Difference between revisions of "Porocarcinoma"
Jump to navigation
Jump to search
(create) |
|||
| (18 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
{{ Infobox diagnosis | |||
| Name = {{PAGENAME}} | |||
| Image = Porocarcinoma - alt -- low mag.jpg | |||
| Width = | |||
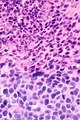
| Caption = Porocarcinoma. [[H&E stain]]. | |||
| Synonyms = | |||
| Micro = | |||
| Subtypes = | |||
| LMDDx = [[basal cell carcinoma]], [[squamous cell carcinoma of the skin|squamous cell carcinoma]], [[pyogenic granuloma]], [[verruca vulgaris]], | |||
[[adenocarcinoma]], [[malignant melanoma]] | |||
| Stains = | |||
| IHC = [[CD117]] +ve | |||
| EM = | |||
| Molecular = | |||
| IF = | |||
| Gross = | |||
| Grossing = | |||
| Staging = | |||
| Site = skin - typically head & neck | |||
| Assdx = | |||
| Syndromes = | |||
| Clinicalhx = | |||
| Signs = | |||
| Symptoms = | |||
| Prevalence = very rare | |||
| Bloodwork = | |||
| Rads = | |||
| Endoscopy = | |||
| Prognosis = poor | |||
| Other = | |||
| ClinDDx = | |||
| Tx = surgical excision | |||
}} | |||
'''Porocarcinoma''' is a rare [[malignant]] [[skin tumour]] that has an aggressive behaviour.<ref name=pmid28721214>{{Cite journal | last1 = Salih | first1 = AM. | last2 = Kakamad | first2 = FH. | last3 = Baba | first3 = HO. | last4 = Salih | first4 = RQ. | last5 = Hawbash | first5 = MR. | last6 = Mohammed | first6 = SH. | last7 = Othman | first7 = S. | last8 = Saeed | first8 = YA. | last9 = Habibullah | first9 = IJ. | title = Porocarcinoma; presentation and management, a meta-analysis of 453 cases. | journal = Ann Med Surg (Lond) | volume = 20 | issue = | pages = 74-79 | month = Aug | year = 2017 | doi = 10.1016/j.amsu.2017.06.027 | PMID = 28721214 }}</ref> | '''Porocarcinoma''' is a rare [[malignant]] [[skin tumour]] that has an aggressive behaviour.<ref name=pmid28721214>{{Cite journal | last1 = Salih | first1 = AM. | last2 = Kakamad | first2 = FH. | last3 = Baba | first3 = HO. | last4 = Salih | first4 = RQ. | last5 = Hawbash | first5 = MR. | last6 = Mohammed | first6 = SH. | last7 = Othman | first7 = S. | last8 = Saeed | first8 = YA. | last9 = Habibullah | first9 = IJ. | title = Porocarcinoma; presentation and management, a meta-analysis of 453 cases. | journal = Ann Med Surg (Lond) | volume = 20 | issue = | pages = 74-79 | month = Aug | year = 2017 | doi = 10.1016/j.amsu.2017.06.027 | PMID = 28721214 }}</ref> | ||
It is also known as '''eccrine porocarcinoma''' (abbreviated '''EPC''') and '''malignant eccrine poroma'''.<ref name=pmid20668633>{{Cite journal | last1 = Luz | first1 = Mde A. | last2 = Ogata | first2 = DC. | last3 = Montenegro | first3 = MF. | last4 = Biasi | first4 = LJ. | last5 = Ribeiro | first5 = LC. | title = Eccrine porocarcinoma (malignant eccrine poroma): a series of eight challenging cases. | journal = Clinics (Sao Paulo) | volume = 65 | issue = 7 | pages = 739-42 | month = Jul | year = 2010 | doi = 10.1590/S1807-59322010000700014 | PMID = 20668633 }}</ref> | |||
==General== | ==General== | ||
*Malignant counterpart of ''[[poroma]]''. | *Malignant counterpart of ''[[poroma]]''.<ref name=pmid28954110 >{{Cite journal | last1 = Abarzúa | first1 = Á. | last2 = Álvarez-Véliz | first2 = S. | last3 = Moll-Manzur | first3 = C. | title = Concomitant poroma and porocarcinoma. | journal = An Bras Dermatol | volume = 92 | issue = 4 | pages = 550-552 | month = | year = | doi = 10.1590/abd1806-4841.20175719 | PMID = 28954110 }}</ref> | ||
*Very rare ~ most papers are case reports.<ref name=pmid25515648>{{Cite journal | last1 = Riera-Leal | first1 = L. | last2 = Guevara-Gutiérrez | first2 = E. | last3 = Barrientos-García | first3 = JG. | last4 = Madrigal-Kasem | first4 = R. | last5 = Briseño-Rodríguez | first5 = G. | last6 = Tlacuilo-Parra | first6 = A. | title = Eccrine porocarcinoma: epidemiologic and histopathologic characteristics. | journal = Int J Dermatol | volume = 54 | issue = 5 | pages = 580-6 | month = | year = 2015 | doi = 10.1111/ijd.12714 | PMID = 25515648 }}</ref> | |||
Clinical - based on meta-analysis of 453 cases: | Clinical features - based on meta-analysis of 453 cases:<ref name=pmid28721214/> | ||
