Stomach carcinoma
Jump to navigation
Jump to search
Stomach carcinoma, also carcinoma of the stomach and gastric carcinoma, is an epithelial derived malignant tumour that arises from the stomach.
| Stomach carcinoma | |
|---|---|
| Diagnosis in short | |
 Stomach signet ring cell carcinoma. H&E stain. | |
| Subtypes | Lauren classification: intestinal type, diffuse type; WHO classification: papillary carcinoma, tubular carcinoma, mucinous carcinoma, signet-ring carcinoma, undifferentiated carcinoma, adenosquamous carcinoma |
| LM DDx | gastric xanthoma, neuroendocrine tumour, metastatic carcinoma (e.g.pancreatic ductal adenocarcinoma, gastric dysplasia |
| Stains | CK7 +ve, CK20 -ve/+ve |
| Site | stomach |
|
| |
| Syndromes | hereditary diffuse gastric cancer, familial adenomatous polyposis, Lynch syndrome, Peutz-Jeghers syndrome, Li-Fraumeni syndrome, Gastric adenocarcinoma and proximal polyposis of the stomach (GAPPS) |
|
| |
| Prevalence | uncommon |
| Endoscopy | +/-linitis plastica (diffuse carcinomas), +/-ulcer with heaped (raised) edges (intestinal carcinomas) |
| Prognosis | usually very poor |
| Clin. DDx | benign ulcer, other gastric tumours |
| Treatment | surgery if feasible |
Many gastric carcinomas form glands and can thus be called gastric adenocarcinoma or adenocarcinoma of the stomach.
General
Epidemiology:
- Prognosis is often poor as it is discovered at a late stage.
- Higher prevalence in countries in the far east (e.g. Japan) - thought to be environmental, e.g. diet.
Risk factors:
- Associated with helicobacter infections, i.e. Helicobacter gastritis.
- Alcohol - heavy use.[1]
- Genetic syndromes:
Note:
- Possible association with tobacco use - dependent on the study.[3]
Treatment:
- Surgical excision.
- Proximal tumours may require a complete gastrectomy as the stomach is innervated from its proximal part.
Classification
- Two different classification schemes.
- Lauren[4] - two types:
- Intestinal type (mass forming).
- Diffuse type (infiltrative).
- WHO classification - 6 subtypes for adenocarcinoma:[5]
- Papillary carcinoma.
- Tubular carcinoma.
- Mucinous carcinoma.
- Signet-ring carcinoma.
- Undifferentiated carcinoma.
- Adenosquamous carcinoma.
- Lauren[4] - two types:
Lame memory device STOMACH:
- Signet ring, Tubular, Oh papillary, Mucinous, Adenosquamouas, Crappy High grade (Undifferentiated).
Gross
Location:
- Large carcinomas preferentially involve the lesser curvature.[6]
- Ulceration with heaped (raised) edges.
- Appearance of the typical intestinal type tumour.
- Diffuse wall thickening with loss of the rugae - called linitis plastica.
- Typically due to diffuse carcinoma.
Main DDx of gastric ulcer:
- Peptic ulcer disease - have a "punched-out" appearance: sharp edge, no granularity of surrounding mucosa.
Images

Linitis plastica - endoscopic image. (WC)

Ulcerating gastric carcinoma. (WC)

Ulcerating gastric carcinoma. (WC)



Microscopic
Features - variable, either of the two following:
- "Typical adenocarcinoma":
- Gland-forming lesion that infiltrates into the lamina propria or beyond.
- Nuclear pleomorphism - common.
- +/-Signet ring carcinoma.
- Scattered single cells in the lamina propria or beyond with:
- Abundant cytoplasm containing one large (mucin-filled) vacuole.
- A peripheral nucleus (displaced by the vacuole).
- Scattered single cells in the lamina propria or beyond with:
DDx:
- Gastric xanthoma - may mimic signet ring cell carcinoma.
- Neuroendocrine tumour - esp. for poorly differentiated; no gland formation.
- Metastatic carcinoma.
- Gastric dysplasia.
Grading
- Moderately differentiated >=50 % glands.[citation needed]
- Poorly differentiated >=50% no glands (sheeting or nests).
Images
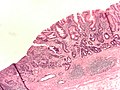
Gastric adenocarcinoma. (WC)
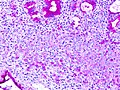
Gastric SRC - PAS stain. (WC)

