Stomach carcinoma
(Redirected from Gastric adenocarcinoma)
Jump to navigation
Jump to search
| Stomach carcinoma | |
|---|---|
| Diagnosis in short | |
|
Template:Px Stomach signet ring cell carcinoma. H&E stain. | |
| Subtypes | Lauren classification: intestinal type, diffuse type; WHO classification: papillary carcinoma, tubular carcinoma, mucinous carcinoma, signet-ring carcinoma, undifferentiated carcinoma, adenosquamous carcinoma |
| LM DDx | gastric xanthoma, neuroendocrine tumour, metastatic carcinoma (e.g.pancreatic ductal adenocarcinoma, gastric dysplasia |
| Stains | CK7 +ve, CK20 -ve/+ve |
| Site | stomach |
|
| |
| Syndromes | hereditary diffuse gastric cancer, familial adenomatous polyposis, Lynch syndrome, Peutz-Jeghers syndrome, Li-Fraumeni syndrome, Gastric adenocarcinoma and proximal polyposis of the stomach (GAPPS) |
|
| |
| Prevalence | uncommon |
| Endoscopy | +/-linitis plastica (diffuse carcinomas), +/-ulcer with heaped (raised) edges (intestinal carcinomas) |
| Prognosis | usually very poor |
| Clin. DDx | benign ulcer, other gastric tumours |
| Treatment | surgery if feasible |
Stomach carcinoma, also carcinoma of the stomach and gastric carcinoma, is an epithelial derived malignant tumour that arises from the stomach.
Many gastric carcinomas form glands and can thus be called gastric adenocarcinoma or adenocarcinoma of the stomach.
General
Epidemiology:
- Prognosis is often poor as it is discovered at a late stage.
- Higher prevalence in countries in the far east (e.g. Japan) - thought to be environmental, e.g. diet.
Risk factors:
- Associated with helicobacter infections, i.e. Helicobacter gastritis.
- Alcohol - heavy use.[1]
- Genetic syndromes:
Note:
- Possible association with tobacco use - dependent on the study.[3]
Treatment:
- Surgical excision.
- Proximal tumours may require a complete gastrectomy as the stomach is innervated from its proximal part.
Classification
- Two different classification schemes.
- Lauren[4] - two types:
- Intestinal type (mass forming).
- Diffuse type (infiltrative).
- WHO classification - 6 subtypes for adenocarcinoma:[5]
- Papillary carcinoma.
- Tubular carcinoma.
- Mucinous carcinoma.
- Signet-ring carcinoma.
- Undifferentiated carcinoma.
- Adenosquamous carcinoma.
- Lauren[4] - two types:
Lame memory device STOMACH:
- Signet ring, Tubular, Oh papillary, Mucinous, Adenosquamouas, Crappy High grade (Undifferentiated).
Gross
Location:
- Large carcinomas preferentially involve the lesser curvature.[6]
- Ulceration with heaped (raised) edges.
- Appearance of the typical intestinal type tumour.
- Diffuse wall thickening with loss of the rugae - called linitis plastica.
- Typically due to diffuse carcinoma.
Main DDx of gastric ulcer:
- Peptic ulcer disease - have a "punched-out" appearance: sharp edge, no granularity of surrounding mucosa.
Images

Linitis plastica - endoscopic image. (WC)

Ulcerating gastric carcinoma. (WC)

Ulcerating gastric carcinoma. (WC)



Microscopic
Features - variable, either of the two following:
- "Typical adenocarcinoma":
- Gland-forming lesion that infiltrates into the lamina propria or beyond.
- Nuclear pleomorphism - common.
- +/-Signet ring carcinoma.
- Scattered single cells in the lamina propria or beyond with:
- Abundant cytoplasm containing one large (mucin-filled) vacuole.
- A peripheral nucleus (displaced by the vacuole).
- Scattered single cells in the lamina propria or beyond with:
DDx:
- Gastric xanthoma - may mimic signet ring cell carcinoma.
- Neuroendocrine tumour - esp. for poorly differentiated; no gland formation.
- Metastatic carcinoma.
- Gastric dysplasia.
Grading
- Moderately differentiated >=50 % glands.[citation needed]
- Poorly differentiated >=50% no glands (sheeting or nests).
Images
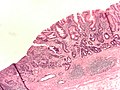
Gastric adenocarcinoma. (WC)
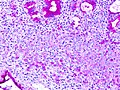
Gastric SRC - PAS stain. (WC)