*No predominance males versus females. | *No predominance males versus females. | ||
*Aggressive behaviour >30% of cases have metastases at presentation - typically to lymph nodes. | |||
Treatment: | |||
*Surgery, | |||
==Gross== | ==Gross== | ||
*Mass or nodule - typically head and neck (40% of cases) or lower extremity (34% of cases).<ref name=pmid28721214/> | *Mass or nodule - typically head and neck (40% of cases) or lower extremity (34% of cases).<ref name=pmid28721214/> | ||
==Microscopic== | |||
Features: | |||
*Ductal/eccrine differentiation:<ref name=pmid20668633/> | |||
**Intracytoplasmic lumens. | |||
**Multicellular ducts with thin esoinophilic layer. | |||
**Lack granular cells and lack decapitated lumens - features of apocrine differentiation. | |||
*Features of malignancy:<ref name=pmid20668633/> | |||
**[[Desmoplastic stromal response]]. | |||
**Irregular dermis infiltrating cell clusters. | |||
*+/-Squamous differentiation. | |||
*+/-Basaloid differentiation. | |||
DDx:<ref name=pmid28954110/> | |||
*[[Basal cell carcinoma]]. | |||
*[[Squamous cell carcinoma of the skin|Squamous cell carcinoma]]. | |||
*[[Pyogenic granuloma]]. | |||
*[[Verruca vulgaris]]. | |||
*[[Adenocarcinoma]]. | |||
*[[Malignant melanoma]] - desmoplastic and nodular variants. | |||
===Images=== | |||
<gallery> | |||
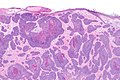
Image: Porocarcinoma -- very low mag.jpg | Porocarcinoma - very low mag. | |||
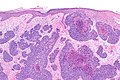
Image: Porocarcinoma -- low mag.jpg | Porocarcinoma - low mag. | |||
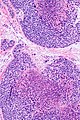
Image: Porocarcinoma -- intermed mag.jpg | Porocarcinoma - intermed. mag. | |||
Image: Porocarcinoma - alt -- intermed mag.jpg | Porocarcinoma - intermed. mag. | |||
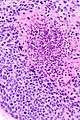
Image: Porocarcinoma -- high mag.jpg | Porocarcinoma - high mag. | |||
Image: Porocarcinoma -- very high mag.jpg | Porocarcinoma - very high mag. | |||
</gallery> | |||
====www==== | |||
*[https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5595608/figure/f4/?report=objectonly Eccrine porocarcinoma (nih.gov)].<ref name=pmid28954110/> | |||
*[https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3884174/figure/F2/ Porocarcinoma (nih.gov)].<ref name=pmid24403888>{{Cite journal | last1 = Kurashige | first1 = Y. | last2 = Minemura | first2 = T. | last3 = Nagatani | first3 = T. | title = Eccrine porocarcinoma: clinical and pathological report of eight cases. | journal = Case Rep Dermatol | volume = 5 | issue = 3 | pages = 259-66 | month = | year = 2013 | doi = 10.1159/000355606 | PMID = 24403888 }}</ref> | |||
==IHC== | |||
Features:<ref>{{Cite journal | last1 = Goto | first1 = K. | last2 = Takai | first2 = T. | last3 = Fukumoto | first3 = T. | last4 = Anan | first4 = T. | last5 = Kimura | first5 = T. | last6 = Ansai | first6 = S. | last7 = Oshitani | first7 = Y. | last8 = Murata | first8 = Y. | last9 = Sakuma | first9 = T. | title = CD117 (KIT) is a useful immunohistochemical marker for differentiating porocarcinoma from squamous cell carcinoma. | journal = J Cutan Pathol | volume = 43 | issue = 3 | pages = 219-26 | month = Mar | year = 2016 | doi = 10.1111/cup.12632 | PMID = 26449497 }}</ref> | |||
*[[CD117]] +ve (~100% of porocarcinoma, ~20% of [[squamous carcinoma]]s focally). | |||
==See also== | ==See also== | ||
| Line 20: | Line 96: | ||
[[Category:Diagnosis]] | [[Category:Diagnosis]] | ||
[[Category:Dermatopathology]] | |||
Latest revision as of 19:24, 8 February 2019
| Porocarcinoma | |
|---|---|
| Diagnosis in short | |
 Porocarcinoma. H&E stain. | |
| LM DDx |
basal cell carcinoma, squamous cell carcinoma, pyogenic granuloma, verruca vulgaris, adenocarcinoma, malignant melanoma |
| IHC | CD117 +ve |
| Site | skin - typically head & neck |
|
| |
| Prevalence | very rare |
| Prognosis | poor |
| Treatment | surgical excision |
Porocarcinoma is a rare malignant skin tumour that has an aggressive behaviour.[1]
It is also known as eccrine porocarcinoma (abbreviated EPC) and malignant eccrine poroma.[2]
General
Clinical features - based on meta-analysis of 453 cases:[1]
- No predominance males versus females.
