Allergic rhinitis.
- Churg-Strauss syndrome (AKA allergic granulomatous angiitis).
- Features: asthma, eosinophilia, granulomatous inflammation, necrotizing systemic vasculitis, and necrotizing glomerulonephritis.[56]
- Nonallergic rhinitis with eosinophilia syndrome (NARES).
- Infectious:
- Fungal infection (with allergic component - AFS = allergic fungal sinusitis).
- Chronic rhinosinusitis.
- Genetic:
- Primary ciliary dyskinesia.
- Cystic fibrosis.
- Associations:
- Alcohol intolerance ~ 50%.
- Aspirin intolerance - upto ~ 25%.
- Tumours:
- Juvenile nasopharyngeal angiofibroma - young males.
- Nasopharyngeal carcinomas.
- Sarcomas.
- Hemangioma.
- Schneiderian papilloma.
- Other.
Memory devices:
- GAIT = Genetic, Allergic/idiopathic, Infectious, Tumours.
- Allergic causes As - allergic, asthma, allergic granulomatous angiitis (Churg-Strauss syndrome), nonallergic rhinitis with eosinophilia.
Epidemiology
- More commonly assoc. with nonallergic conditions.[55]
Treatment
- Recurrent polyps: functional endoscopic sinus surgery (FESS).
Inflammatory polyps with neutrophils
General
- Histologic findings are non-specific; DDx includes:[57]
- Cystic fibrosis.
- Primary ciliary dyskinesia syndrome.
- Young syndrome
Microscopic
Features:
- Neutrophil predominant.
- Edema.
- +/-Mucus-impaction (dilated glands with mucus).
- Suggestive of cystic fibrosis.[58]
Sign out
A. Nasal sinus tissue, right, excision: - Inflamed edematous sinonasal mucosa with abundant neutrophils. - Negative for malignancy. B. Nasal sinus tissue, left, excision: - Inflamed edematous sinonasal mucosa with abundant neutrophils and fragments of bone. - Negative for malignancy.
Allergic nasal polyp
General
- People with allergies.
- Same type of polyps seen in those without allergies.[59]
Gross
- Polypoid mass - several millimetres to centimetres in size.
- Translucent.[citation needed]
Microscopic
Features:[60]
- Normal respiratory epithelium.
- Stroma with:
- Edema.
- Eosinophils.
- +/-Other inflammatory cells (plasma cells, lymphocytes, neutrophils).
DDx:
- Inflammatory nasal polyp with abundant neutrophils.
- Vasculitis.
Sign out
A. Nasal sinus tissue, right, excision: - Inflamed edematous sinonasal mucosa with abundant eosinophils. - Negative for malignancy. B. Nasal sinus tissue, left, excision: - Inflamed edematous sinonasal mucosa with abundant eosinophils and fragments of bone. - Negative for malignancy.
A. NASAL SINUS TISSUE, RIGHT, EXCISION: - INFLAMED EDEMATOUS SINONASAL MUCOSA WITH ABUNDANT EOSINOPHILS. - NEGATIVE FOR MALIGNANCY. B. NASAL SINUS TISSUE, LEFT, EXCISION: - INFLAMED EDEMATOUS SINONASAL MUCOSA WITH ABUNDANT EOSINOPHILS AND FRAGMENTS OF BONE. - NEGATIVE FOR MALIGNANCY.
Tonsillar lymphangiomatous polyp
Microscopic
Features:[61]
- Polyp with lymph channels.
Schneiderian papilloma
General
- Lumpers vs. splitters debate about whether it is one entity or three.[63]
- Inverted (Schneiderian) - most common ~60-65%.
- Fungiform (Schneiderian) - less common ~30-35%.
- Oncocytic (Schneiderian) - least common ~5%.
Inverted
- AKA inverted papilloma.[64]
- Usually lateral wall (as the septum as little soft tissue to grow into).[63]
- May transform to carcinoma.
Fungiform
Oncocytic
Microscopic
Inverted Schneiderian papilloma
Features:[63]
- Well-demarcated epithelial islands in the stroma.
- Squamous +/-surface keratinization or respiratory type epithelium (with cilia).
- +/-Neutrophils.
- +/-Goblet cells.
Notes:
- May mimic invasive SCC.
Images:
- Inverted papilloma & verrucous carcinoma (upmc.edu).
- Schneiderian papilloma - very low mag. (WC).
- Schneiderian papilloma - very high mag. (WC).
{kind=link}
{kind=link}
Fungiform Schneiderian papilloma
Features:
- Exophytic growth pattern - key feature.
Oncocytic Schneiderian papilloma
Features:
- Oncocytes - key feature.
- Exophytic or endophytic growth pattern.
See also
References
- ↑ 1.0 1.1 1.2 Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 780. ISBN 0-7216-0187-1.
