Difference between revisions of "Thyroid gland nodular hyperplasia"
(redirect w/ cat.) |
|||
| (9 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
{{ Infobox diagnosis | |||
| Name = {{PAGENAME}} | |||
| Image = Thyroid FNA, Benign, Consistent with Adenomatoid Nodule (8116075837).jpg | |||
| Width = | |||
| Caption = Thyroid FNA compatible with adenomatoid nodule. | |||
| Synonyms = nodular hyperplasia, adenomatoid nodule | |||
| Micro = typically follicles of variable size - may be microfollicular or solid; no nuclear changes of [[papillary thyroid carcinoma|PTC]]; no fibrous capsule | |||
| Subtypes = | |||
| LMDDx = [[papillary thyroid carcinoma]], [[follicular thyroid adenoma]], [[follicular thyroid carcinoma]] | |||
| Stains = | |||
| IHC = | |||
| EM = | |||
| Molecular = | |||
| IF = | |||
| Gross = enlarged thyroid gland +/- distinct nodules | |||
| Grossing = | |||
| Site = [[thyroid gland]] | |||
| Assdx = | |||
| Syndromes = | |||
| Clinicalhx = | |||
| Signs = thyroid gland enlargement | |||
| Symptoms = | |||
| Prevalence = common | |||
| Bloodwork = | |||
| Rads = | |||
| Endoscopy = | |||
| Prognosis = benign | |||
| Other = | |||
| ClinDDx = malignancy of thyroid gland | |||
| Tx = surgical resection | |||
}} | |||
'''Thyroid gland nodular hyperplasia''' is a common [[thyroid gland]] pathology and may be an indication for thyroidectomy. | |||
==General== | |||
*Clinical diagnosis: ''goitre'', [[AKA]] ''sporadic goitre'', AKA ''multinodular goitre'' (MNG). | |||
*Most common diagnosis in the thyroid. | |||
**If you've seen a handful of thyroids you've seen this. | |||
*Considered to be a combination of environmental factors (e.g. lack of iodine in the diet) and genetic factors (often with autosomal dominant inheritance).<ref name=pmid21487943>{{Cite journal | last1 = Paschke | first1 = R. | title = Molecular pathogenesis of nodular goiter. | journal = Langenbecks Arch Surg | volume = 396 | issue = 8 | pages = 1127-36 | month = Dec | year = 2011 | doi = 10.1007/s00423-011-0788-5 | PMID = 21487943 }}</ref> | |||
==Gross== | |||
Features: | |||
*Enlarge thyroid gland. | |||
*+/-Distinct (well-circumscribed) nodules. | |||
==Microscopic== | |||
Features: | |||
*Follicles of variable size - '''key feature'''. | |||
**Should be obvious at low power, i.e. with the 2.5x objective. | |||
*+/-Nodules. | |||
**Do not have a thick fibrous capsule. | |||
**May have a high cellularity. | |||
**Architecture: solid or microfollicular.<ref name=Ref_EP36>{{Ref EP|36}}</ref> | |||
Negatives: | |||
*No nuclear features suggestive of malignancy (at lower power). | |||
**One should not look at high power. | |||
*Not cellular. | |||
DDx: | |||
*[[Papillary thyroid carcinoma]] - esp. [[papillary thyroid carcinoma follicular variant]]. | |||
*[[Follicular thyroid adenoma]] - contained in a fibrous capsule. | |||
*[[Follicular thyroid carcinoma]] - has fibrous capsule and invasion through it. | |||
===Images=== | |||
<gallery> | |||
Image: Thyroid Benign Adenomatoid Nodule, FNA (5690954863).jpg | FNA c/w with AN. (WC/Euthman) | |||
Image: Thyroid FNA, Benign, Consistent with Adenomatoid Nodule (8116075837).jpg | FNA c/w AN. (WC/Euthman) | |||
</gallery> | |||
==Molecular== | |||
*Nodular hyperplasias may be clonal;<ref name=pmid1973172>{{Cite journal | last1 = Namba | first1 = H. | last2 = Matsuo | first2 = K. | last3 = Fagin | first3 = JA. | title = Clonal composition of benign and malignant human thyroid tumors. | journal = J Clin Invest | volume = 86 | issue = 1 | pages = 120-5 | month = Jul | year = 1990 | doi = 10.1172/JCI114673 | PMID = 1973172 }}</ref> however, this is not used for diagnosis and considered clinically irrelevant. | |||
==Sign out== | |||
<pre> | |||
HEMITHYROID, RIGHT, HEMITHYROIDECTOMY: | |||
- NODULAR HYPERPLASIA. | |||
- NEGATIVE FOR MALIGNANCY. | |||
</pre> | |||
<pre> | |||
HEMITHYROID, RIGHT, HEMITHYROIDECTOMY: | |||
- CELLULAR ADENOMATOID NODULE ON A BACKGROUND OF NODULAR HYPERPLASIA. | |||
- NEGATIVE FOR MALIGNANCY. | |||
</pre> | |||
<pre> | |||
RIGHT THYROID, RIGHT HEMITHYROIDECTOMY: | |||
- BENIGN NODULE WITH MICROFOLLICLES IN A BACKGROUND OF NODULAR HYPERPLASIA. | |||
- NEGATIVE FOR MALIGNANCY. | |||
</pre> | |||
===Micro=== | |||
The sections show thyroid gland with follicles of variable size and marked enlargement. | |||
A lymphocytic infiltrate is present. Focal germinal centre formation is present. Oncocytic changes and reactive changes are seen focally. No significant nuclear atypia is identified. | |||