- Aggressive behaviour >30% of cases have metastases at presentation - typically to lymph nodes.
Treatment:
- Surgery,
Gross
- Mass or nodule - typically head and neck (40% of cases) or lower extremity (34% of cases).[1]
Microscopic
Features:
- Ductal/eccrine differentiation:[2]
- Intracytoplasmic lumens.
- Multicellular ducts with thin esoinophilic layer.
- Lack granular cells and lack decapitated lumens - features of apocrine differentiation.
- Features of malignancy:[2]
- Desmoplastic stromal response.
- Irregular dermis infiltrating cell clusters.
- +/-Squamous differentiation.
- +/-Basaloid differentiation.
DDx:[3]
- Basal cell carcinoma.
- Squamous cell carcinoma.
- Pyogenic granuloma.
- Verruca vulgaris.
- Adenocarcinoma.
- Malignant melanoma - desmoplastic and nodular variants.
Images
Porocarcinoma - very low mag.
Porocarcinoma - low mag.

Porocarcinoma - intermed. mag.
Porocarcinoma - intermed. mag.
Porocarcinoma - high mag.
Porocarcinoma - very high mag.






www
IHC
Features:[6]
- CD117 +ve (~100% of porocarcinoma, ~20% of squamous carcinomas focally).
See also
References
- ↑ 1.0 1.1 1.2 Salih, AM.; Kakamad, FH.; Baba, HO.; Salih, RQ.; Hawbash, MR.; Mohammed, SH.; Othman, S.; Saeed, YA. et al. (Aug 2017). "Porocarcinoma; presentation and management, a meta-analysis of 453 cases.". Ann Med Surg (Lond) 20: 74-79. doi:10.1016/j.amsu.2017.06.027. PMID 28721214.
- ↑ 2.0 2.1 2.2 Luz, Mde A.; Ogata, DC.; Montenegro, MF.; Biasi, LJ.; Ribeiro, LC. (Jul 2010). "Eccrine porocarcinoma (malignant eccrine poroma): a series of eight challenging cases.". Clinics (Sao Paulo) 65 (7): 739-42. doi:10.1590/S1807-59322010000700014. PMID 20668633.
- ↑ 3.0 3.1 3.2 Abarzúa, Á.; Álvarez-Véliz, S.; Moll-Manzur, C.. "Concomitant poroma and porocarcinoma.". An Bras Dermatol 92 (4): 550-552. doi:10.1590/abd1806-4841.20175719. PMID 28954110.
- ↑ Riera-Leal, L.; Guevara-Gutiérrez, E.; Barrientos-García, JG.; Madrigal-Kasem, R.; Briseño-Rodríguez, G.; Tlacuilo-Parra, A. (2015). "Eccrine porocarcinoma: epidemiologic and histopathologic characteristics.". Int J Dermatol 54 (5): 580-6. doi:10.1111/ijd.12714. PMID 25515648.
- ↑ Kurashige, Y.; Minemura, T.; Nagatani, T. (2013). "Eccrine porocarcinoma: clinical and pathological report of eight cases.". Case Rep Dermatol 5 (3): 259-66. doi:10.1159/000355606. PMID 24403888.
- ↑ Goto, K.; Takai, T.; Fukumoto, T.; Anan, T.; Kimura, T.; Ansai, S.; Oshitani, Y.; Murata, Y. et al. (Mar 2016). "CD117 (KIT) is a useful immunohistochemical marker for differentiating porocarcinoma from squamous cell carcinoma.". J Cutan Pathol 43 (3): 219-26. doi:10.1111/cup.12632. PMID 26449497.