Ovary
The ovary has a wealth of pathology. It has benign tumours and malignant ones. It is a significant part of gynecologic pathology.
Normal ovary
- Corpora albicans - pale/white body with lobulated contour.
- Involuted corpus luteum.
- Not seen pre-pubertal.
- Number increase with age.
- Ovarian follicles.
- Stroma - hyperchromatic - spindle morphology, whorling.
- If the cells have a round morphology... think about endometriosis.
Images
www:
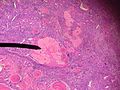
Corpus albicans. (WC)

{kind=link}
Cysts - overview
General
- Very common.
Most common:
- Serous cystadenoma.
- Usually uniloculated.
- Morphology: ciliated, columnar.
- Mucinous cystadenoma.
- Usually multiloculated.[1]
- Memory device: multiloculated = mucinous.
- Usually multiloculated.[1]
- Endometrioma (see endometriosis).
- Simple cyst.
- Corpus luteum cyst.
- Cancerous cyst (see ovarian cancer).
Notes:
- Epithelium is often lost in processing - may make interpretation challenging
- Ovarian surface epithelium (previously call germinal epithelium) - covers the ovary
Ovarian surface vs. mesothelium:
- Image: ovarian surface epithelium - endojournals.org.
- Image: mesothelium - internetattitude.com.
{kind=link}
Specific benign diagnoses
Endometriosis
Main article: Endometriosis
Corpus luteum cyst
General
- Normal in childbearing age women.
Gross
- Classically yellow.
Microscopic
Features:
- Pseudocyst lined by stratified, pale staining (luteinized) cells.
- +/-Hemorrhagic centre.
Images:
{kind=link}
{kind=link}
Benign mesothelial inclusion cyst
- AKA mesothelial inclusion cyst.
- AKA peritoneal inclusion cyst.[citation needed]
- AKA cortical inclusion cyst.[4][citation needed]
General
- May be found incidentally, e.g. during C-section.
Epidemiology:
- Associated with previous surgery.
Gross
Microscopic
Features:
- Benign mesothelium.
- Single layer of squamoid or cuboid mesothelial cells.[6]
DDx:
Image:
IHC
- CK +ve, calretinin +ve.[6]
Sign out
OVARY, LEFT, BIOPSY: - BENIGN CORTICAL INCLUSION CYST.
Ovarian infarct
Main article: Ovarian infarct
Pregnancy luteoma
General
- Tumour of pregnancy.
- Benign.
- Regress after pregnancy; thus, conservative management.[8]
Clinical:
Gross
- Solid.
- Yellow.
Images:
Microscopic
Features:
- Sheets of cells.
- Cells with eosinophilic cytoplasm, round nuclei and prominent nucleoli.
DDx:
Images
IHC
- Inhibin +ve.[11]
Ovarian tumours
Main article: Ovarian tumours
For a very brief overview of gynecologic tumours see: Gynecologic pathology.
See also
References
- ↑ IAV. 6 February 2009.
- ↑ Auersperg N, Wong AS, Choi KC, Kang SK, Leung PC (April 2001). "Ovarian surface epithelium: biology, endocrinology, and pathology". Endocr. Rev. 22 (2): 255–88. PMID 11294827. http://edrv.endojournals.org/cgi/pmidlookup?view=long&pmid=11294827.
- ↑ ALS. 5 February 2009.
- ↑ Feeley, KM.; Wells, M. (Feb 2001). "Precursor lesions of ovarian epithelial malignancy.". Histopathology 38 (2): 87-95. PMID 11207821.
- ↑ GAG 26 Feb 2009.
- ↑ 6.0 6.1 6.2 Urbanczyk K, Skotniczny K, Kucinski J, Friediger J (2005). "Mesothelial inclusion cysts (so-called benign cystic mesothelioma)--a clinicopathological analysis of six cases". Pol J Pathol 56 (2): 81-7. PMID 16092670.
- ↑ Asch, E.; Levine, D.; Kim, Y.; Hecht, JL. (Mar 2008). "Histologic, surgical, and imaging correlations of adnexal masses.". J Ultrasound Med 27 (3): 327-42. PMID 18314510.
- ↑ Masarie, K.; Katz, V.; Balderston, K. (Sep 2010). "Pregnancy luteomas: clinical presentations and management strategies.". Obstet Gynecol Surv 65 (9): 575-82. doi:10.1097/OGX.0b013e3181f8c41d. PMID 21144088.
- ↑ Kao, HW.; Wu, CJ.; Chung, KT.; Wang, SR.; Chen, CY.. "MR imaging of pregnancy luteoma: a case report and correlation with the clinical features.". Korean J Radiol 6 (1): 44-6. PMID 15782020.
- ↑ Rodriguez, M.; Harrison, TA.; Nowacki, MR.; Saltzman, AK. (Nov 1999). "Luteoma of pregnancy presenting with massive ascites and markedly elevated CA 125.". Obstet Gynecol 94 (5 Pt 2): 854. PMID 10546765.
- ↑ 11.0 11.1 Wang, Y.; Zhou, F.; Qin, JL.; Qian, ZD.; Huang, LL. (2015). "Pregnancy luteoma followed with massive ascites and elevated CA125 after ovulation induction therapy: a case report and review of literatures.". Int J Clin Exp Med 8 (1): 1491-3. PMID 25785161.