====Alternate==== | |||
The sections show thyroid gland with follicles of variable size and marked enlargement. A large nodule is present with microfollicles that are densely packed around the edge and few in the centre. The nuclei of the microfollicles are round. No significant nuclear membrane irregularities there are apparent. Very rare enlarged nuclei are present. Occasional nucleoli are seen. No nuclear overlap is readily apparent. | |||
==See also== | |||
*[[Thyroid gland]]. | |||
*[[Thyroid cytopathology]]. | |||
==References== | |||
{{Reflist|2}} | |||
[[Category:Diagnosis]] | [[Category:Diagnosis]] | ||
[[Category:Thyroid gland]] | |||
Latest revision as of 18:16, 11 August 2015
| Thyroid gland nodular hyperplasia | |
|---|---|
| Diagnosis in short | |
.jpg) Thyroid FNA compatible with adenomatoid nodule. | |
|
| |
| Synonyms | nodular hyperplasia, adenomatoid nodule |
|
| |
| LM | typically follicles of variable size - may be microfollicular or solid; no nuclear changes of PTC; no fibrous capsule |
| LM DDx | papillary thyroid carcinoma, follicular thyroid adenoma, follicular thyroid carcinoma |
| Gross | enlarged thyroid gland +/- distinct nodules |
| Site | thyroid gland |
|
| |
| Signs | thyroid gland enlargement |
| Prevalence | common |
| Prognosis | benign |
| Clin. DDx | malignancy of thyroid gland |
| Treatment | surgical resection |
Thyroid gland nodular hyperplasia is a common thyroid gland pathology and may be an indication for thyroidectomy.
General
- Clinical diagnosis: goitre, AKA sporadic goitre, AKA multinodular goitre (MNG).
- Most common diagnosis in the thyroid.
- If you've seen a handful of thyroids you've seen this.
- Considered to be a combination of environmental factors (e.g. lack of iodine in the diet) and genetic factors (often with autosomal dominant inheritance).[1]
Gross
Features:
- Enlarge thyroid gland.
- +/-Distinct (well-circumscribed) nodules.
Microscopic
Features:
- Follicles of variable size - key feature.
- Should be obvious at low power, i.e. with the 2.5x objective.
- +/-Nodules.
- Do not have a thick fibrous capsule.
- May have a high cellularity.
- Architecture: solid or microfollicular.[2]
Negatives:
- No nuclear features suggestive of malignancy (at lower power).
- One should not look at high power.
- Not cellular.
DDx:
- Papillary thyroid carcinoma - esp. papillary thyroid carcinoma follicular variant.
- Follicular thyroid adenoma - contained in a fibrous capsule.
- Follicular thyroid carcinoma - has fibrous capsule and invasion through it.
Images

FNA c/w with AN. (WC/Euthman)
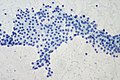
FNA c/w AN. (WC/Euthman)
.jpg)
Molecular
- Nodular hyperplasias may be clonal;[3] however, this is not used for diagnosis and considered clinically irrelevant.
Sign out
HEMITHYROID, RIGHT, HEMITHYROIDECTOMY: - NODULAR HYPERPLASIA. - NEGATIVE FOR MALIGNANCY.
HEMITHYROID, RIGHT, HEMITHYROIDECTOMY: - CELLULAR ADENOMATOID NODULE ON A BACKGROUND OF NODULAR HYPERPLASIA. - NEGATIVE FOR MALIGNANCY.
RIGHT THYROID, RIGHT HEMITHYROIDECTOMY: - BENIGN NODULE WITH MICROFOLLICLES IN A BACKGROUND OF NODULAR HYPERPLASIA. - NEGATIVE FOR MALIGNANCY.
Micro
The sections show thyroid gland with follicles of variable size and marked enlargement. A lymphocytic infiltrate is present. Focal germinal centre formation is present. Oncocytic changes and reactive changes are seen focally. No significant nuclear atypia is identified.
Alternate
The sections show thyroid gland with follicles of variable size and marked enlargement. A large nodule is present with microfollicles that are densely packed around the edge and few in the centre. The nuclei of the microfollicles are round. No significant nuclear membrane irregularities there are apparent. Very rare enlarged nuclei are present. Occasional nucleoli are seen. No nuclear overlap is readily apparent.
See also
References
- ↑ Paschke, R. (Dec 2011). "Molecular pathogenesis of nodular goiter.". Langenbecks Arch Surg 396 (8): 1127-36. doi:10.1007/s00423-011-0788-5. PMID 21487943.
- ↑ Thompson, Lester D. R. (2006). Endocrine Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 36. ISBN 978-0443066856.
- ↑ Namba, H.; Matsuo, K.; Fagin, JA. (Jul 1990). "Clonal composition of benign and malignant human thyroid tumors.". J Clin Invest 86 (1): 120-5. doi:10.1172/JCI114673. PMID 1973172.