Metaphyseal fibrous defect
(Redirected from Fibrous cortical defect)
Jump to navigation
Jump to search
| Metaphyseal fibrous defect | |
|---|---|
| Diagnosis in short | |
 | |
|
| |
| Synonyms | nonossifying fibroma, fibrous cortical defect, fibrous metaphyseal defect, fibroxanthoma of bone |
| LM DDx | giant cell tumour of bone, others |
| Site | metaphysis of bone - usu. lower extremity |
|
| |
| Clinical history | incidental radiograhic finding |
| Prevalence | common |
| Radiology | lucent defect |
| Prognosis | benign |
| Treatment | none |
| Metaphyseal fibrous defect | |
|---|---|
| External resources | |
| Wikipedia | Nonossifying fibroma |
| Pathology Outlines | topic/bonemetaphysealfibrousdefect |
Metaphyseal fibrous defect, abbreviated MFD, is a common benign abnormality of the metaphysis, classically seen in children and young adults.
They are also known as fibrous cortical defect, fibrous metaphyseal defect, and fibroxanthoma of bone. Nonossifying fibroma is a larger lesion but otherwise identical.
General
- Common.
- Non-neoplastic.
- Self-limited.
- Skeletally immature individuals, children and adolescents.
- Often small lesions discovered as an radiographic incidentaloma.
- Rarely seen as a pathologic specimen (should not be biopsied).
- May be seen in the context of Jaffe-Campanacci syndrome which may be a presentation of Neurofibromatosis Type 1.[1][2]
- Radiographic diagnosis.
Clinical history:
- Incidental radiographic finding.
- Pathologic fracture.
Treatment:
- None (spontaneously resolve by ossification).
- Diagnosis is part of the skeletal do not touch list.[3]
Notes:
- May resolve into a bone island.
Clinical DDx:
- FOG MACHINES acronym for radiographically lytic bone lesions.[4]
Gross
- Firm, granular, brown to yellow to red.
Site:
- Metaphysis of distal femur or proximal tibia (80%).
- Cortical.
- Metaphysis.
- Long bones.
- Eccentric location.
Radiology
- Sharply demarcated, lucent, loculated, meta-diaphyseal lesion.
- Surrounded by a rim of sclerotic bone.

Nonossifying fibroma. (WC)

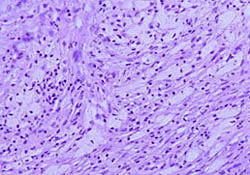
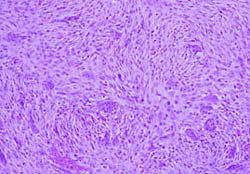
Microscopic
Features:
- Spindle cells without cytologic atypia are arranged in a storiform pattern.
- Scattered chronic inflammatory cells and benign giant cells.
- Foam cells and hemosiderin deposition are present.
- Mitoses are seen but cytologic atypia is absent.
DDx (microscopic):
- Giant cell tumour of bone - epiphyseal location, occurs in adults.
- Other giant cell lesions of bone.
- Spindle cell lesions of bone.
Images

Metaphyseal fibrous defect - intermediate magnification.

Metaphyseal fibrous defect - high magnification.

www:
{kind=link}
{kind=link}
%20micro.jpg){kind=link}
Stains
- Not relevant.
IHC
- Not relevant.
Molecular
- Not relevant.
Sign out
BONE, CURETTAGE: - METAPHYSEAL FIBROUS DEFECT / NONOSSIFYING FIBROMA.
See also
- Bone.
References
- ↑ URL: http://www.bonetumor.org/plasma-cell-tumors/jaffe-campanacci-syndrome. Accessed on: October 14, 2014.
- ↑ Stewart, DR.; Brems, H.; Gomes, AG.; Ruppert, SL.; Callens, T.; Williams, J.; Claes, K.; Bober, MB. et al. (Jun 2014). "Jaffe-Campanacci syndrome, revisited: detailed clinical and molecular analyses determine whether patients have neurofibromatosis type 1, coincidental manifestations, or a distinct disorder.". Genet Med 16 (6): 448-59. doi:10.1038/gim.2013.163. PMID 24232412.
- ↑ URL: http://radiopaedia.org/articles/skeletal-do-not-touch-lesions-1. Accessed on: October 14, 2014.
- ↑ URL: http://radiopaedia.org/articles/lytic-bone-lesion-mnemonic. Accessed on: October 14, 2014.