_PAS_stain.jpg)
{kind=link}
www:
Stains
- Mucicarmine +ve.
IHC
Others:
- p53 +ve in upto 75% of cases.[8]
Molecular
- May have HER2 over expression - more common in intestinal-type tumours.[9]
- Poor prognosis - like in breast cancer.
- Scoring system different than in breast cancer - complete membrane staining is not required.
Staging
- Sixteen (or more) lymph nodes should be assessed (as per the 7th Ed. of the UICC/AJCC staging).[10]
- The 5th Ed. of the UICC/AJCC staging manual stated 15 lymph nodes.[10]
Sign out
Biopsy
Intestinal type
Stomach, Biopsy: - INVASIVE ADENOCARCINOMA, INTESTINAL TYPE, moderately differentiated. - Gastric mucosa with intestinal metaplasia. Comment: The tumour stains as follows: POSITIVE: CK7, CDX2. NEGATIVE: CD20. HER2 testing has been ordered and will be reported as an addendum.
STOMACH, BIOPSY: - INVASIVE ADENOCARCINOMA, INTESTINAL TYPE, MODERATELY DIFFERENTIATED. - Gastric mucosa with moderate chronic active inflammation and extensive intestinal metaplasia. - Benign small bowel mucosa with erosions.
GASTRIC ULCER, BIOPSY: - INVASIVE ADENOCARCINOMA, INTESTINAL-TYPE, MODERATELY DIFFERENTIATED.
Diffuse type
STOMACH, BIOPSY: - INVASIVE ADENOCARCINOMA, DIFFUSE TYPE. COMMENT: A pankeratin immunostain demonstrates single (infiltrating) epithelial cells in the lamina propria.
Micro
The tumour consists of single cells with abundant foamy-appearing cytoplasm and eccentric nuclei with mild nuclear atypia.
Poorly differentiated
GASTRIC ULCER, BIOPSY: - INVASIVE ADENOCARCINOMA, POORLY-DIFFERENTIATED.
See also
References
- ↑ Duell, EJ.; Travier, N.; Lujan-Barroso, L.; Clavel-Chapelon, F.; Boutron-Ruault, MC.; Morois, S.; Palli, D.; Krogh, V. et al. (Nov 2011). "Alcohol consumption and gastric cancer risk in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort.". Am J Clin Nutr 94 (5): 1266-75. doi:10.3945/ajcn.111.012351. PMID 21993435.
- ↑ Rudloff, U. (2018). "Gastric adenocarcinoma and proximal polyposis of the stomach: diagnosis and clinical perspectives.". Clin Exp Gastroenterol 11: 447-459. doi:10.2147/CEG.S163227. PMID 30584346.
- ↑ Nomura, A.; Grove, JS.; Stemmermann, GN.; Severson, RK. (Nov 1990). "Cigarette smoking and stomach cancer.". Cancer Res 50 (21): 7084. PMID 2208177.
- ↑ LAUREN P (1965). "THE TWO HISTOLOGICAL MAIN TYPES OF GASTRIC CARCINOMA: DIFFUSE AND SO-CALLED INTESTINAL-TYPE CARCINOMA. AN ATTEMPT AT A HISTO-CLINICAL CLASSIFICATION". Acta Pathol Microbiol Scand 64: 31–49. PMID 14320675.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 823. ISBN 0-7216-0187-1.
- ↑ Yamagawa, H.; Onishi, T. (Sep 1989). "[A clinicopathological study of early gastric cancers with a diameter larger than five centimeters].". Gan No Rinsho 35 (10): 1114-8. PMID 2550682.
- ↑ Werling, RW.; Yaziji, H.; Bacchi, CE.; Gown, AM. (Mar 2003). "CDX2, a highly sensitive and specific marker of adenocarcinomas of intestinal origin: an immunohistochemical survey of 476 primary and metastatic carcinomas.". Am J Surg Pathol 27 (3): 303-10. PMID 12604886.
- ↑ Zali, MR.; Moaven, O.; Asadzadeh Aghdaee, H.; Ghafarzadegan, K.; Ahmadi, KJ.; Farzadnia, M.; Arabi, A.; Abbaszadegan, MR. (Jul 2009). "Clinicopathological significance of E-cadherin, β-catenin and p53 expression in gastric adenocarinoma.". J Res Med Sci 14 (4): 239-47. PMID 21772890.
- ↑ Romiti, A.; Di Rocco, R.; Milione, M.; Ruco, L.; Ziparo, V.; Zullo, A.; Duranti, E.; Sarcina, I. et al. (Jan 2012). "Somatostatin receptor subtype 2 A (SSTR2A) and HER2 expression in gastric adenocarcinoma.". Anticancer Res 32 (1): 115-9. PMID 22213295.
- ↑ 10.0 10.1 Deng, JY.; Liang, H. (Apr 2014). "Clinical significance of lymph node metastasis in gastric cancer.". World J Gastroenterol 20 (14): 3967-75. doi:10.3748/wjg.v20.i14.3967. PMID 24744586.