- ↑ Bánóczy, J.; Gintner, Z.; Dombi, C. (Apr 2001). "Tobacco use and oral leukoplakia.". J Dent Educ 65 (4): 322-7. PMID 11336117.
- ↑ Lan, AX.; Guan, XB.; Sun, Z. (Jun 2009). "[Analysis of risk factors for carcinogenesis of oral leukoplakia].". Zhonghua Kou Qiang Yi Xue Za Zhi 44 (6): 327-31. PMID 19953947.
- ↑ 4.0 4.1 Lee, JJ.; Hung, HC.; Cheng, SJ.; Chen, YJ.; Chiang, CP.; Liu, BY.; Jeng, JH.; Chang, HH. et al. (Apr 2006). "Carcinoma and dysplasia in oral leukoplakias in Taiwan: prevalence and risk factors.". Oral Surg Oral Med Oral Pathol Oral Radiol Endod 101 (4): 472-80. doi:10.1016/j.tripleo.2005.07.024. PMID 16545712.
- ↑ Sciubba, JJ. (1995). "Oral leukoplakia.". Crit Rev Oral Biol Med 6 (2): 147-60. PMID 7548621.
- ↑ Natarajan, E.; Woo, SB. (Jan 2008). "Benign alveolar ridge keratosis (oral lichen simplex chronicus): A distinct clinicopathologic entity.". J Am Acad Dermatol 58 (1): 151-7. doi:10.1016/j.jaad.2007.07.011. PMID 18158926.
- ↑ Penner, CR.; Thompson, L. (Dec 2003). "Nasal glial heterotopia: a clinicopathologic and immunophenotypic analysis of 10 cases with a review of the literature.". Ann Diagn Pathol 7 (6): 354-9. PMID 15018118.
- ↑ URL: http://150.59.224.157/pathology/index.php?now_position=1&first_category_id=2&second_category_id=19. Accessed on: 4 February 2011.
- ↑ URL: http://www.childrenshospital.org/az/Site663/mainpageS663P0.html. Accessed on: 15 March 2011.
- ↑ 10.0 10.1 Pietarinen-Runtti, P.; Apajalahti, S.; Robinson, S.; Passador-Santos, F.; Leivo, I.; Mäkitie, AA. (Feb 2010). "Cystic neck lesions: clinical, radiological and differential diagnostic considerations.". Acta Otolaryngol 130 (2): 300-4. doi:10.3109/00016480903127450. PMID 19593684.
- ↑ URL: http://www.pathology.med.ohio-state.edu/residents/InternalGate/Area51/ResidentSlideCollection/RSLdx.asp. Accessed on: 15 March 2011.
- ↑ Goto, TK.; Shimizu, M.; Kobayashi, I.; Chikui, T.; Kanda, S.; Toshitani, K.; Shiratsuchi, Y.; Yoshida, K. (May 2002). "Lymphoepithelial lesion of the parotid gland.". Dentomaxillofac Radiol 31 (3): 198-203. doi:10.1038/sj/dmfr/4600690. PMID 12058269.
- ↑ Metwaly, H.; Cheng, J.; Ida-Yonemochi, H.; Ohshiro, K.; Jen, KY.; Liu, AR.; Saku, T. (Jul 2003). "Vascular endothelial cell participation in formation of lymphoepithelial lesions (epi-myoepithelial islands) in lymphoepithelial sialadenitis (benign lymphoepithelial lesion).". Virchows Arch 443 (1): 17-27. doi:10.1007/s00428-003-0824-0. PMID 12761623.
- ↑ URL: http://www.pathconsultddx.com/pathCon/diagnosis?pii=S1559-8675%2806%2970310-2. Accessed on: 4 February 2011.
- ↑ Thompson, Lester D. R. (2006). Head and Neck Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 9. ISBN 978-0443069604.
- ↑ 16.0 16.1 Thompson, Lester D. R. (2006). Head and Neck Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 33. ISBN 978-0443069604.
- ↑ 17.0 17.1 Thompson, Lester D. R. (2006). Head and Neck Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 426. ISBN 978-0443069604.
- ↑ Hedström, J.; Grenman, R.; Ramsay, H.; Finne, P.; Lundin, J.; Haglund, C.; Alfthan, H.; Stenman, UH. (Oct 1999). "Concentration of free hCGbeta subunit in serum as a prognostic marker for squamous-cell carcinoma of the oral cavity and oropharynx.". Int J Cancer 84 (5): 525-8. PMID 10502732.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1193. ISBN 978-1416031215.
- ↑ Baglin, AC. (Aug 2011). "[Vascular tumors and pseudotumors. Pyogenic granuloma (lobular capillary hemangioma)].". Ann Pathol 31 (4): 266-70. doi:10.1016/j.annpat.2011.05.014. PMID 21839350.
