Difference between revisions of "Penis"
(→Images) |
|||
| Line 42: | Line 42: | ||
===Pre-cancerous=== | ===Pre-cancerous=== | ||
*Penile intraepithelial neoplasia ( | *[[Penile intraepithelial neoplasia]] (PeIN). | ||
*Paget disease (like [[extramammary Paget disease]]). (???) | *Paget disease (like [[extramammary Paget disease]]). (???) | ||
Revision as of 07:04, 9 February 2015
The penis is occasionally afflicted by disease that the pathologist sees
It is afflicted by common skin pathologies.
Normal
- Corpus spongiosum - fills with blood during erection.[1]
- Corpus cavernosum - around the urethra.
Image

Cross section of penis. (WC)

Diseases
Inflammatory
- Phimosis.
- Paraphimosis.
- Balanoposthitis.
- Balanatis.
- Plasma cell balanitis.
- Balanitis xerotica obliterans.
- Balanitis circinata.
- Lipogranulomas.
Infectious
- HPV infection.
- HSV infection.
- Scabies.
- Pediculosis pubis.
- Syphilis.
- Gonorrhea.
- Lymphogranuloma venereum.
- Granuloma inguinale.
- Chancroid.
- Molluscum contagiosum.
- Filariasis - elephantiasis.
Other non-tumour
- Idiopathic scrotal calcinosis.
- Melanocytic lesions, esp. nevi.
- Fordyce spots.
Pre-cancerous
- Penile intraepithelial neoplasia (PeIN).
- Paget disease (like extramammary Paget disease). (???)
Neoplastic
- Squamous cell carcinoma.
- Merkel cell carcinoma.
- Sebaceous carcinoma.
- Clear cell carcinoma.
- Basal cell carcinoma.
- Melanoma.
Others:
- Mesenchymal lesions - see: soft tissue lesions.
- Hematopoetic, e.g. lymphoma.
- Metastasis.
Specific conditions
Phimosis
General
- Cannot retract foreskin.
- This is a clinical diagnosis.
Microscopic
Features:[2]
- +/-Inflammation.
- Fibrosis.
Notes: Findings non-specific.
DDx - general:
- Squamous cell carcinoma - nuclear atypia.
- Lichen sclerosus - supeficial dermal fibrosis with thinned epidermis.
- Lichen planus - interface dermatitis with apoptotic bodies.
- Infection.
- Syphilis - plasma cells.
- Candidiasis.
- Zoon balanitis - plasma cells.
Sign out
FORESKIN, CIRCUMCISION: - SKIN WITH PATCHY MILD NONSPECIFIC INFLAMMATION. - NEGATIVE FOR DYSPLASIA AND NEGATIVE FOR MALIGNANCY.
FORESKIN, EXCISION: - KERATINIZED SQUAMOUS EPITHELIUM WITH PATCHY MILD NON-SPECIFIC SUBEPITHELIAL INFLAMMATION. - NEGATIVE FOR MALIGNANCY.
FORESKIN, CIRCUMCISION: - BENIGN KERATINIZED SQUAMOUS EPITHELIUM. - MILDLY FIBROUS SUBEPITHELIAL TISSUE WITH MINIMAL PATCHY NONSPECIFIC INFLAMMATION. - NEGATIVE FOR DYSPLASIA AND NEGATIVE FOR MALIGNANCY.
Micro
The sections show skin with mild patchy chronic inflammation, consisting predominantly of lymphocytes, at the dermal-epidermal junction. The epidermis matures to the surface, has rete ridges and is of a normal thickness. Focally, parakeratosis is present. No significant nuclear atypia is identified.
Thinned epidermis
The sections show skin with mild patchy chronic inflammation, consisting predominantly of lymphocytes, at the dermal-epidermal junction. Eosinophils are not readily apparent.
The epidermis matures to the surface; however, it is thinned and focally flattened appearing. No hyperkeratosis or parakeratosis is apparent. The superficial dermis is minimally hyalinized focally. No significant nuclear atypia is identified.
Alternate
The sections show skin with mild patchy chronic inflammation, consisting predominantly of lymphocytes, at the dermal-epidermal junction. Eosinophils are not readily apparent. The epidermis matures to the surface; however, it is focally thinned and focally flattened. No significant hyperkeratosis or parakeratosis is apparent. The superficial dermis shows no apparent fibrosis. No significant nuclear atypia is identified.
Penile fibromatosis
- AKA Peyronie's disease.
General
- Prevalence ~5%.[3]
Treatment:
- Conservative versus surgery.
Gross
- Abnormal curvature of the penis, esp. in the erect state.
Microscopic
Features:[3]
- Tunica albuginea fibrosis.
Zoon balanitis
General
- Balanitis = inflammation of glands penis.
- Rare.
- Uncircumsized men.[6]
- Analogous to plasma cell vulvitis in women.
Treatment:[6]
- Circumcision.
- Corticosteroids.
Microscopic
Features:[4]
- Abundant plasma cells - key feature.
- Dermal atrophy.
- Spongiosis and intraepithelial lymphocytes.
- Tortuosity dermal blood vessels.
DDx:
- Syphilis - plasma cell-rich infiltrate.
- Balanitis xerotica obliterans.
Images
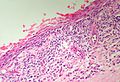
Note the flattened 'lozenge' keratinocytes separated by spongiosis (SKB).
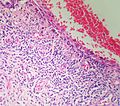
The epidermis is very atrophic in this example but shows 'lozenge' keratinocytes and spongiosis (SKB).
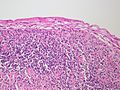
This example might at first glance appear to be a lichenoid balanitis but the thin layer of epidermis is actually intact (SKB).



Sign out
PENILE FORESKIN, CIRCUMCISION: - COMPATIBLE WITH PLASMA CELL BALANITIS (ZOON BALANITIS), SEE COMMENT. COMMENT: A treponemal infection should be considered clinically.
Squamous cell carcinoma of the penis
See also
References
- ↑ Zhang, XH.; Melman, A.; Disanto, ME. (Jul 2011). "Update on corpus cavernosum smooth muscle contractile pathways in erectile function: a role for testosterone?". J Sex Med 8 (7): 1865-79. doi:10.1111/j.1743-6109.2011.02218.x. PMID 21324096.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 391. ISBN 978-0781765275.
- ↑ 3.0 3.1 Serefoglu, EC.; Hellstrom, WJ. (Dec 2011). "Treatment of Peyronie's disease: 2012 update.". Curr Urol Rep 12 (6): 444-52. doi:10.1007/s11934-011-0212-2. PMID 21818660.
- ↑ 4.0 4.1 4.2 Balato, N.; Scalvenzi, M.; La Bella, S.; Di Costanzo, L. (2009). "Zoon's Balanitis: Benign or Premalignant Lesion?". Case Rep Dermatol 1 (1): 7-10. doi:10.1159/000210440. PMID 20652106.
- ↑ Korenaga, D.; Kanematsu, T.; Watanabe, A.; Maehara, Y.; Kitano, S.; Sugimachi, K. (Feb 1991). "Clinical management of gastric cancer and concomitant esophagogastric varices.". J Surg Oncol 46 (2): 91-6. PMID 1992223.
- ↑ 6.0 6.1 Yoganathan, S.; Bohl, TG.; Mason, G. (Dec 1994). "Plasma cell balanitis and vulvitis (of Zoon). A study of 10 cases.". J Reprod Med 39 (12): 939-44. PMID 7884748.