Uterus
The uterus is essential for survival of the species. It is commonly afflicted with tumours.
Endometrium and its pathology is dealt with in the endometrium, endometrial hyperplasia and endometrial carcinoma articles.
Other tumours are dealt with in uterine tumours.
Operations
- Myomectomy.
- Indication: uterine leiomyomas.
- Subtotal hysterectomy.
- Discouraged... as the cervix remains and can develop a cancer.
- Total hysterectomy.
- Indications:
- Endometrial cancer (low stage, good histologic type), endometrial hyperplasia.
- Uterine prolapse.
- Uterine adenomyosis.
- Uterine leiomyomas.
- Chronic pelvic pain.[1]
- Indications:
- Radical hysterectomy - total hysterectomy + parametrial tissue.[2]
- Indications: cervical cancers, advanced uterine cancers.
- This is typically done by gynecologists with additional training at larger centres.
- Usually done with a bilateral salpingo-opherectomy (both tubes and ovaries) and pelvic lymph node dissection.
- Indications: cervical cancers, advanced uterine cancers.
Notes:
- There are almost no quality of life differences between total & subtotal hysterectomy.[3]
- Simple hysterectomy is removal of the uterus and cervix;[4] it can be used as a synonym for total hysterectomy.[5]
Grossing hysterectomy specimens
- Hysterectomy for endometrial cancer grossing.
- Hysterectomy for endometrial hyperplasia grossing.
- Hysterectomy for fibroids grossing.
Hysterectomy specimens - orientation
Orientation:
- Less peritoneum on anterior (as the urinary bladder is there).
- Posterior peritoneal edge: pointy (upside down triangle).
- Anterior peritoneal edge: rounded/non-pointy.
- Posterior peritoneal edge: pointy (upside down triangle).
- Tubes on anterior-lateral aspect.[6]
- Round ligaments posterior to tubes.
Normal uterine wall
Gross
- Firm.
- Pear-shaped.
- Not quite true -- it is usu. flattened at the anterior and posterior.
Negatives:
- No nodules.
- No trabeculations.
Microsopic
Features:
- Smooth muscle arranged in fascicles.
IHC
- ER +ve.
- PR +ve.
Tumours of the corpus
Main article: Uterine tumours
The most common is leiomyoma (uterine fibroids).
Endometrium
Main article: Endometrium
Dealt with in endometrium, endometrial hyperplasia and endometrial carcinoma articles.
Specific conditions
Congenital absence of the uterus
General
- Often associated with absence of the deep portion of the vagina; thus, may be congenital absence of the uterus and vagina (CAUV).
- May go by the name Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome.[7]
- May be seen in the context of Müllerian agenesis. (???)
Features:[7]
- Subdivided - as etiologies differ.
- Thought to have a genetic component - autosomal dominant with variable penetration.
Treatment:
- Uterine transplant - attempted.[8]
Uterus didelphys
General
- Benign - though may adversely affect fertility.[9]
- Rare - seen in < 0.3% deliveries.[10]
- Can be thought of as double uterus - a consequence of the Muellerian ducts not fusing.
Related conditions:
- Arcuate uterus - fundus has a concave contour towards the uterine cavity.
- Septate uterus.
- Bicornuate uterus.
- Uterus didelphys.
Image:
Gross
- Two uteri - each have a cervix, each connect to one fallopian tube/ovary.
- +/-Vaginal septum or double vagina.[10]
Microscopic
- Non-specific - gross diagnosis.
Uterine adenomyosis
- AKA adenomyosis of the uterus.
Main article: Uterine adenomyosis
Uterine prolapse
- Urogenital prolapse redirects here.
General
- Clinical diagnosis.
- A common indication for a total hysterectomy.
- Hysterectomy specimen usually comes with some vaginal mucosa.
- Parous women, usually menopausal.[12]
- Possibly obesity - studies vary.[13]
Gross
- Long cervix.
Microscopic
Features:
- Uterus: non-specific.
- Vaginal mucosa: (focal) keratinization due to rubbing - common finding.
Images
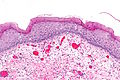
Keratinized cervix - intermed. mag. (WC)

Keratinized cervix - high mag. (WC)

Keratinized cervix - very high mag. (WC)