_PAS_stain.jpg)
www:
Stains
- Mucicarmine +ve.
IHC
Others:
- p53 +ve in upto 75% of cases.[8]
Molecular
- May have HER2 over expression - more common in intestinal-type tumours.[9]
- Poor prognosis - like in breast cancer.
- Scoring system different than in breast cancer - complete membrane staining is not required.
Staging
Sign out
Biopsy
Intestinal type
Stomach, Biopsy: - INVASIVE ADENOCARCINOMA, INTESTINAL TYPE, moderately differentiated. - Gastric mucosa with intestinal metaplasia. Comment: The tumour stains as follows: POSITIVE: CK7, CDX2. NEGATIVE: CD20. HER2 testing has been ordered and will be reported as an addendum.
STOMACH, BIOPSY: - INVASIVE ADENOCARCINOMA, INTESTINAL TYPE, MODERATELY DIFFERENTIATED. - Gastric mucosa with moderate chronic active inflammation and extensive intestinal metaplasia. - Benign small bowel mucosa with erosions.
GASTRIC ULCER, BIOPSY: - INVASIVE ADENOCARCINOMA, INTESTINAL-TYPE, MODERATELY DIFFERENTIATED.
Diffuse type
STOMACH, BIOPSY: - INVASIVE ADENOCARCINOMA, DIFFUSE TYPE. COMMENT: A pankeratin immunostain demonstrates single (infiltrating) epithelial cells in the lamina propria.
Micro
The tumour consists of single cells with abundant foamy-appearing cytoplasm and eccentric nuclei with mild nuclear atypia.
Poorly differentiated
GASTRIC ULCER, BIOPSY: - INVASIVE ADENOCARCINOMA, POORLY-DIFFERENTIATED.
See also
References
- ↑ Duell, EJ.; Travier, N.; Lujan-Barroso, L.; Clavel-Chapelon, F.; Boutron-Ruault, MC.; Morois, S.; Palli, D.; Krogh, V. et al. (Nov 2011). "Alcohol consumption and gastric cancer risk in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort.". Am J Clin Nutr 94 (5): 1266-75. doi:10.3945/ajcn.111.012351. PMID 21993435.
- ↑ Rudloff, U. (2018). "Gastric adenocarcinoma and proximal polyposis of the stomach: diagnosis and clinical perspectives.". Clin Exp Gastroenterol 11: 447-459. doi:10.2147/CEG.S163227. PMID 30584346.
- ↑ Nomura, A.; Grove, JS.; Stemmermann, GN.; Severson, RK. (Nov 1990). "Cigarette smoking and stomach cancer.". Cancer Res 50 (21): 7084. PMID 2208177.
- ↑ LAUREN P (1965). "THE TWO HISTOLOGICAL MAIN TYPES OF GASTRIC CARCINOMA: DIFFUSE AND SO-CALLED INTESTINAL-TYPE CARCINOMA. AN ATTEMPT AT A HISTO-CLINICAL CLASSIFICATION". Acta Pathol Microbiol Scand 64: 31–49. PMID 14320675.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 823. ISBN 0-7216-0187-1.
- ↑ Yamagawa, H.; Onishi, T. (Sep 1989). "[A clinicopathological study of early gastric cancers with a diameter larger than five centimeters].". Gan No Rinsho 35 (10): 1114-8. PMID 2550682.
- ↑ Werling, RW.; Yaziji, H.; Bacchi, CE.; Gown, AM. (Mar 2003). "CDX2, a highly sensitive and specific marker of adenocarcinomas of intestinal origin: an immunohistochemical survey of 476 primary and metastatic carcinomas.". Am J Surg Pathol 27 (3): 303-10. PMID 12604886.
- ↑ Zali, MR.; Moaven, O.; Asadzadeh Aghdaee, H.; Ghafarzadegan, K.; Ahmadi, KJ.; Farzadnia, M.; Arabi, A.; Abbaszadegan, MR. (Jul 2009). "Clinicopathological significance of E-cadherin, β-catenin and p53 expression in gastric adenocarinoma.". J Res Med Sci 14 (4): 239-47. PMID 21772890.
- ↑ Romiti, A.; Di Rocco, R.; Milione, M.; Ruco, L.; Ziparo, V.; Zullo, A.; Duranti, E.; Sarcina, I. et al. (Jan 2012). "Somatostatin receptor subtype 2 A (SSTR2A) and HER2 expression in gastric adenocarcinoma.". Anticancer Res 32 (1): 115-9. PMID 22213295.
- ↑ 10.0 10.1 Deng, JY.; Liang, H. (Apr 2014). "Clinical significance of lymph node metastasis in gastric cancer.". World J Gastroenterol 20 (14): 3967-75. doi:10.3748/wjg.v20.i14.3967. PMID 24744586.