Wilms tumour
Jump to navigation
Jump to search
| Wilms tumour | |
|---|---|
| Diagnosis in short | |
 Wilms tumour. H&E stain. | |
|
| |
| Synonyms | nephroblastoma |
| LM DDx | metanephric adenoma, nephrogenic nests, small round cell tumours, Immature teratoma |
| IHC | WT-1 +ve, CD56 +ve |
| Site | kidney - see pediatric kidney tumours |
|
| |
| Syndromes | WAGR syndrome, Beckwith-Wiedemann syndrome, Denys-Drash syndrome |
|
| |
| Signs | +/-abdominal mass |
| Prevalence | most common pediatric kidney tumour |
Wilms tumour, also nephroblastoma and Wilms' tumour, is the most common pediatric kidney tumour.[1][2]
General
- Common abdominal pediatric tumour.
- Affects approximately 1 in 8000 children.
- There is no sex predilection and the mean patient age at diagnosis ranges among 37 to 43 months.
- May be associated with a syndrome:[3]
- WAGR syndrome (Wilms tumour, Aniridia (absence of iris), GU abnormalities, Retardation).[4]
- Beckwith-Wiedemann syndrome.[5]
- Denys-Drash syndrome.[6]
Gross
Features [7]
- Most nephroblastomas are unifocal.
- Usually solitary, rounded, multilobular masses sharply demarcated from adjacent parenchyma.
- The cut surface is most commonly pale grey or tan.
- Cyst most be prominent in some cases.
- Multifocal masses in a single kidney and bilateral primary lesions are less frequent.
Images
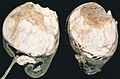
Wilms tumour. (WC/AFIP)

www:
Microscopic
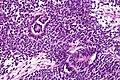
Features - classically three components (blastema, immature stroma, tubules):[8]
- Malignant small round blue cells ("blastema"):
- The blastemal component is the least differentiated cellular element.
- Size = ~ 2x RBC diameter.
- Nuclear pleomorphism (variation of size, shape and staining).
- Irregular nuclear membrane - important.
- Scant/difficult to discern cytoplasm - basophilic (light blue).
- Mitoses - common.
- Stroma ("immature stroma"):
- Spindle cells:
- Elliptical nuclear membrane.
- Abundant loose cytoplasm.
- Spindle cells:
- Epithelial components ("tubules"):
- Primitive rossete-like tubules, well-formed maturing and mature tubules, glomerular structures and variably papillary architecture.
- Usually clustered.
- Usu. have a central (clear/white) space surrounded by a rim of intensely eosinophilic cytoplasm.
- Nuclei of tubular structures often elongated and palisaded.
- Primitive rossete-like tubules, well-formed maturing and mature tubules, glomerular structures and variably papillary architecture.
Other findings:
- Commonly seen in association with nephrogenic rests.
- Cluster of cells small (blue) cells; lack nuclear atypia seen in Wilms tumour.[9]
- +/-Heterologous elements (skeletal muscle, smooth muscle adipose tissue, cartilage).[10]
- Heterologous = doesn't normally belong there.[11]
DDx:
- Metanephric adenoma.
- Nephrogenic nests.
- Other small round cell tumours.
- Synovial sarcoma, biphasic - especially in adults.
- Immature teratoma.
Notes:
- Palisade = fence made of stakes driven into the ground.[12]
- Approximately 30-40% Wilms tumour cases have nephrogenic rests.[13]
- The three phases are also called blastemal, epithelial and stromal.[10]
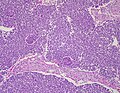
Images
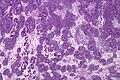
Wilms tumour - low mag. (WC/Nephron)
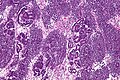
Wilms tumour - intermed. mag. (WC/Nephron)
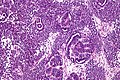
Wilms tumour - high mag. (WC/Nephron)
Wilms tumour - very high mag. (WC/Nephron)
Wilms tumor - low mag. (WC/Ed Uthman)



_(4882456062).jpg)
www:
{kind=link}
Anaplasia
Subclassified as:[10]
- Focal anaplasia.
- Diffuse anaplasia.
Criteria (all of the following):[10]
- Atypical mitoses.
- Nuclear hyperchromasia.
- Nuclear size variation (of the tumour cells) > 3x.
IHC
- WT-1 +ve (nuclear).
- CD56 +ve.[14]
- -ve in metanephric adenoma.
Molecular
- Cytogenetics[15]
- Partial gains of 1q.
- Partial losses of 1p, 1q, 4q, 11q, 16q, 22q.
- Complete loss of chromosome 16, 11, 12, 22.
- Trisomy of chromosome 8, 12, 13, 18.
See also
References
- ↑ Coppes MJ, Wolff JE, Ritchey ML (1999). "Wilms tumour: diagnosis and treatment". Paediatr Drugs 1 (4): 251–62. PMID 10935424.
- ↑ Stefanowicz J, Sierota D, Balcerska A, Stoba C (2004). "[Wilms' tumour of unfavorable histology--results of treatment with the SIOP 93-01 protocol at the Gdańsk centre. Preliminary report]" (in Polish). Med Wieku Rozwoj 8 (2 Pt 1): 197–200. PMID 15738594.
- ↑ URL: http://emedicine.medscape.com/article/989398-overview. Accessed on: 9 March 2011.
- ↑ Online 'Mendelian Inheritance in Man' (OMIM) 194072
- ↑ Online 'Mendelian Inheritance in Man' (OMIM) 130650
- ↑ Online 'Mendelian Inheritance in Man' (OMIM) 194080
- ↑ Coppes, MJ.; Arnold, M.; Beckwith, JB.; Ritchey, ML.; D'Angio, GJ.; Green, DM.; Breslow, NE. (Apr 1999). "Factors affecting the risk of contralateral Wilms tumor development: a report from the National Wilms Tumor Study Group.". Cancer 85 (7): 1616-25. PMID 10193955.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 254-5. ISBN 978-1416054542.
- ↑ URL: http://www.pathconsultddx.com/pathCon/diagnosis?pii=S1559-8675%2806%2970416-8. Accessed on: 28 March 2011.
- ↑ 10.0 10.1 10.2 10.3 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 282. ISBN 978-0781765275.
- ↑ URL: http://www.biology-online.org/dictionary/Heterologous. Accessed on: 1 October 2011.
- ↑ URL: http://www.thefreedictionary.com/palisaded. Accessed on: 2 February 2011.
- ↑ Coppes MJ, Haber DA, Grundy PE (September 1994). "Genetic events in the development of Wilms' tumor". N. Engl. J. Med. 331 (9): 586–90. doi:10.1056/NEJM199409013310906. PMID 8047084.
- ↑ Muir, TE.; Cheville, JC.; Lager, DJ. (Oct 2001). "Metanephric adenoma, nephrogenic rests, and Wilms' tumor: a histologic and immunophenotypic comparison.". Am J Surg Pathol 25 (10): 1290-6. PMID 11688464.
- ↑ Md Zin, R.; Murch, A.; Charles, A. (Jun 2011). "Pathology, genetics and cytogenetics of Wilms' tumour.". Pathology 43 (4): 302-12. doi:10.1097/PAT.0b013e3283463575. PMID 21516053.