- ↑ 21.0 21.1 21.2 21.3 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 12. ISBN 978-0781765275.
- ↑ 22.0 22.1 Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 776. ISBN 0-7216-0187-1.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 775. ISBN 0-7216-0187-1.
- ↑ URL: http://basicpathology-histopathology.blogspot.com/2009/10/head-and-neck-oral-cavity-reactive_3282.html. Accessed on: 2 February 2011.
- ↑ S. Sade. 8 September 2011.
- ↑ Levy, I.; Rolain, JM.; Lepidi, H.; Raoult, D.; Feinmesser, M.; Lapidoth, M.; Ben-Amitai, D. (Dec 2005). "Is pyogenic granuloma associated with Bartonella infection?". J Am Acad Dermatol 53 (6): 1065-6. doi:10.1016/j.jaad.2005.08.046. PMID 16310070.
- ↑ Chan, TV.; Spiegel, JH. (Oct 2007). "Klebsiella rhinoscleromatis of the membranous nasal septum.". J Laryngol Otol 121 (10): 998-1002. doi:10.1017/S0022215107006421. PMID 17359555.
- ↑ URL: http://www.brown.edu/Courses/Digital_Path/systemic_path/hn/rhinoscleroma2.html. Accessed on: 18 January 2012.
- ↑ URL: http://www.jameswpattersonmd.com/case_studies/index.cfm?CFID=387434. Accessed on: 21 February 2012.
- ↑ S. Raphael. December 2008.
- ↑ S. Raphael. December 2008.
- ↑ 32.0 32.1 Wang, XI.; Thomas, J.; Zhang, S. (Jan 2012). "Changing trends in human papillomavirus-associated head and neck squamous cell carcinoma.". Ann Diagn Pathol 16 (1): 7-12. doi:10.1016/j.anndiagpath.2011.07.003. PMID 22001331.
- ↑ Wittekindt, C.; Wagner, S.; Klussmann, JP. (Sep 2011). "[HPV-associated head and neck cancer. The basics of molecular and translational research].". HNO 59 (9): 885-92. doi:10.1007/s00106-011-2357-1. PMID 21769577.
- ↑ Vourexakis, Z.; Dulguerov, P. (Oct 2011). "[HPV associated head and neck cancers].". Rev Med Suisse 7 (311): 1919-22. PMID 22046680.
- ↑ 35.0 35.1 Heath, S.; Willis, V.; Allan, K.; Purdie, K.; Harwood, C.; Shields, P.; Simcock, R.; Williams, T. et al. (Feb 2012). "Clinically significant human papilloma virus in squamous cell carcinoma of the head and neck in UK practice.". Clin Oncol (R Coll Radiol) 24 (1): e18-23. doi:10.1016/j.clon.2011.05.007. PMID 21752613.
- ↑ Chernock, RD.; El-Mofty, SK.; Thorstad, WL.; Parvin, CA.; Lewis, JS. (Sep 2009). "HPV-related nonkeratinizing squamous cell carcinoma of the oropharynx: utility of microscopic features in predicting patient outcome.". Head Neck Pathol 3 (3): 186-94. doi:10.1007/s12105-009-0126-1. PMC 2811624. PMID 20596971. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2811624/.
- ↑ Pitman, KT.; Costantino, PD.; Lassen, LF. (1995). "Sinonasal undifferentiated carcinoma: current trends in treatment.". Skull Base Surg 5 (4): 269-72. PMC 1656535. PMID 17170968. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1656535/.
- ↑ Al-Mamgani, A.; van Rooij, P.; Mehilal, R.; Tans, L.; Levendag, PC. (Apr 2012). "Combined-modality treatment improved outcome in sinonasal undifferentiated carcinoma: single-institutional experience of 21 patients and review of the literature.". Eur Arch Otorhinolaryngol. doi:10.1007/s00405-012-2008-5. PMID 22476411.
- ↑ 39.0 39.1 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 38. ISBN 978-0781765275.
- ↑ 40.0 40.1 Mills, SE. (Mar 2002). "Neuroectodermal neoplasms of the head and neck with emphasis on neuroendocrine carcinomas.". Mod Pathol 15 (3): 264-78. doi:10.1038/modpathol.3880522. PMID 11904342.
- ↑ Wadsworth, B.; Bumpous, JM.; Martin, AW.; Nowacki, MR.; Jenson, AB.; Farghaly, H. (Dec 2011). "Expression of p16 in sinonasal undifferentiated carcinoma (SNUC) without associated human papillomavirus (HPV).". Head Neck Pathol 5 (4): 349-54. doi:10.1007/s12105-011-0285-8. PMC 3210220. PMID 21805120. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3210220/.