{kind=link}
Sign out
UTERUS AND CERVIX, TOTAL HYSTERECTOMY: - UTERINE CERVIX WITH FOCAL KERATINIZATION OTHERWISE WITHIN NORMAL LIMITS. - NONPROLIFERATIVE ENDOMETRIUM.
UTERUS AND CERVIX, TOTAL HYSTERECTOMY: - UTERINE CERVIX WITH KERATINIZATION, OTHERWISE WITHIN NORMAL LIMITS. - CYSTIC NONPROLIFERATIVE ENDOMETRIUM. - UTERINE SMOOTH MUSCLE AND SEROSA WITHIN NORMAL LIMITS. - NEGATIVE FOR MALIGNANCY.
Denudated exocervix
UTERUS AND CERVIX, TOTAL HYSTERECTOMY: - UTERINE CERVIX WITH MILD CHRONIC INFLAMMATION AND EXOCERVICAL DENUDATION, NO EVIDENCE OF DYSPLASIA. - CYSTIC NONPROLIFERATIVE ENDOMETRIUM. - UTERINE CORPUS WITH BENIGN HYALINIZED NODULE. - NEGATIVE FOR MALIGNANCY. COMMENT: Levels were cut on the uterine cervix sections (A1 and A2).
Focal ulceration
- UTERINE CERVIX WITH PARAKERATOSIS, ACANTHOSIS, CHRONIC INFLAMMATION, AND FOCAL ULCERATION ASSOCIATED WITH GRANULATION TISSUE FORMATION. - PARTIALLY CYSTIC NONPROLIFERATIVE ENDOMETRIUM. - UTERINE CORPUS WITH LEIOMYOMA. - NO EVIDENCE OF DYSPLASIA. - NEGATIVE FOR HYPERPLASIA AND NEGATIVE FOR MALIGNANCY.
With endometrial polyp
UTERUS AND CERVIX, TOTAL HYSTERECTOMY: - BENIGN ENDOMETRIAL POLYP WITH NONPROLIFERATIVE ENDOMETRIAL GLANDS. - UTERINE CERVIX WITH MILD CHRONIC INFLAMMATION AND FOCAL EXOCERVICAL DENUDATION, NO EVIDENCE OF DYSPLASIA. - VERY WEAKLY PROLIFERATIVE ENDOMETRIUM, MOSTLY ATROPHIC APPEARING, NEGATIVE FOR ENDOMETRIAL HYPERPLASIA. - UTERINE CORPUS WITHIN NORMAL LIMITS. - NEGATIVE FOR MALIGNANCY.
Dysfunctional uterine bleeding
- Abbreviated DUB.
General
- Clinical diagnosis based on negative pathology - specifically a negative endometrial biopsy.
Clinical:
Microscopic
Features:
- Endometrium within normal limits - see proliferative phase endometrium and secretory phase endometrium.
Sign out
Uterus, Cervix, and Bilateral Uterine Tubes, Total Hysterectomy and Bilateral Salpingectomy: - Uterine cervix within normal limits. - Proliferative phase endometrium with focal fibrosis, compatible with prior ablation. - Uterine leiomyomas. - Bilateral uterine tubes without significant pathology. - NEGATIVE for malignancy.
Block letters
A. OMENTUM, BIOPSY: - FIBROADIPOSE TISSUE WITHIN NORMAL LIMITS -- CONSISTENT WITH OMENTUM. B. UTERUS, SUBTOTAL HYSTERECTOMY: - SECRETORY PHASE ENDOMETRIUM. - UTERINE WALL WITHIN NORMAL LIMITS.
UTERUS, CERVIX, AND BILATERAL UTERINE TUBES, TOTAL HYSTERECTOMY AND BILATERAL SALPINGECTOMY: - UTERINE CERVIX WITHIN NORMAL LIMITS. - PROLIFERATIVE PHASE ENDOMETRIUM WITH FOCAL FIBROSIS, COMPATIBLE WITH PRIOR ABLATION. - UTERINE LEIOMYOMAS. - BILATERAL UTERINE TUBES WITHOUT SIGNIFICANT PATHOLOGY. - NEGATIVE FOR MALIGNANCY.
See also
References
- ↑ Lamvu, G. (May 2011). "Role of hysterectomy in the treatment of chronic pelvic pain.". Obstet Gynecol 117 (5): 1175-8. doi:10.1097/AOG.0b013e31821646e1. PMID 21508759.
- ↑ Frumovitz, M.; Sun, CC.; Schmeler, KM.; Deavers, MT.; Dos Reis, R.; Levenback, CF.; Ramirez, PT. (Jul 2009). "Parametrial involvement in radical hysterectomy specimens for women with early-stage cervical cancer.". Obstet Gynecol 114 (1): 93-9. doi:10.1097/AOG.0b013e3181ab474d. PMID 19546764.
- ↑ Thakar, R.; Ayers, S.; Clarkson, P.; Stanton, S.; Manyonda, I. (Oct 2002). "Outcomes after total versus subtotal abdominal hysterectomy.". N Engl J Med 347 (17): 1318-25. doi:10.1056/NEJMoa013336. PMID 12397189.
- ↑ Somashekhar, SP.; Ashwin, KR. (Sep 2015). "Management of Early Stage Cervical Cancer.". Rev Recent Clin Trials. PMID 26411950.
- ↑ URL: http://www.baymoon.com/~gyncancer/library/glossary/bldefhyster.htm. Accessed on: 8 October 2015.
- ↑ Lester, Susan Carole (2010). Manual of Surgical Pathology (3rd ed.). Saunders. pp. 425. ISBN 978-0-323-06516-0.
- ↑ 7.0 7.1 URL: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1832178/.
- ↑ URL: http://singularityhub.com/2011/06/18/in-a-medical-first-infertile-daughter-will-receive-uterus-from-mother-video/. Accessed on: 17 June 2011.
- ↑ Taylor, E.; Gomel, V. (Jan 2008). "The uterus and fertility.". Fertil Steril 89 (1): 1-16. doi:10.1016/j.fertnstert.2007.09.069. PMID 18155200.
- ↑ 10.0 10.1 Brown, DC.; Nelson, RF. (Mar 1967). "Uterus didelphys and double vagina with delivery of a normal infant from each uterus.". Can Med Assoc J 96 (11): 675-7. PMC 1936081. PMID 6019679. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1936081/.
- ↑ URL: http://www.msdlatinamerica.com/ebooks/RadiologyReviewManual/sid1652818.html. Accessed on: 28 April 2012.
- ↑ Mladenović-Segedi, L.; Segedi, D.. "[Most important etiologic factors in the development of genital prolapse].". Srp Arh Celok Lek 138 (5-6): 315-8. PMID 20607975.
- ↑ Thubert, T.; Deffieux, X.; Letouzey, V.; Hermieu, JF. (Jul 2012). "[Obesity and urogynecology: a systematic review].". Prog Urol 22 (8): 445-53. doi:10.1016/j.purol.2012.03.009. PMID 22732579.