- ↑ Klatt, Edward C. (2006). Robbins and Cotran Atlas of Pathology (1st ed.). Saunders. pp. 145. ISBN 978-1416002741.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 39. ISBN 978-0781765275.
- ↑ Gulley ML, Nicholls JM, Schneider BG, Amin MB, Ro JY, Geradts J (April 1998). "Nasopharyngeal carcinomas frequently lack the p16/MTS1 tumor suppressor protein but consistently express the retinoblastoma gene product". Am. J. Pathol. 152 (4): 865–9. PMC 1858242. PMID 9546345. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1858242/.
- ↑ Singhi, AD.; Califano, J.; Westra, WH. (Feb 2012). "High-risk human papillomavirus in nasopharyngeal carcinoma.". Head Neck 34 (2): 213-8. doi:10.1002/hed.21714. PMID 21484924.
- ↑ 46.0 46.1 Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Oberman, Harold A; Reuter, Victor E (2004). Sternberg's Diagnostic Surgical Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 975. ISBN 978-0781740517.
- ↑ Wenig BM (March 2002). "Squamous cell carcinoma of the upper aerodigestive tract: precursors and problematic variants". Mod. Pathol. 15 (3): 229–54. doi:10.1038/modpathol.3880520. PMID 11904340. http://www.nature.com/modpathol/journal/v15/n3/pdf/3880520a.pdf.
- ↑ URL: http://www.pathconsultddx.com/pathCon/diagnosis?pii=S1559-8675%2806%2970297-2. Accessed on: March 9, 2010.
- ↑ URL: http://www.biomedcentral.com/1471-2407/6/146. Accessed on: March 9, 2010.
- ↑ Abu-Eid R, Landini G (March 2006). "Morphometrical differences between pseudo-epitheliomatous hyperplasia in granular cell tumours and squamous cell carcinomas". Histopathology 48 (4): 407–16. doi:10.1111/j.1365-2559.2006.02350.x. PMID 16487362.
- ↑ 51.0 51.1 51.2 51.3 Thompson, LD. (Sep 2009). "Olfactory neuroblastoma.". Head Neck Pathol 3 (3): 252-9. doi:10.1007/s12105-009-0125-2. PMC 2811627. PMID 20596981. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2811627/.
- ↑ 52.0 52.1 52.2 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 41. ISBN 978-0781765275.
- ↑ URL: http://path.upmc.edu/cases/case467.html. Accessed on: 21 January 2012.
- ↑ Klatt, Edward C. (2006). Robbins and Cotran Atlas of Pathology (1st ed.). Saunders. pp. 144. ISBN 978-1416002741.
- ↑ 55.0 55.1 URL: http://emedicine.medscape.com/article/994274-overview. Accessed on: 16 March 2011.
- ↑ http://emedicine.medscape.com/article/333492-overview
- ↑ URL: http://emedicine.medscape.com/article/994274-diagnosis. Accessed on: 16 March 2011.
- ↑ Beju D, Meek WD, Kramer JC (April 2004). "The ultrastructure of the nasal polyps in patients with and without cystic fibrosis". J. Submicrosc. Cytol. Pathol. 36 (2): 155–65. PMID 15554502.
- ↑ Davidsson, A.; Hellquist, HB. (1993). "The so-called 'allergic' nasal polyp.". ORL J Otorhinolaryngol Relat Spec 55 (1): 30-5. PMID 8441521.
- ↑ Klatt, Edward C. (2006). Robbins and Cotran Atlas of Pathology (1st ed.). Saunders. pp. 144. ISBN 978-1416002741.
- ↑ http://www.nature.com/modpathol/journal/v13/n10/full/3880208a.html
- ↑ URL: http://emedicine.medscape.com/article/862677-overview. Accessed on: 19 November 2011.
- ↑ 63.0 63.1 63.2 63.3 63.4 63.5 Barnes L (March 2002). "Schneiderian papillomas and nonsalivary glandular neoplasms of the head and neck". Mod. Pathol. 15 (3): 279–97. doi:10.1038/modpathol.3880524. PMID 11904343. http://www.nature.com/modpathol/journal/v15/n3/full/3880524a.html.
- ↑ Vrabec, DP. (May 1994). "The inverted Schneiderian papilloma: a 25-year study.". Laryngoscope 104 (5 Pt 1): 582-605. PMID 8189990.
- ↑ Bravo Domínguez, O.; Vela Cortina, M.; Ramírez Ruiz, RD.; Ros Vergara, A.; Dinarés Jaumeandreu, D.; Encina Ruiz, L.; Arias Cuchí, G.; Ardíaca Bosch, MC. et al. (2005). "[Oncocytic schneiderian papilloma. A case report].". An Otorrinolaringol Ibero Am 32 (2): 115-23. PMID 15929584.